
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare case of multiple autoimmune syndrome
after sars-cov2 infection
Marta Graziadei; Jennifer Nardella; Chiara Sorrento; Anna Pia Volini; Carlo Sabba; Antonio Perrone*
DIM- Interdisciplinary Department of Medicine, Internal Medicine Unit, “Cesare Frugoni”, University of Bari “Aldo Moro” School of Medicine, Poli-clinico Hospital, Bari, Italy.
*Corresponding Author : Antonio Perrone
DIM – Interdisciplinary Department of Medicine, Internal Medicine Unit “Cesare Frugoni”, University of Bari “Aldo Moro” School of Medicine, Policlinico Hospital, 70124 Bari (BA), Italy.
Email: antonio.perrone@uniba.it
Received : Sep 13, 2022
Accepted : Oct 11, 2022
Published : Oct 18, 2022
Archived : www.jcimcr.org
Copyright : © Perrone A (2022).
Abstract
Mixed Connective Tissue Disease (MCTD) is a complex clinical entity, which includes features of Systemic Lupus Erythematosus (SLE), Rheumatoid Arthritis (RA), Systemic Sclerosis (SSc) and Polymyositis/Dermatomyositis (PM/DM), along with the presence of a distinctive antibody, anti-U1-Ribonucleoprotein (RNP). Autoimmune hepatitis is a chronic inflammatory disease of the liver. It is characterized by increase in transaminase and immunoglobulin G levels, the presence of autoantibodies, and portal inflammatory infiltrate with interface hepatitis at liver biopsy. Primary biliary cholangitis is a chronic inflammatory autoimmune liver disease that is characterized by a positive antimitochondrial antibodies test and consequent progressive destruction of the small intrahepatic bile duct. Many reports have confirmed the development of autoimmune diseases after SARS-CoV-2 infection.Here we report the case of a 64-year-old woman, with a positive medical history for SARS-CoV2 infection, who was admitted to our Internal Medicine Unit “Cesare Frugoni”, Policlinico Hospital, Bari, in January 2022, and diagnosed with an extremely rare Multiple Autoimmune Syndrome (MAS), consisting in Mixed connective tissue disease, autoimmune hepatitisand primary biliary cholangitis.
Keywords: Multiple autoimmune syndrome; Mixed connective tissue disease; Autoimmune hepatitis; Primary biliary cholangitis.
Citation: Graziadei M, Nardella J, Sorrento C, Volini AP, Perrone A, et al. A rare case of multiple autoimmune syndrome after sars-cov2 infection. J Clin Images Med Case Rep. 2022; 3(10): 2108.
Introduction
Mixed Connective Tissue Disease (MTCD) is an uncommon systemic inflammatory rheumatic condition, that represents a specific subset of the broader category of rheumatic “overlap syndromes”, a term used to describe the collection of features of more than one classic inflammatory rheumatic disease in a patient’s clinical display, including systemic lupus erythematosus, polymyositis, scleroderma and rheumatoid arthritis [1]. MCTD patients have rheumatic overlap syndrome along with the presence of a distinctive type of antibody, the anti-U1-Ribonucleoprotein (RNP). The etiology of MCTD is unclear. Exposure to viral infections has shown to be linked to an increased risk of developing this uncommon display of autoimmune conditions through the phenomenon of antigen mimicry. Additional underlining risk factors for developing MCTD might be hereditary conditions and environmental related risks [2].
Autoimmune Hepatitis (AIH) is a rare disease thought to be due to a lack of self-tolerance ultimately leading to liver injury and, in some cases, cirrhosis or acute liver failure. The diagnosis requires exclusion of other etiologies and is multilayered, consisting of specific histological abnormalities with elevated liver enzymes, IgG levels, and one or more associated autoantibodies including Antinuclear Antibody (ANA) and Smooth Muscle Antibodies (SMA). Rarely Antibodies Against Microsome Type 1 (anti-LKM1) and Soluble Liver Antigen (SLA) might also be detected [3].
Primary Biliary Cholangitis (PBC) is a rare disease of the small intrahepatic bile ducts. The principal characteristics of PBC are cholestasis, serum detection of Anti-Mitochondrial (AMA), or PBC-specific Antinuclear (ANA) antibodies positivity and histological evidence of chronic, granulomatous, lymphocytic small bile duct cholangitis [4].
