
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Three cases of eruptive syringoma with dermoscopic features
Beixue Jiang1; Yangyang Jiang2; Xiaojing Guo2; Fang Yang1*
1Department of Dermatology, Shenzhen People’s Hospital (The Second Clinical Medical College, Jinan University; The First Affiliated Hospital, Southern University of Science and Technology), Shenzhen 518020, Guangdong, China.
2Department of Pathology, Shenzhen People’s Hospital (The Second Clinical Medical College, Jinan University; The First Affiliated Hospital, Southern University of Science and Technology), Shenzhen 518020, Guangdong, China.
*Corresponding Author : Fang Yang
Department of Dermatology, Shenzhen People’s Hospital (The Second Clinical Medical College, Jinan University; The First Affiliated Hospital, Southern University of Science and Technology), Shenzhen 518020, Guangdong, China.
Email: yangfang 3013@126.com
Received : Dec 15, 2020
Accepted : Oct 13, 2022
Published : Oct 20, 2022
Archived : www.jcimcr.org
Copyright : © Yang F (2022).
Abstract
Syringoma is a benign adnexal neoplasm originating from the intraepidermal eccrine duct. Eruptive Syringoma (ES) is a rare variant that is characterized by skin-colored to reddish-brown and shiny papules. Here we report three cases of ES, one of them initially misdiagnosed as Darier disease. Dermoscopy showed light brown pigment networks and dotted or linear vessels. All these cases were confirmed as ES by histopathological examination, highlighting the importance of histopathological and dermoscopic evaluation.
Keywords: Syringoma; Eruptive; Dermoscopy; Biopsy.
Citation: Jiang B, Jiang Y, Guo X, Yang F, et al. Three cases of eruptive syringoma with dermoscopic features. J Clin Images Med Case Rep. 2022; 3(10): 2112.
Introduction
Syringoma is a relatively common benign adnexal neoplasm originating from the ducts of eccrine sweat glands. Clinically, lesions appear as multiple, non-fusion, skin-colored small papules, and primarily affect the eyelids of women during adolescence or adulthood. ES is a rare variant of syringoma first described by Biesiadecki and Kaposi in 1887 [1]. It can be easily missed diagnosis or misdiagnosis clinically. We present here three rare cases of ES localized in multiple sites.
Case presentations
Case 1
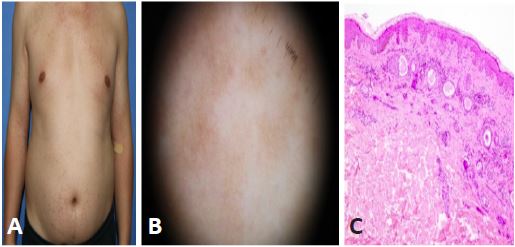
A 28-year-old man presented to our department with multiple asymptomatic papules on the trunk and upper limbs. He was diagnosed with Darier disease and treated with oral and topical tretinoin. However, the lesions were not subsided. Then the therapy was stopped because of elevated liver enzymes. No other members of the family had similar skin lesions. Physical examination revealed multiple, smooth, firm, non-fusion, reddish to dark red papules, 1 mm to 4 mm in diameter on the neck, chest, abdomen, and flexion of upper limbs (Figure 1a). Dermoscopy showed light brown pigment networks and a yellowish-white unstructured area surrounded by linear vessels on a pink background under polarized light (Figure 1b). Histopathological examination showed epithelial cords, ducts, and cystic structures within the superficial dermis. The ducts were lined by two rows of epithelial cells, characteristic of a tadpole-like pattern, and filled with eosinophilic amorphous substances (Figure 1c).
Case 2
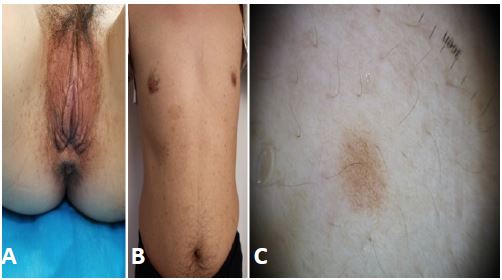
A 27-year-old woman with an 8 years history of asymptomatic papules located on her body. She denied any use of medications. Physical examination revealed multiple flesh-colored to reddish papules over the face, armpit, trunk, thigh, and vulva (Figure 2a). Histopathological examination showed the classical histopathological features of syringoma.
Case 3
An otherwise healthy 43-year-old man presented with brownish flat-topped papules on the chest and abdomen for 19 years (Figure 2b). The lesions remained stable with no progression. Dermoscopy showed a light brown pigment network and dotted and linear vessels on a pale yellow background (Figure 2c). Histopathological examination showed the classical histopathological features of syringoma.
The three cases’ clinical pictures and dermoscopic findings coupled with the histopathologic features were consistent with the lesions being ES. The patient of case 1 experienced recurrence after being treated with electrocautery. The lesions were constantly increasing in multiple sites including biopsy sites during the past year. The patient of case 2 exhibited lesions recurrence following CO2 laser and the lesions were increased in the past year. The patient of case 3 opted for no intervention after being informed the lesions were benign. The lesions remained stable during follow-up.
