
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Benign fibroepithelial polyp of ureter masquerading as upper
tract urothelial carcinoma: A management conundrum
Anshuman Singh; Arun Chawla*; Anupam Choudhary; Bommireddy V Reddy
Department of Urology and Renal Transplant, Kasturba Medical College, Manipal, India.
*Corresponding Author : Arun Chawla
Professor & Head, Department of Urology and Renal Transplant, Kasturba Medical College, Manipal, India.
Email: arun.chawla@manipal.edu
Received : Sep 15, 2022
Accepted : Oct 13, 2022
Published : Oct 20, 2022
Archived : www.jcimcr.org
Copyright : © Chawla A (2022).
Abstract
Upper tract Urothelial Cell Carcinomas (UTUCs) account for only 5–7% of urothelial carcinomas. Of these only 25% are located in the ureter. The imaging characteristics of these tumors can mimic certain benign entities like fibroepithelial polyps. The gold standard treatment for invasive upper tract urothelial carcinomas, regardless of the tumor’s location in the UUT, is Radical Nephroureterectomy (RNU) with excision of a bladder cuff. We describe the case of a patient with postoperatively detected benign fibroepithelial polyp who presented with symptoms and findings mimicking features of an UTUC. In cases where the preoperative diagnosis is in doubt, which can be the case with ureteric fibroepithelial polyps, surgical treatment should be to attempt complete excision of the tumor with renal preservation to prevent unnecessary nephrectomy.
Citation: Singh A, Chawla A, Choudhary A, Reddy BV, et al. Benign fibroepithelial polyp of ureter masquerading as upper tract urothelial carcinoma: A management conundrum. J Clin Images Med Case Rep. 2022; 3(10): 2113.
Introduction
The upper urinary tract Urothelial Cell Carcinomas (UTUCs) account for only 5–7% of urothelial carcinomas. Of these only 25% are located in the ureter. In western countries, the incidence is 1-2 cases per 100,000 per year [1]. Typical symptoms are gross haematuria (80%) and flank pain (30%) and often caused by clots passing down the ureter. Males are affected three times as common as women. The incidence increases with age and smoking confers a two fold risk [1]. Diagnosis is usually made combining with urine cytology, Intravenous Urography (IVU), or multidetector computed tomographic urography. Ultrasound is excellent for detecting renal parenchymal tumours, but not tumours of the renal pelvis or ureter. Further investigations are selective ureteric urine cytology, retrograde pyeloureterography, or flexible uretero-renoscopy [1]. The gold standard treatment for invasive upper tract urothelial carcinomas, regardless of the location of the tumour in the UUT, is Radical Nephroureterectomy (RNU) with excision of a bladder cuff. We describe the case of a patient with postoperatively detected benign fibroepithelial polyp who presented with symptoms and findings mimicking features of an UTUC.
Case scenario
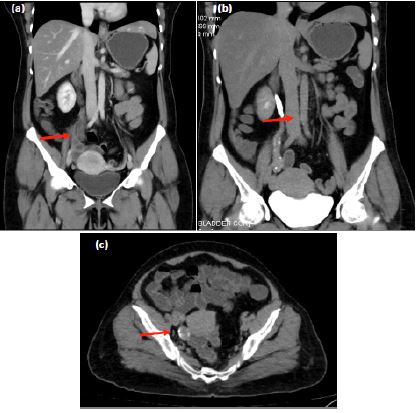
A 46 year old diabetic female presented to our hospital with recurrent right loin pain for the past six months. The pain was not associated with any other symptoms. There was no history of visible haematuria, lower urinary tract symptoms or constitutional symptoms. Other personal and family history was normal. Urine analysis was suggestive of microscopic hematuria and pyuria. She was evaluated with ultrasonography of abdomen which detected right side hydroureteronephrosis with normal renal parenchyma. Urinary bladder was normal sonologically with no tumor. Contrast enhanced CT scan of abdomen was done along with CT urogram which showed dilated ureter with irregular soft tissue density filling defect showing heterogenous contrast enhancement extending from L1 vertebrae till vesicoureteral junction and causing retrograde minimal hydroureteronephrosis. Right side RGP was done subsequently which revealed irregular filling defects in the ureter extending from L2 vertebral level till vesicoureteral junction. Right ureteroscopy was suggestive of irregular polypoidal lesion causing near complete obliteration of ureteral lumen at mid-distal ureteric level. Ureteroscope could not be negotiated beyond the mid ureter. Urine cytological examination was negative for malignant cells.