Autoimmune diseases are chronic conditions that are initiated by the loss of immunological tolerance to self-antigens, forming a heterogeneous group of disorders in which multiple alterations in the immune system result in a spectrum of syndromes that either target specific organs or affect the body systemically. Coexistence of Autoimmune Diseases (AIDs) in a single person is largely described in literature [5].
Viral infections are known to play a significant role in the development of autoimmune phenomena in patients with impaired immune regulation. There has been growing interest in the development of autoimmune phenomena following COVID-19 infection. This includes both the development of new autoimmune diseases as well as the exacerbation of previously diagnosed diseases [6].
The present paper describes the case of newly diagnosed MCTD in combination with AIH and PBC in a PCR-confirmed COVID-19 patient.

Case presentation
A 64-years-old woman was admitted to Internal Medicine Unit “Cesare Frugoni”, Policlinico Hospital, Bari, in January 2022, complaining of fatigue, hand tremors, dark urine and muscle weakness involving proximal muscles of the trunk, particularly shoulders and upper arms. The physical examination showed dark red itchy rash on her cheeks, eyelids, knuckles, knees, chest and back. Moreover she presented swollen fingers, periungual telangiectasias and a light scleral jaundice (Figure 1). She denied assumption of alcohol and previous of blood transfusions. She reported a positive family history for autoimmune disorders (mother affected by RA). In February 2021 she was hospitalized for Covid19-related acute respiratory failure. She was then discharged at home in improved clinical conditions.
She was admitted to our department because of the laboratory finding of hypertransaminasemia at blood tests performed after an episode of vomiting.
The laboratory data obtained included: ESR 21 mm/hour (n.v. 1-20 mm/h), normal HB, WBC and PLT counts, serum gammaglobulin fraction 2.20 g/dL (37.3%; n.v. 11.1-18.8%), GOT 414U/L (n.v. 15-37 U/L), GPT 773 U/L (12-78 U/L), ALP 169U/L (n.v. 43-115 U/L), total bilirubine 5 mg/dL (n.v. 0.20-1 mg/dL; conjugated 3.66 mg/dL), gamma-GT 326 U/L (n.v.5-55 U/L), hypocomplementemia. In addition, elevated CPK, myoglobin and LDH values were detected (CPK 1401 U/L, myoglobin 231 ng/mL, LDH 813 U/L).
The antibody panel confirmed ANA positivity (1:2560) and anti-double stranded DNA positivity as well as evidence of antiU1 ribonucleoprotein (17.5 CU/mL v.n.< 10), Sp100 nuclear antigen and anti-Ro52 antibodiespositivity.
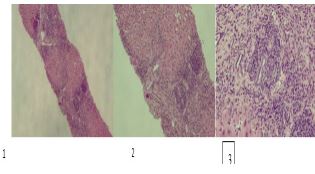
A diagnosis of autoimmune hepatitis type I was made based on the detection of a significant antibody titer for ANA(>1/2560) and on the results of echo-guided liver biopsy, which showed advanced immune inflammation with lymphomonocyte and plasma cell (MUM1+) infiltration, associated to necrosis of limiting plate and ductular cell neogenesis (CK7+). Moreover, liver specimen showed a moderate portal inflammation with abundant lymphoplasma cells detection and mild bile duct damage with lymphocytic cholangitis, consistent with a diagnosis of Primary biliary cholangitis (Figure 2).
Serum antibodies for hepatitis related viral infections and antibodies against CMV and EBV testing yielded negative results. The RA-test for rheumatoid factor and antiphospholipid antibodies were within the normal range.
Both Computed Tomographic (CT) scan and Magnetic Resonance Image (MRI) were performed, showing enlarged disomogeneus liver with several regeneration nodules.
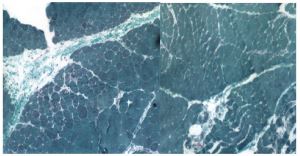
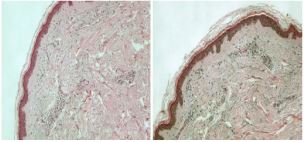
The Electromyography showed signs of myogenic suffering of the left deltoid. Muscolar biopsy was performed on the opposite deltoid, detecting myogenic and neurogenic suffering (Figure 3). Moreover punch biopsy on skin lesion showed epidermal atrophy and mild dermal fibrosis with sign of angiogenesis and perivascular chronic lymphocytic inflammatory infiltration (Figure 4).
