
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Two cases of intracranial infection after percutaneous
microballoon compression of trigeminal neuralgia
Zhong Yu-Long1†; Zhu Chun-Ran2†; Xu Wu1; Wang Jing1; Jiang Cheng-Rong1; Hu Jing-Wen2; Liang Wei-Bang1*
1Department of Neurosurgery, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing 210008 Jiangsu, China.
2Department of Neurosurgery, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing 210028, Jiangsu Province, China.
†Equal Contributors.
*Corresponding Author : Liang Wei-Bang
Department of Neurosurgery, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing 210008 Jiangsu, China.
Email: 13901597020@163.com
Received : Sep 15, 2022
Accepted : Oct 14, 2022
Published : Oct 21, 2022
Archived : www.jcimcr.org
Copyright : © Wei-Bang L (2022).
Abstract
Introduction: Trigeminal neuralgia is a common cranial nerve disease. Percutaneous Microballoon Compression (PBC) has a definite therapeutic effect, and postoperative intracranial infection is rarely reported.
Case presentation: Case presentation: A total of 1051 patients with trigeminal neuralgia conducted PBC surgery in our hospital from October 2014 to December 2021, and 2 cases reported intracranial infection, which were cured and discharged after active and effective treatment. Combined with the experience of our center, we analyze the risk factors and management strategies for postoperative infection of trigeminal neuralgia PBC in order to provide a reference for the diagnosis and treatment of this disease for neurosurgeons.
Conclusion: The results showed that the patients with trigeminal neuralgia undergoing PBC surgery were mainly elderly, with masticatory difficulty due to pain accompanied by malnutrition, fear of facial cleaning because of pain which leads to oil accumulation, and even the possibility of infection in the skin and soft tissue space of the head and neck regions. Therefore, PBC puncture may lead to intracranial infection. The key to avoiding this is prevention, timely cerebrospinal fluid drainage and antibiotic treatment after infection are the keys to a good prognosis.
Keywords: Trigeminal neuralgia; Percutaneous microballoon compression; Intracranial infection.
Citation: Yu-Long Z, Chun-Ran Z, Wu X, Jing W, Wei-Bang L, et al. Two cases of intracranial infection after percutaneous microballoon compression of trigeminal neuralgia. J Clin Images Med Case Rep. 2022; 3(10): 2114.
Introduction
Trigeminal neuralgia is characterized by sharp and intense pain coming from the trigeminal nerve and is often described as burning, lancinating, and electric shock-like [1,2]. Compared with the classical surgical option of Microvascular Decompression (MVD), Percutaneous Balloon Compression (PBC) is a technically simple and minimally invasive surgery for treating TN with lower risks and shorter training duration, and is therefore widely adopted in all level hospitals [3,4]. Mean while, PBC postoperative intracranial infections are rarely reported. In this study, we offer the clinical data of two cases of PBC postoperative intracranial infection reported at the Department of Neurosurgery at Drum Tower Hospital Clinical College of Nanjing Medical University. Case characteristics and treatment process were retrospectively analyzed.
Cases presentations
Case 1
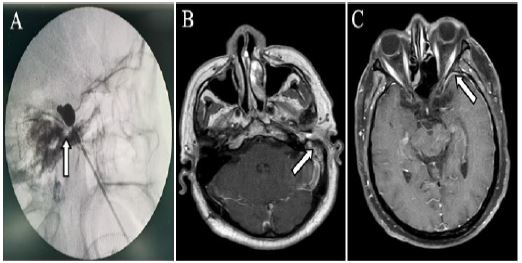
Female, a 64-year-old farmer. She developed a paroxysmal electric shock-like pain on the left face nine years ago and the symptoms worsened for a month. Past medical history revealed she had meningitis 49 years ago and was experiencing hearing loss in the left ear for the past half-year. Otherwise, her physical examinations were negative. A preoperative examination was conducted to prevent secondary lesions. The patient was diagnosed with 1. Left trigeminal neuralgia (the second and third branches). 2. Meningitis (infection history). 3. Left ear hearing loss. PBC surgery treatment was performed under general anesthesia, eliminating any surgical contraindications Microballoon shape under CT scan during the operation is shown in (Figure 1A). After the surgery, the patient experienced complete pain relief and mild facial numbness in the left face. On the second postoperative day, she did not experience discomfort and was discharged. The same night she was admitted to our emergency department due to high fever, with body temperature peaking at 41oC, increased respiratory and heart rate, and a loss of consciousness. Findings included: T39.6oC; R27BPM; P114 BPM; BP 132/96 mmHg; round pupils, equally sized at 2 mm; visual acuity; and neck stiffness. A routine blood test showed a leukocyte count of 13.6 x 109 /L; neutrophil percentage of 87.3%; and lymphocyte percentage of 7.8%. Routine lumbar puncture revealed that CSF was light yellow and slightly turbid; RBC count 0/L; leukocytecount4228 x 106 /L; neutrophil percentage 83.4%; and lymphocyte percentage 16.6%. CSF protein characterization: positive +; quantization: 3408.7 mg/L; glucose 1.39 mmol/L; Cl 120.8 mmol/L; and plasma procalcitonin 4.07 ng/ml. CSF culture: negative. Contrast-enhanced axial MRI revealed left ear otitis media (1B) while the enhancement in the left temporal region showed pachymeningeal thickening (1C). Anti-infective therapy of vancomycin-meropenem was given, and continuous lumbar drainage was conducted. The patient presented extensive her pes labialis on the third postoperative day. Antiviral ointment was applied to the area of infection, and anti-infective therapy was performed. Two days later, her body temperaturere turned to normal, and her consciousness fully recovered. Findings of a blood test after one week of continuous lumbar drainage and anti-infective therapy included: leukocytecount 8.6 x 109 /L; neutrophil percentage 81.4%; and lymphocyte percentage 13.4%. Routine lumbar puncture revealed that CSF was clear and colourless; RBC count 2000 x 106 /L; leukocyte count 35 x 106 /L; neutrophil percentage 19.5%; and lymphocyte percentage 80.5%. CSF protein characterization: negative; quantization: 1044.4 mg/L; glucose 2.13 mmol/L; Cl 122.7 mmol/L. CSF culture was negative. CSF indices, body temperature and blood indices remained normal for a day since lumbar drainage was removed. Her general condition improved rapidly, herpes labialis subsided, and she was discharged. She remains a symptomatic to this day.
Case 2
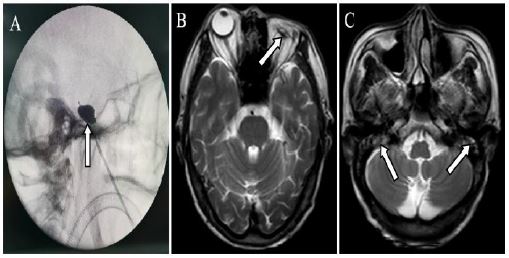
Male, a 79-year-old farmer. He experienced a paroxysmal electric shock-like pain on the left face for ten years and was hospitalized after the symptoms worsened for three months. His medical history is significant for a bilateral suppurative otitis media that led to bilateral hearing loss eight years ago and a purulent infection in the left eye that led to ophthalmectomy of the left eye three years ago. Otherwise, his physical examinations were negative. The patient was diagnosed with 1. Left trigeminal neuralgia (the first and second branches), 2. Absence of left eyeball (surgically removed), 3. Bilateral suppurative otitismedia (bilateral hearing loss). A preoperative examination was conducted to prevent secondary lesions. PBC surgery treatment was performed under general anesthesia, eliminating any surgical contraindications. Micro balloon shape under CT scan during the operation is shown in (Figure 2A). After the surgery, the patient experienced complete pain relief and mild facial numbness in the left face. At noon of the second postoperative day, the patient presented with high fever, with body temperature peaking at 39.8oC, a feeling of anxiety, and an increase in respiratory rate and heart rate. Findings included: mental prostration; disturbance of consciousness; T 38.7oC; R25 BPM; P105 BPM; BP 123/87 mmHg; left eyeball absent; right pupil 1.5 mm, round; visual acuity; and neck stiffness. A routine blood test revealed a leukocyte count of 7.1 x 109 /L; neutrophil percentage of 92%; and lymphocyte percentage of 6.1%. Routine lumbar puncture findings included CSF light yellow and slightly turbid; RBC count 0/L; leukocyte count 14816 x 106 /L; neutrophil percentage 90.9%; and lymphocyte percentage 9.1%. CSF protein characterization: positive+; quantization: 7551.2 mg/L; glucose 0.31 mmol/L; and Cl 117.4 mmol/L. CSF culture: negative. Head MRI showed ophthalmectomy of the left eye (2B) and bilateral suppurative otitis media (2A). Anti-infective therapy of vancomycin-meropenem was given. Due to bilateral hearing loss and anxiety of the patient, cooperation in lumbar cistern drainage was poor so that intermittent lumbar drainage was performed instead. On the third postoperative day, the patient presented extensive herpes labialis. Antiviral ointment was applied to the area of infection. The patient’s body temperature returned to normal after being given three days of anti-infective therapy, and his consciousness fully recovered. A routine blood test revealed a leukocyte count of 5.3 x 109 /L; neutrophil percentage of 87.4%; lymphocyte percentage of 6.5%. Routine lumbar puncture findings included CSF slightly yellow and turbid; RBCcount0/L; leukocyte count 2965 x 106 /L; neutrophil percentage 76.6%; lymphocyte percentage 23.4%. CSF protein characterization: positive; quantization: 3430 mg/L; glucose 1.6 mmol/L; Cl 126.3 mmol/L. CSF culture was negative. After a week of anti-infective therapy, the patient’s body temperature returned to normal, and his consciousness and mental state improved markedly. A second lumbar puncture was not performed as our patient refused. CSF indices, blood indices remained normal, herpes labialis subsided, and his general condition improved rapidly. Since discharged, he remained asymptotic without recurrence of pain or hyperthermia.