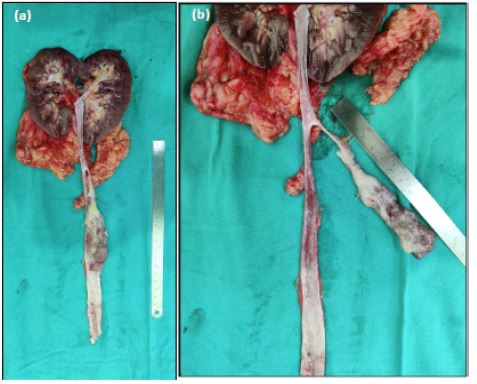
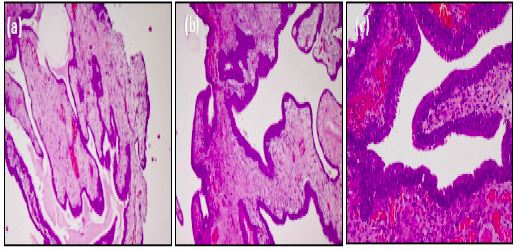
The differential diagnosis included urothelial carcinoma of the ureter, benign neoplastic lesion of the ureter and any chronic inflammatory pathology of the ureter. However, keeping in mind the heterogenously enhancing nature of the lesion causing near complete obliteration of the ureteric lumen with microscopic haematuria the provisional diagnosis was kept as malignant and the patient was taken up for right nephroureterectomy. Postoperatively excised specimen was suggestive of solitary pedunculated polyp arising from proximal ureter with rest of the ureteric mucosa normal on gross examination. Histopathology was suggestive of fibroepithelial polyp of the ureter with no evidence of any malignant focus.
Discussion
A Ureteric Fibroepithelial Polyp (UFP) is a rare cause of haematuria and hydronephrosis. The prevalence of ureteric fibroepithelial polyp is rare with only 200 cases documented in the literature. In recent years, most cases are reported in Asian chilchildren, but older reviews show that it can occur in every age [2,3] as was noted in our case. With non-specific imaging findings it is difficult to differentiate it from Upper Tract Urothelial Carcinomas (UTUC), which are usually treated by radical nephroureterectomy. Preoperative differentiation between UTUCs and ureteric fibroepithelial polyp cannot be made with imaging tests only. Urine cytology and endoscopic biopsy alone might be insufficient to confirm the diagnosis as shown in our case report because of high false negative rates observed with these investigations in cases of later confirmed malignancy [11].
UFP can occur in any age, but commonly present in the third to fourth decades. Males are 1.5 times more affected than females. Most UFP occur in the left ureter with a predilection for the proximal segment. Mean fibroepithelial polyp diameter is reported with less than 5 cm; however, larger polyps that even can protrude into the bladder have been reported [7,8]. Ureteral polyps usually appear as solitary tumours; however, rare cases of multiple and bilateral appearance have also been reported [2].
Most common symptoms of patients with UFP are visible haematuria and intermittent right pelvic pain. Some cases are presented with hydronephrosis. IVU or retrograde pyelography typically demonstrates a tubular filling defect. This finding combined with negative cytology and biopsy would raise the suspicion for UFP. There are no evidence based guidelines for the treatment of a UFP, however, priority should be given to complete excision of the tumour with renal preservation so as to cause minimal risk of subsequent morbidity of a nephrectomy.
Histologically, these polyps are composed of stroma derived from the mesoderm and covered by a layer of normal transitional epithelial cells [4]. Most UFP are long pedunculated projections with a smooth surface arising from a small and narrow base. These polyps are thought to be either congenital slow growing lesions or lesions that develop as a result of chronic urothelial irritants, such as infection, inflammation, or obstruction. Other benign lesions of the upper urinary tract that may be included in the differential diagnosis of filling defects in ureter on contrast based imaging modalities include endometriomas, fibromas, leiomyomas, granulomas, neurofibromas, haemangiomas, and lymphangiomas [5,6].