Based on antibody pattern, clinical and laboratory findings, a diagnosis of Mixed Connective Tissue Disease was made.
Discussion
Autoimmune diseases are chronic conditions that occur because of loss of immunological tolerance to self-antigens. The etiologyis still unclear, but a combination of genetic, immunological, environmental, and hormonal factors is believed to play an important role in their development [7]. AIH and PBC are two individual autoimmune disorders, that may occur simultaneously or sequentially in 10–20%. Patients with pure or combined AIH/PBC may also present with other organ-specific or systemic autoimmune diseases [8]. The liver is frequently involved in Connective Tissue Diseases (CTD), most commonly in the form of liver function tests related biochemical changes with predominant cholestatic or hepatocellular patterns. CTD commonly affecting the liver include systemic lupus erythematosus, antiphospholypid syndrome, primary Sjögren’s syndrome, systemic sclerosis, dermatomyositis, polimyositis, and antisynthetase syndrome, although overlap syndromes between AILD and CTD may also be diagnosed [9]. The association between mixed connective tissue diseases and AIH seems to be really rare [10-14], and even more the concomitant presence of MCTD and PBC. The peculiar clinical picture presented by the patient lead us to the writing of this case report. Moreover, timing and clinical features of the patient (i.e. older age, disease free medical history) suggest that the development of these autoimmune disease may be consequent to Covid19 infection. Since the beginning of the COVID-19 pandemic, SARS-CoV-2 ability to induce auto-antibodies production and autoimmune clinical manifestations has been observed in multiple studies [15-17].
As suggested for other viruses, the widespread interaction of Coronaviruses with our immune system can trigger autoimmune diseases favored by a molecular mimicry between viral and human peptides. Their sporadic transcription and recombination generate a wide number of epitopes that may contribute to elicit autoimmunity trough the phenomenon of molecular mimicry, bystander activation, epitope spreading and cytokine storm [18]. Acute hemolytic anemia, macrophage activating syndrome, Guillain-Barre syndrome (GBS), autoimmune thrombotic thrombocytopenic purpura, autoimmune skin manifestations, and autoimmune thyroid diseases are some of the most represented autoimmune diseases connected to COVID-19 infection [19,20].
Development of autoimmune liver disease seems to be more frequently associated to COVID-19 vaccine [21], rather then to CoVID-19 infection [22,23]. A possible relationship between COVID-19 and rheumatic autoimmune diseases such as SLE has also been recently documented [24-26]. However, there is a lack of data and knowledge on MCTD in COVID-19 positive patients [27]. Given these clinical evidences it is interesting to note how rare it is to find the combination of the three AIDs, underlying the connection with a previous Covid-19 infection. In conclusion, it may be assumed that this case is a very rare combination of MCTD, AIH and PBC following Covid-19 infection.
References
- https://rarediseases.org/rare-diseases/mixed-connective-tissue-disease-mctd/
- Sapkota B, Al Khalili Y. Mixed Connective Tissue Disease. 2022 May. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 31194355.
- Harrington C, Krishnan S, Mack CL, Cravedi P, Assis DN, Levitsky J, et al. Non-Invasive Biomarkers for the Diagnosis and Management of Autoimmune Hepatitis. Hepatology. 2022.
- Gerussi A, Paraboschi EM, Cappadona C, Caime C, Binatti E, et al. The Role of Epigenetics in Primary Biliary Cholangitis. Int J Mol Sci. 2022; 23: 4873.
- Anaya, Juan Manuel, Corena, Rodrigo, Castiblanco John, Rojas Villarraga Adriana, Shoenfeld Yehuda et al. The kaleidoscope of autoimmunity: Multiple autoimmune syndromes and familial autoimmunity. Expert Review of Clinical Immunology. 2007; 3: 623–635.
- Gustine JN, Jones D: Immunopathology of hyperinflammation in COVID-19. Am J Pathol. 2021; 191: 4-17. 10.1016/j.ajpath.2020.08.009
- Jörg S, Grohme DA, Erzler M, Binsfeld M, Haghikia A, et al. Environmental factors in autoimmune diseases and their role in multiple sclerosis. Cell Mol Life Sci. 2016; 73: 4611-4622.
- Efe C, Wahlin S, Ozaslan E, Berlot AH, Purnak T, Muratori L, et al. Autoimmune hepatitis/primary biliary cirrhosis overlap syndrome and associated extrahepatic autoimmune diseases. Eur J Gastroenterol Hepatol. 2012; 24: 531-534.