Discussion and conclusion
Syringoma was divided into four variants based on clinical features: localized, familial, a form associated with Down syndrome, and a generalized variant, including multiple and eruptive Syringomas (ES) [2]. The pathogenesis of ES remains unknown. Some scholars speculated that ES was thought to be under hormonal influence, and others thought that autoimmune status, immunosuppression (liver and kidney transplantation), drug hypersensitivity, trauma from waxing, radiation, picking, and heat stimuli [3,4]. The lesions are present symmetrically and characterized by skin-colored to reddish-brown shiny papules or flat-topped papules. However, few cases present pigmentation, erythema, Darier signs positive, or pseudokoebnerization [5]. They are typically located on the eyelids, neck, anterior chest, upper abdomen, upper extremities, axillae, and genitals, except on the palms, soles, or mucous membranes. Commonly manifested with asymptomatic or itching and gradually subsided in rare cases.
ES is easily misdiagnosis clinically and may be confused with Darier disease, Fox-Fordyce disease, lichen planus, mastocytosis, granuloma annulare, trichoepithelioma, or sarcoidosis. In addition, it is associated with systemic syndromes such as Nicolau–Balus syndrome (syringomas, milia, and atrophoderma vermiculata) and Down syndrome. Meanwhile, Marfan and Ehlers–Danlos syndromes need to be ruled out when lesions involve the eyelids [6]. In our patients, no associated systemic syndromes were found. The diagnosis of ES can be established on a clinical, dermoscopic, and histopathological basis. Notably, dermoscopy is a non-invasive examination and helps narrow the differential diagnosis. In our cases, patient 1 was misdiagnosed and treated for Darier disease initially. In most patients of ES, dermoscopy findings of reticular brown lines or fine pigment networks were described, which is consistent with our patients. Some cases reported that tiny whitish dots, multifocal hypopigmented areas, and glittering yellow-whitish round structures are considered the dermoscopic hallmarks of the vulvar variant [7-9]. Histopathological examination showed the presence of epithelial cords, ducts, and cystic structures within the superficial dermis. The ducts were lined by two rows of epithelial cells, with a characteristic comma-shaped/tadpole-like pattern, and filled with eosinophilic amorphous substances. In Darier disease, the dermoscopic evaluation showed comedo-like openings with a central polygonal yellowish/brownish structure, surrounded by a whitish halo on a pink background [10]. Histopathology findings showed acantholysis above the basal layer of the epidermis and dyskeratotic keratinocytes.
At present, there is no effective treatment for ES. The purpose of treatment is to improve the cosmetic appearance. It is mainly treated by local physical and chemical therapy, including surgical resection, cryosurgery, electro desiccation, CO2 laser, CO2 laser combined with trichloroacetic acid [5], argon laser, fractional photothermolysis, dermabrasion, and chemical peeling. However, due to this variation type always involving the deeper regions of the dermis, some treatments may cause pigmentation, scar formation, or recurrence, and the therapeutic effect is not ideal. Systematic therapy includes oral retinoic acid or tranilast [11]. Topical retinoic acid and atropine are also been reported. But the efficacy is still uncertain. It is noteworthy that our patient’s (case 1) lesions did not alleviate after oral and topical retinoic acid, and side effects occurred (increased liver enzyme levels). After receiving CO2 laser or electrocautery therapy (patient 1 and patient 2), there was recurrence of the lesions and no pigmentation and scar formation during follow-up. The disease was not self-limiting in our case series.
References
- Jacquet L, Darier J. Hidradénomes éruptifs, I.épithéliomes adenoids des glandes sudoripares ou adénomes sudoripares. Ann Dermatol Venereol. 1887; 8: 317-323.
- Williams K, Shinkai K. Evaluation and management of the patient with multiple syringomas: A systematic review of the literature. Journal of the American Academy of Dermatology. 2016; 74: 1234-1240.e1239.
- Huang A, Taylor G, Liebman TN. Generalized eruptive syringomas. Dermatology online journal. 2017; 23.
- Maeda T, Natsuga K, Nishie W, Yamashita K, Shimizu H, et al. Extensive Eruptive Syringoma After Liver Transplantation. Acta dermato-venereologica. 2018; 98: 119-120.
- Samia AM, Donthi D, Nenow J, Malik P, Prenshaw K, et al. A Case Study and Review of Literature of Eruptive Syringoma in a Six-Year-Old. Cureus. 2021; 13: e14634.
- Soler-Carrillo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. Journal of the European Academy of Dermatology and Venereology: JEADV. 2001; 15: 242-246.
- Aleissa M, Aljarbou O, AlJasser MI. Dermoscopy of Eruptive Syringoma. Skin appendage disorders. 2021; 7: 401-403.
- Botsali A, Caliskan E, Coskun A, Tunca M. Eruptive Syringoma: Two Cases with Dermoscopic Features. Skin appendage disorders. 2020; 6: 319-322.
- Dutra Rezende H, Madia ACT, Elias BM, Peraro TF, Mattos Dinato SL, et al. Comment on: Eruptive Syringoma - Two Cases with Dermoscopic Features. Skin appendage disorders. 2022; 8: 81-82.
- Silva Hirschberg C, Cabrera R, Rollán MP, Castro A, et al. Darier disease: The use of dermoscopy in monitoring acitretin treatment. Anais brasileiros de dermatologia. 2022.
- Horie K, Shinkuma S, Fujita Y, Ujiie H, Aoyagi S, et al. Efficacy of N-(3,4-dimethoxycinnamoyl)-anthranilic acid (tranilast) against eruptive syringoma: Report of two cases and review of published work. The Journal of dermatology. 2012; 39: 1044-1046.