
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Recurrent stroke associated with brain metastasis due
to a cardioembolism secondary to left atrial Sarcoma:
Case presentation and review of the literature
García Villa Marcela1; Rafael Padron-Davalos2; Villarreal Careaga Jorge3; Ramon Ahahir Madrigal Cázarez4; Rodríguez Leyva Ildefonso2*
1Hospital Star Medica, Av. Virrey de Mendoza N° 2000 Col. Félix Ireta C.P. 58070, Morelia, Mich, Mexico.
2Neurology and Service. Hospital Central “Dr. Ignacio Morones Prieto”. Venustiano Carranza 2395, Zona Universitaria, 78290. San Luis Potosí, San Luis Potosí, México and Facultad de Medicina, Universidad Autónoma de San Luis Potosí. Venustiano Carranza 2405, Los Filtros, 78210. San Luis Potosí, San Luis Potosí, México.
3Neurology Service, General Hospital of Culiacan; Culiacán, Sinaloa, Mexico.
4Clínica Galeno, Cardiology Service, Morelia Michoacan, Mexico.
*Corresponding Author : Rodriguez L Ildefonso
Head, Neurology Service, Hospital Central “Dr. Ignacio Morones Prieto”. Venustiano Carranza 2395, Zona Universitaria, 78290. San Luis Potosí, San Luis Potosí, México.
Email: ildefonso.rodriguez@uaslp.mx.
Received : Sep 13, 2022
Accepted : Oct 12, 2022
Published : Oct 19, 2022
Archived : www.jcimcr.org
Copyright : © Ildefonso RL (2022).
Abstract
Primary cardiac tumours are rare; 75% of primaries are benign mesenchymal, mostly myxomas. Primary sarcomas are the second most frequent type. Only a few hundred primary cardiac sarcomas have been reported, most diagnosed by autopsy. Sarcomas of the intima are polypoid mesenchymal masses anchored to a vessel or the cardiac wall. To our knowledge, there is a unique report of primary cardiac Sarcoma complicated with cerebral infarction and cerebral metastatic disease. Metastases show a preference for lung, liver, and mediastinum, but the brain is usually a sanctuary. We describe a female in her forty’s with recurrent stroke associated with a cardiac sarcoma, also presenting brain metastases, who died a year after starting the problem by pulmonary thromboembolism.
Keywords: Cardiac tumour; Sarcoma; Stroke.
Citation: Marcela GV, Davalos RP, Jorge VC, Cázarez RAM, Ildefonso RL, et al. Recurrent stroke associated with brain metastasis due to a cardioembolism secondary to left atrial Sarcoma: Case presentation and review of the literature. J Clin Images Med Case Rep. 2022; 3(10): 2110.
Background
Primary tumours of the heart are rare. About 75% of primary cardiac tumours are benign mesenchymal tumours, most of which are myxomas. Although very rare, primary sarcomas of the heart are the second most common type of primary cardiac tumours [1]. Currently, only a few hundred primary cardiac sarcomas have been reported, most of which are based on autopsy series [2]. Intimal sarcomas are malignant mesenchymal tumours originating in the intima as polypoid masses anchored to a vessel or the cardiac wall. They have a thrombus-like appearance [3,4]. There is a wide variety of possible clinical presentations. They appear by four distinct mechanisms: obstruction of blood flow and interference with valvular function; local invasion leading to arrhythmias or pericardial effusion; embolic phenomena; or systemic symptoms. All mechanisms may overlap and present in different combinations, resulting in a variable clinical picture [5]. Given the fragility of the tumour, patients often experience systemic embolisms, which may be the initial form of presentation [6]. The site of metastases shows a preference for the lung, liver, and mediastinum, but the brain appears to be an uncommon site of metastases [7].
Clinical case
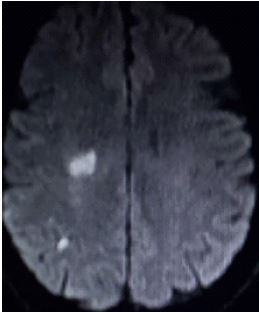
A woman in her 40s presented in ER in late May 2020 with sudden dizziness, followed by confusion and bradypsychia that resolved within minutes. However, it made left hemiparesis evident. She had a history of arterial hypertension (losartan 50 mg PO qDay). She denied tobacco, alcohol or illicit drug use and another relevant history. On examination, the heart was rhythmic and without murmurs. She had only mild left facial and body hemiparesis on neurological examination with brachial predominance, symmetrical muscle stretch reflexes ++, and bilateral plantar flexor response. There were no other significant data. A cranial MRI showed an acute infarct in the right middle cerebral artery territory, mainly in the right frontal operculum (Figure 1). Routine blood tests, including TSH, lipid profile and SARS-CoV2, were all normal.