- De Santis Maria, Crotti Chiara, Selmi Carlo, et al. Liver abnormalities in connective tissue diseases. Best Practice & Research Clinical Gastroenterology. 2013; 27: 543–551.
- Tomsic M, Ferlan-Marolt V, Kveder T, Hojker S, Rozman B, et al. Mixed connective tissue disease associated with autoimmune hepatitis and thyroiditis. Ann Rheum Dis. 1992; 51: 544–546.
- Marshall JB, Ravendhran N, Sharp GC, et al. Liver disease in mixed connective tissue disease. Arch Intern Med. 1983; 143: 1817–1818.
- Rolny P, Goobar J, Zettergren L. HBsAg-negative chronic active hepatitis and mixed connective tissue disease syndrome. An unusual association observed in two patients. Acta Med Scand. 1984; 215: 391–395.
- Maeda M, Kanayama M, Hasumura Y, Takeuchi J, Uchida T, et al. Case of mixed connective tissue disease associated with autoimmune hepatitis. Dig Dis Sci. 1988; 33: 1487–1490.
- Wada T, Motoo Y, Ohmizo R, Terada T, Nakanuma Y, et al. Association of mixed connective tissue disease, Sjögren’s syndrome and autoimmune hepatitis: Report of a case. Jpn J Med. 1991; 30: 278–280.
- Vojdani A, Kharrazian D. Potential Antigenic Cross-Reactivity Between SARS-Cov-2 and Human Tissue With a Possible Link to an Increase in Autoimmune Diseases. Clin Immunol. 2020; 217: 108480.
- Liu, Yu, et al. “COVID-19 and autoimmune diseases.” Current opinion in rheumatology. 2021; 33: 155-162.
- Caso F, Costa L, Ruscitti P, Navarini L, Del Puente A, et al. Could Sars-Coronavirus-2 Trigger Autoimmune and/or Autoinflammatory Mechanisms in Genetically Predisposed Subjects? Autoimmun. Rev. 2020; 19: 102524.[CrossRef]
- Luchetti Gentiloni MM, Paci V, Marconi V, Gigli M, Benfaremo D, et al. 2022; SARS-COV-2 Infection, Vaccination, and Immune-Mediated Diseases: Results of a Single-Center Retrospective Study. Front. Immunol. 13: 859550.
- Yazdanpanah N, Rezaei N. Autoimmune complications of COVID-19. J Med Virol. 2022; 94: 54-62.
- Nardella J, Comitangelo D, Marino R, Malcangi G, Barratta MD, et al. Acquired Hemophilia A After SARS-CoV-2 Infection: A Case Report. J Med Cases. 2022; 13: 197-201.
- Chen Y, Xu Z, Wang P, Li XM, Shuai ZW, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022; 165: 386-401.
- Bartoli A, Gitto S, Sighinolfi P, Cursaro C, Andreone P, et al. Primary Biliary Cholangitis Associated with SARS-CoV-2 Infection. J. Hepatol. 2021; 74: 1245–1246. [Cross Ref]
- Singh B, Kaur P. Michael Maroules Autoimmune Hepatitis–Primary Biliary Cholangitis Overlap Syndrome Triggered by COVID-19. Eur. J. Case Rep. Intern. Med. 2021; 8. [Cross Ref]
- Joo YB, Lim YH, Kim KJ, Park KS, Park YJ, et al. Respiratory viral infections and the risk of rheumatoid arthritis, Arthritis Res. Ther. 2019; 21: 199. https://doi.org/10.1186/s13075-019-1977-9.
- Gartshteyn Y, Askanase AD, Schmidt NM, et al. COVID-19 and systemic lupuserythematosus: a case series, Lancet Rheumatol. 2020; 2: e452–e454. https://doi.org/10.1016/S2665-9913(20)30161-2.
- Khalid M, Rogers S, Fatima A, et al. July 02, A flare of systemic lupuserythematosus disease after COVID-19 infection: a case of lupus cerebritis, Cureus. 2021; 13: e16104, https://doi.org/10.7759/cureus.16104.
- Ali S, Almas T, Zaidi U, Ahmed F, Shaikh S, et al. A novel case of lupus nephritis and mixed connective tissue disorder in a COVID-19 patient. Ann Med Surg (Lond). 2022; 78: 103653.