Discussion
Trigeminal neuralgia occurs mainly in middle-aged to older adults, presented as paroxysmal, severe, burning, lancinating, or electric shock-like pain in the distribution of trigeminal nerve. Various surgical treatment modalities are possible, among which MVD is the most classical approach and can effectively stop the pain while maintaining good facial sensory [5,6]. On the other hand, PBC acts as an ideal option for older and debilitated patients who fear intracranial operations, for the ones who present short trigeminal neuralgia, and for those who are refractory to previous MVD intracranial operation [7,8]. In the PBC technique, an inflated balloon was introduced to compress neuron bodies in the semilunar node of the trigeminal nerve, leading to ischemia followed by injury of the large myelinated fibers, achieving pain relief at the sacrifice of facial sensitivity. As a result, PBC patients are prone to postoperative facial sensory blunting. Compared to MVD, PBC possesses the merits of being minimally invasive, technically simple, quick in recovery, and low in risks. Therefore, it is widely accepted by patients and is implemented in hospitals of all levels.
PBC presents lower risks than MVD in the way that rare cases of intracranial infection have been reported. Since PBC was first carried out in our department in 2016, intracranial infection has been reported in 2 out of 1051 cases of TN treatment at an occurrence rate of 0.19%. Reviewing the clinical data of these two cases, balloon catheters were successfully introduced into the Meckel’s cave by a C-arm, the operation durations were controlled within 20 minutes, and the needle did not penetrate through to the oral cavity. Possible infection triggers are concluded as follows: 1) Patients of TN are reluctant to food intake by mastication due to long-term suffering from facial pain. This leads to malnutrition, debilitation, anemia and decreased immunity, which were observed in the above two patients. 2) Patients of TN are reluctant to touch their faces, leading to inadequate facial cleansing, which can give rise to sebum build up or even scabies and carbuncles which are difficult to remove with standard disinfectants. 3) Both these patients had a history of percutaneous infection. Case 1 patient suffered from meningitis and an ipsilateral otitis media, while case 2 patients suffered from suppurative otitis media and purulent eye infection. We there by infer that the primary focus of infection is present in the soft tissue space of the patients’ head and neck, which, if located in the penetrating route, can lead to intracranial infections. 4) Three days after the operation, both patients presented extensive herpes labialis whose distribution and severity were more significant than average. Trigeminal nerves are reported to host the herpes virus, whose activation can be triggered by operation, and the symptoms get more severe with decreased immunity [9,10]. According to our evaluation of 1051TN cases, the four factors above are all risk factors for postoperative intracranial infection, while the two patients described above presented all of them.
Patients who suffer from PB intracranial infections present hyperthermia quickly within 24 postoperative, with body temperature rising to 39 degrees or higher, followed by loss of consciousness and neck stiffness. Blood test, lumbar puncture test and CSF culture should be performed to identify the cause. Targeted treatments including continuous lumbar drainage, regular antibiotic therapy and nutrition support should be conducted. If treated properly, one should observe significant recovery within three days. The patient is ready for a discharge if no abnormalities are observed three days after the end of antibiotic therapy. The above two patients were both discharged upon proper treatment followed by recovery and have remained asymptotic.