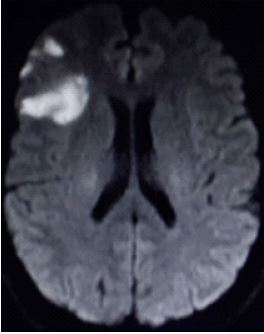
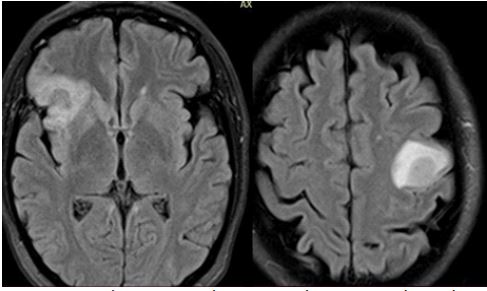
A 24-hour Holter and transthoracic echocardiogram were reported without significant alterations. CT angiography was also irrelevant. The immunological and prothrombotic laboratory profile was also negative. In the following month, he presented sudden dysarthria. A new MRI showed ischemic lesions in the right middle cerebral artery territory (Figure 2).
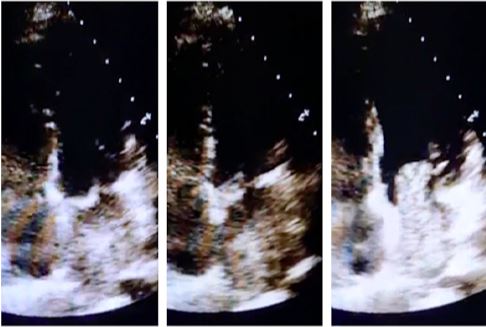
A new transthoracic echocardiogram showed a 9 x 2 cm mass originating in the atrial roof, causing severe mitral valve stenosis and moderate insufficiency (Figure 3).
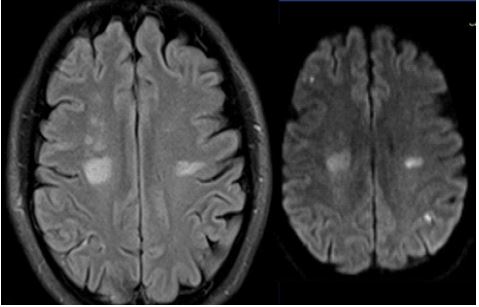
A new event was clinically present, and a new MRI showed infarct areas in the contralateral hemisphere (Figure 4).
The patient underwent surgery. Trans-operative findings of a tumour lesion in the left atrium invading the mitral valve and adjacent vessels and the histopathological diagnosis was a poorly differentiated intimal sarcoma was followed up by oncology. A whole-body 18F-FDG PET/CT scan was performed and was negative.
In late 2020, the patient presented for the third time with focal neurological symptoms, and a new cranial MRI showed an occupational process with perilesional oedema compatible with brain metastasis (Figure 5). Consequently, radiotherapy was started. Unfortunately, one year after starting the problem, the patient developed pulmonary thromboembolism and died.
Discussion
Virtually all types of sarcomas in the heart have been described [10]. They are sporadic tumours. Their incidence is 0.03%, although cardiac Sarcoma is the most frequent primary tumour in up to 30% of cases [11,12]. It can occur at any age; its maximum incidence is around 40 years, affecting men and women equally, and survival is only 24 months or less after complete resection [13,14].
Its clinical presentation is varied; it may begin with a sudden onset, with positional symptoms of chest discomfort, dyspnea, orthopnea, cough, or syncope. Poor heart valve function results in heart failure, arrhythmias or obstructive symptoms, depending on the chamber affected [15].
Sun YP et al. in 2017 described the first report of a primary Sarcoma complicated with cerebral infarction and brain metastases after initial cardiac mass resection surgery. These tumours can lead to brain metastases and cerebral vascular complications such as infarcts, haemorrhages, and intracranial aneurysms [16]. Patients often suffer systemic embolisms, and the brain is a frequently affected site.
Diagnosis is with noninvasive techniques, with echocardiography (transthoracic or transesophageal) beneficial for this purpose. Cardiac CT and MRI help predict the cardiac mass’s malignant nature, with features such as broad-based lesions. These lesions occupy the entire cardiac chamber, infiltrating the myocardium, pericardium or necrosis of adjacent structures and metastasis [17]. Transesophageal echocardiography is the first step in diagnosis because it is a reliable and inexpensive test showing the tumour’s size, location, and fixation. MRI, CT, and PET can show the different cardiac extents and metastases present in up to 80% of patients at the time of diagnosis. A definitive diagnosis requires histologic examination [18].
The diagnosis in this patient was challenging because the first echocardiogram was reported negative, and we considered subclinical atrial fibrillation. Two new trials support evidence that prolonged cardiac event monitoring increases the detection of subclinical Atrial Fibrillation (AF) in patients with a Transient Ischemic Attack (TIA) or acute ischemic stroke. In the PER DIEM trial of patients with cryptogenic stroke, new AF was observed in 15.3 % of patients in the insertable cardiac monitor group (placed for one year) compared with 4,7% in the external loop recorder group (worn for four weeks) [19]. The STROKE-AF trial of patients with large or small vessel stroke detected new AF in 12.1% of patients in the insertable cardiac monitor group compared with 1.8% in the usual care group of dedicated external cardiac monitoring [20]. Fortunately, a second transthoracic echocardiogram was performed after the second ischemic stroke, and we made the correct diagnosis.