Despite no preoperative evidence of malignancy, many case reports of UFP include management by open or laparoscopic surgery. Recent publications refer to endoscopic, percutaneous or ureteroscopic excisions or laser ablation of the polyp [2,9]. Endoscopic treatment is associated with minimal operative morbidity to the patient but like in our case, endoscopic access to evaluate the entire extent of the polyp can be limited and is not always possible. The polyp can constrict the ureter so that it is impossible to pass or access the base of the polyp. View also can be limited by little working space or bloody urine, so that open or laparoscopic approach with segmental resection of the ureter becomes necessary [2]. In many cases preoperative diagnosis is also uncertain and there remains a risk and suspicion for undertreating an undiagnosed focus of urothelial carcinoma when the imaging characteristics are non-specific. Williams et al [10] reported that 49% of their cohort underwent nephroureterectomy, while the remainder underwent open surgical exploration with local excision. Debruyne et al. in their series of 108 patients reported that 37% of the patients underwent nephroureterectomies because of an uncertain preoperative diagnosis [12]. With technological advances, the mainstay of evaluation of suspicious ureteral lesions has become diagnostic ureteroscopy and biopsy. Ureteroscopic assessment has advantage possibility of endoscopic resection or ablation of the polyp. However in case of diagnostic dilemma preoperatively, many patients require nephroureterectomy due to suspicion of urothelial malignancy and the histological diagnosis of UFP is made postoperatively, as in our case.
Conclusion
A fibroepithelial polyp of the ureter is a rare benign tumour mimicking typical findings of UTUC. It has to be included in the differential diagnosis of UTUC, especially when urine cytology and biopsy are negative. In this condition of diagnostic uncertainty priority should be given for excision of tumour with renal preservation or intraoperative confirmation of any focus of malignancy before proceeding for radical nephroureterctomy.
References
- M Roupreˆt, R Zigeuner, J Palou, et al. Guidelines on Upper Urinary Tract Urothelial Cell Carcinomas, European Association of Urology Guidelines, 2011.
- MA Childs, EC Umbreit, AE Krambeck, TJ Sebo, DE Patterson, MT Gettman, et al. Fibroepithelial polyps of the ureter: A single-institutional experience, Journal of Endourology. 2009; 23: 1415–1419.
- Y Sun, C Xu, X Wen, et al. Is endoscopic management suitable for long ureteral fibroepithelial polyps? Journal of Endourology. 2008; 22: 1459–1462.
- TR Williams, BJ Wagner, WR Corse, JC Vestevich, et al. Fibroepithelial polyps of the urinary tract, Abdominal Imag- ing. 2002; 27: 217–221.
- JS Lam, JB Bingham, M Gupta. Endoscopic treatment of fibroepithelial polyps of the renal pelvis and ureter, Urology. 2003; 62: 810–813.
- HJ Kiel, T Ullrich, W Roessler, WF Wieland, R Knuechel-Clarke. Benign ureteral tumors. Four case reports and a review of the literature. Urologia Internationalis. 1999; 63: 201–205.
- K Kijvikai, LJ Maynes, SD Herrell. Laparoscopic management of large ureteral fibroepithelial polyp, Urology. 2007; 70: 373.e4–373.e7.
- A Coloma del Peso, G Bocardo Fajardo, F Teba del Pino, et al. Endoscopic treatment of a giant fibroepithelial polyp of the ureter. Archivos Espanoles de Urologia. 2010; 63: 305– 308.
- D Baltogiannis, A Kafetzoulis, D Giannakis, M Saito, I Miya-gawa, N Sofikitis, et al. Fibroepithelial polyp of distal ureter with periodic prolapse into bladder, Urologia Internationalis. 2008; 80: 338–340.
- Williams PR, Feggetter J, Miller RA, Wickham JE. The di- agnosis and management of benign fibrous ureteric polyps. Br J Urol. 1980; 52: 253–256.
- Zhao Y, Deng FM, Melamed J, Huang WC, Huang H, Ren Q, et al. Diagnostic role of urine cytology and ureteroscopic biopsies in detection of high grade upper tract urothelial carcinoma. Am J Clin Exp Urol. 2021; 9: 221- 228.
- Debruyne FM, Moonen WA, Daenekindt AA, Delaere KP. Fibroepithelial polyp of ureter. Urology. 1980; 16: 355– 359.