The findings revealed some preventions for PBC postoperative intracranial infection. We recommend providing enteral nutrition support before the operation to improve the physical condition of a patient who has been experiencing difficulties in food intake and is under malnutrition. If the patient is featured by facial scabies and carbuncles, MRI results should be evaluated to determine the presence of soft tissue infections in the head and neck region. Medical history should be carefully reviewed, and if there is a previous head and neck infection, prophylactic antibiotics should be given for three days before and after the surgery. We propose using Chlorhexidine alcohol to clean up any facial sebum build up during anesthesia. The corner of the mouth on the same side of penetration should be sealed with medical film to avoid contamination of the wound by oral secretion. Bed making should be carried out under hygiene standards before surgery commencement. Keeping the patient’s head straight during a surgical operation facilitates quick and accurate positioning of the foramen ovale and can prevent penetration of the oral cavity. Avoiding unnecessary movements to complete the operation efficiently also reduces the risks of infections. If herpes labialis appears, antiviral ointment should be applied to the affected area. The patient’s condition typically improves remarkably in a week with improved nutrition and immunity.
Conclusion
In conclusion, trigeminal neuralgia patients are featured by individuals, and PBC surgery patients are dominated by the elderly. Common causes of intracranial infections during PBC surgery include malnutrition which is triggered by reluctance to mastication and the build up of sebum which is accompanied by the risks of soft tissue infections in the head and neck region due to inadequate facial cleansing. Appropriate preventative methods and postoperative disinfection can help to achieve good prognoses.
Declarations
Authors’ contributions: ZHONG Yu-long and ZHU Chun-ran contributed equally to the design and drafting of the manu script; WANG Jing, JIANG Cheng-rong and HUJing-wen were involved in the literature review; ZHONG Yu-long and XU Wu composed and amended the manuscript; LIANG Wei-bang monitored the quality this work. He also supervised and reviewed the manuscript.
References
- Xu R, Xie ME, Jackson CM. Trigeminal Neuralgia: Current Approaches and Emerging Interventions [J]. J Pain Res. 2021; 14: 3437-3463.
- Sterman-Neto H, Fukuda CY, Duarte KP, et al. Balloon compression vs radio frequency for primary trigeminal neuralgia: A randomized, controlled trial. Pain. 2021; 162: 919-929.
- Li MW, Jiang XF, Niu CS. Efficacy of and risk factors for percutaneous balloon compression for trigeminal neuralgia in elderly patients[J]. Br J Neurosurg. 2021; 35: 280-284.
- Chaves JPG, DE Oliveira TVHF, Francisco AN, et al. Trigeminal neuralgia recurrence: A comparison of microvascular decompression and percutaneous balloon compression: a fiveyears follow-up study [J]. Arq Neuropsiquiatr. 2021; 79: 51-55.
- Reddy VK, Parker SL, Patrawala SA, et al. Microvascular decompression for classic trigeminal neuralgia: determination of minimum clinically important difference in pain improvement for patient reported outcomes. Neurosurgery. 2013; 72: 749-754.
- Di Carlo DT, Benedetto N, Marani W, et al. Microvascular decompression for trigeminalneuralgia due to vertebrobasilar artery compression: A systematic review and meta-analysis. Neurosurg Rev. 2022; 45: 285-294.
- Ni H, Wang Y, Chen X, et al. Outcomes of Treatment for Elderly Patients with Trigeminal Neuralgia: Percutaneous Balloon Compression Versus Microvascular Decompression [J]. J Craniofac Surg. 2020; 31: e685-e688.
- Wu J, Xiao Y, Chen B, et al. Efficacy and safety of microvascular decompression versus percutaneous balloon compression in the treatment of trigeminal neuralgia: A systematic review and meta-analysis. Ann Palliat Med. 2022; 11: 1391-1400.
- Texakalidis P, Xenos D, Tora MS, et al. Comparative safety and efficacy of percutaneous approaches for the treatment of trigeminal neuralgia: A systematic review and meta-analysis. Clin Neurol Neurosurg. 2019; 182: 112-122.
- Wan C, Dong DS, Song T. High-Voltage, Long-Duration Pulsed Radiofrequency on Gasserian Ganglion Improves Acute/Subacute Zoster-Related Trigeminal Neuralgia: A Randomized, Double-Blinded, Controlled Trial. Pain Physician. 2019; 22: 361-368.