This presentation is interesting because of the rarity of cardiac sarcomas and the clinical presentation of a rare recurrent infarct associated with metastases. To our knowledge, there is only another report in the literature like the one we present.
The outcomes of these patients are unfavourable, with poor short-term survival. Patients treated with surgery alone have a median survival of 3 months to 1 year. Postoperative radiotherapy is effective, but its value is limited by the sensitivity of the heart to radiation, resulting in cardiomyopathy and chronic pericarditis [21].
References
- Silverman NA. Primary cardiac tumour. Ann Surg. 1980; 191: 127–138.
- Zhang PJ, Brooks MD, Goldblum JR, Yoder B, Seethaka R, et al. the health primary cardiac sarcomas: A clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival. Hum Pathol. 2008; 39: 1385-1395.
- Van Diesel J, Sciot R, Delcroix M, et al. Single-center experience with intimal Sarcoma, an ultra-orphan, commonly fatal mesenchymal malignancy. Oncol Res Treat 2017; 40: 353–359.
- Hirsch K, Falkensammer J, Starkl T, Richter B, Beham A, et al. Intimal angiosarcoma of the carotid artery. Eur J Vasc Endovascular Surg. 2014; 47: 331.
- Pedro Enrique Jiménez Caballero. The Neurologist. 2008; 14: 2. Lippincott Williams & Wilkins.
- McManus Bruce, Lee Cheng Han. Chapter 69 primary. tumors of the heart. In: Libby Peter, Bon now Robert O, Mann Douglas L, et al. Eds. Braunwald’s Heart Disease. 8th ed. 2008-1815-1828
- D Pasalic, LT Hegerova, WI Gonsalves, et al. An insidious cardiac sarcoma presenting with progressive neurologic dysfunction, Rare Tumors. 2013; 5: e56.
- Berkhemer OA, Fransen PSS, Beumer D, et al. A randomised trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015; 372: 11-20.
- Kang DH, Hwang YH, Kim YS, et al. Direct thrombus retrieval using the reperfusion catheter of the penumbra system: Forced-suction thrombectomy in acute ischemic stroke: AJNR Am J Neuroradiol. 2010; 31: 283-287.
- Vander S. Unusual primary tumors of the heart. Semin Thorac Cardiovasc Surg. 2000; 12: 89-100.
- Burke A and Virmani R. Tumors of the heart and great vessels. In: Atlas of tumor pathology. 3rd series. Washington (DC): American Registry of Pathology. 1996; 1–98.
- Hoffmerier A, Deiters S, Schmidt C, et al. Radical resection of cardiac Sarcoma. Thorac Cardiovasc Surg 2004; 52: 77–81.
- Wu JC, Fishbein MC, Child JS. An unusual cause of stroke from a left atrial mass. J Am Soc Echocardiogr 2007; 20: 537.e1–e2.
- Jassal DS, Thakrar A, Neilan TG, et al. Cardioembolic stroke in patient with spindle cell sarcoma of the left atrium. J Am Soc Echocardiogr. 2007; 20: 438.e1–e4.
- Nihar Mehta, Ajit Desai, Bharat Shivadasani, Satyjeet Suryawanshi, AB Mehta, et al. Left A trial Spindle Cell Sarcoma- Case report. Indian Heart Journal. 2012; 64: 416-419.
- Sun YP, Wang X, Gao YS, Zhao S, Bai Y, et al. Primary cardiac sarcoma complicated with cerebral infarction and brain metastasis: A case report and literature review. Cancer Biomark. 2017; 21: 247-250.
- Hoffmann Udo, Globits Sebastian, Schima Wolfgang, et al. Usefulness of magnetic resonance imaging of cardiac and pericardiac masses. Am J Cardiol. 2003; 92: 890-895.
- Gupta A. Primary cardiac sarcomas. Expert Rev Cardiovasc Ther. 2008; 6: 1295-1297
- Brain H. Buck, MD, Michael D. Hill, Russel Quinn, et al. Effect of implantable vs Prolonged External Electrocardiographic Monitoring on Atrial Fibrillation Detection in Patients with Ischemic Stroke. The PER DIEM Randomized Clinical Trial. Jama. 2021; 325: 2160-2168.
- Richard A Bernstein, Hooman Kamel, Christopher B Granger, et al. Effect of Long-term Continuous Cardiac Monitoring vs Usual Care on Detection of Atrial Fibrillation in Patients With Stroke Attributed to Large- or Small-Vessel Disease. The Stroke-AF Randomized Clinical Trial. Jama. 2021; 325: 2169-2177.
- Reineke Moeri Schimmel, Elisabeth Pras, Ingrid Desar, Sijin Krol, Petra Braam. Primary Sarcoma of the heart: Case report and literature review. Journal of Cardiothoracic Surgery BMC. 2020.