
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
False hypoperfusion detected by RAPID
software due to status epilepticus
Daniel Vázquez Justes1*; Miriam Paul Arias1; Mariona Baraldés Rovira; Eugènia Saureu Rufach; Raquel Mitjana2
1Neurology Department, Hospital UniversitariArnau Vilanova, Lleida, Spain.
2Radiology Department, Diagnostic Institute (IDI), Hospital UniversitariArnau Vilanova, Lleida, Spain.
*Corresponding Author : Daniel Vázquez-Juste
Neurology Department, Hospital Universitari Arnau Vilanova, Lleida, Spain.
Email: danivazkez@gmail.com
Received : Sep 14, 2022
Accepted : Oct 11, 2022
Published : Oct 18, 2022
Archived : www.jcimcr.org
Copyright : © Justes DV (2022).
Abstract
Introduction: Automated CT Perfusion (CTP) has become an essential decision-making tool for treatment decision in the extended-time window of acute ischemic stroke. But its interpretation can be challenging. Making a correct diagnosis requires a good clinical examination, in conjunction with neuroimaging.
Case report: We present a case of an 85-year-old patient who presented a seizure in the emergency room, followed by a left hemiplegia, language impairment and left gaze deviation. Stroke code protocol was performed, and RAPID software showed left hemisphere hypoperfusion. Detailed examination showed right hemisphere hyperperfusion with decreased Tmax in the left hemisphere. Active seizures were suspected, and an electroencephalogram was performed, which confirmed Non-convulsive status epilepticus from the right side.
Conclusion: RAPID software should be interpreted cautiously. Clinical examination is essential, in order to not misdiagnose ischemic stroke in cases of images suggestive of hypoperfusion.
Keywords: CT perfusion; Status epilepticus; Stroke mimic.
Citation: Justes DV, Arias MP, Rovira MB, Rufach ES, Mitjana R, et al. False hypoperfusion detected by RAPID software due to status epilepticus. J Clin Images Med Case Rep. 2022; 3(10): 2109.
Introduction
Automated CT perfusion (CTP) has become an essential decision-making tool for treatment decision in the extended-time window of acute ischemic stroke. It allows to identify those patients beyond the 4.5-hour window for use of intravenous tissue Plasminogen Activator (tPA) and those beyond 6 hours who should have thrombectomy [1,2]. The trials which have extended the treatment window have used the RAPID automated CTP (iSchema View) in order to quantify core infarct (as non-salvageable tissue) and the penumbra (potentially salvageable). CTP also reveals information which could aid in the differential diagnosis of stroke, being useful in conditions like migraine or seizures. However, CTP and RAPID should be interpreted cautiously, in order to avoid pitfalls. Clinical information is essential in order to avoid misdiagnosis.
Case report
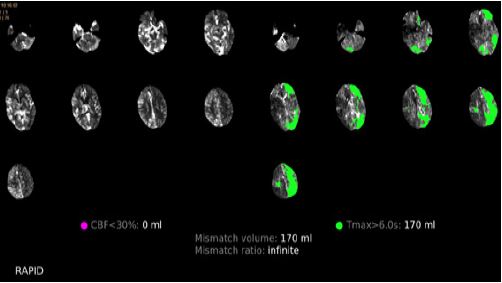
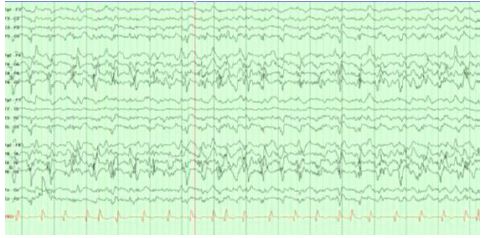
An 85-year-old man was admitted to the emergency room with COVID pneumonia. He had no past history of epilepsy. In the emergency room, the patient suffered a generalized tonic-clonic seizure. After the seizure, the patient´s examination showed somnolence, left hemiplegia, oculocephalic deviation to the left, and severe language impairment. At that point, there was no evident motor activity.Given the possibility of ischemic stroke, a multimodal CT scan was performed. On CTP (Figure 1), RAPID software showed 170 milliliters of prolonged time-to-peak concentration (Tmax) in the left hemisphere, involving several vascular territories (Figure 1). Qualitative visual analysis revealed a pattern of cerebral hyperperfusion in the right hemisphere (Figure 2). Given the possibility of Non-Convulsive Status Epilepticus (NCSE), an electroencephalogram was performed, which confirmed focal NCSE of the right hemisphere (Figure 3).
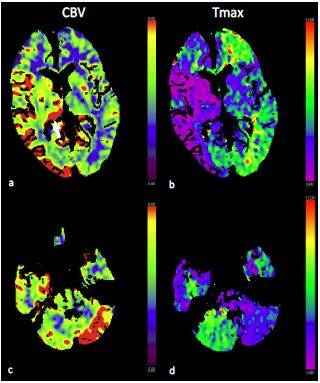
There was also increased perfusion in the right pulvinar nuclei (Figure 2) and in the left cerebellar hemisphere (cerebellar diaschisis).
Discussion
We present a case of left hemiparesis due to NCSE from the right hemisphere. There are several features to be remarked in this case. First, the neurological examination was of left hemiplegia, but with oculocephalic deviation to the left, which was consistently with epileptic onset. If hemiplegia had been of vascular origin, the presumptive oculocephalic deviation should have been to the contralateral side to the plegia. Moreover, the patient had had an epileptic seizure, so we could not exclude the possibility of a stroke manifesting as symptomatic seizure. The other remarkable feature was the prolonged Tmax detected with RAPID software in the left hemisphere, initially, this prolongation could have lead to suspicion of ischemic stroke, but the side affected was not consistent with expected as per clinical examination, which should have been the right in the case of stroke. The qualitative analysis revealed the pattern of hyperperfusion of the right hemisphere, and the EEG revealed focal right hemisphere NCSE. We therefore considered increasing Tmax in the left hemisphere was probably due to contralateral cerebral blood steal phenomena. Finally, the cerebellar diaschisis observed in this case has been previously reported in patients with NCSE [3].
Conclusion
The results of CTP and RAPID software should be interpreted with caution due to the possibility of stroke mimic. Hypoperfusion could be misdiagnosed in CTP due to contra lateral hyperperfusion.
References
- Ma H, Campbell BCV, Parsons MW, Churilov L, Levi CR, et al. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. N Engl J Med. 2019; 380: 1795-1803.
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, et al. DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med. 2018; 378: 11-21.
- Won J, Choi DS, Hong SJ, Shin HS, Baek HJ, et al. Crossed cerebellar hyperperfusion in patients with seizure-related cerebral cortical lesions: An evaluation with arterial spin labelling perfusion MR imaging. Radiol Med. 2018; 123: 843-850.