
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Cutaneous plasmacytosis in a 30-year-old
woman post COVID-19 vaccine
Shuangfei Liu1,2; Yuqi Tang1,2; Junchi Tang1,2; Yingying Luo2,3; Biying Qiu2,3; Bin Yang1,2,3*
1Guangdong College of Clinical Dermatology, Anhui Medical University, Guangzhou, China.
2Guangdong Provincial Dermatology Hospital, Guangzhou, China.
3Dermatology Hospital, Southern Medical University, Guangzhou, China.
*Corresponding Author : Bin Yang, MD, PhD
Guangdong College of Clinical Dermatology, Anhui Medical University, Guangzhou, China.
Tel: +8613922207231, Fax: +8613922207231;
Email: yangbin1@smu.edu.cn
Received : Sep 13, 2022
Accepted : Oct 14, 2022
Published : Oct 21, 2022
Archived : www.jcimcr.org
Copyright : © Yang B (2022).
Abstract
With the continuous spread of COVID-19 pandemic and no effective drugs for its treatment, getting vaccinated is the only effective method to defend against the COVID-19. However, few adverse events related to the vaccination of COVID-19 vaccine have been reported. Here, we report a case of cutaneous plasmacytosis after COVID-19 vaccination.
Keywords: Cutaneous plasmacytosis; Covid-19; Vaccination; Adverse event.
Citation: Liu S, Tang Y, Tang J, Lup Y, Yang B, et al. Cutaneous plasmacytosisina 30-year-old woman post COVID-19 vaccine. J Clin Images Med Case Rep. 2022; 3(10): 2115.
Introduction
Cutaneous plasmacytosis, a rare skin disorder which is originally reported in the Japanese population, is categorized as a subtype of skin lesions of IgG4-related disease [1,2]. The skin lesion mainly appeared on the trunk, with its clinical manifestation including multiple red-brown plaques and flat tumors. Biopsy shows there is lymphocytic infiltration around dermal vessels, mainly infiltrated with normal plasma cells, while the epidermis is not involved [3]. With the outbreak of the COVID-19 pandemic, the application of COVID-19 vaccine is becoming more and more widespread. Sinopharm BBIBP‐CorV and WIBP‐CorV are inactivated vaccine which is based on attenuated SARS‐CoV‐2 virus. Previous studies have corroborated the efficacy and safety of these two vaccines. The adverse reactions are mainly injection pain, fever, and fatigue [4,5]. In this article, we report a case of cutaneous plasmacytosis after COVID-19 vaccination.
Report of a case
A 30-year-old Chinese woman presented with a 1 year history of multiple brown-reddish plaques on her forehead and face. A dark-red plaque on her left forehead had first been noticed after receiving the first shot of COVID-19 vaccine (Sinopharm WIBP‐ CorV) about 1 year ago. After February 2021, skin eruptions had been started to spread slowly to the face after being vaccinated with the second shot of COVID-19 vaccine (Sinopharm BBIBP-CorV). 8 months later, after getting the third shot of COVID-19 vaccine (Sinopharm BBIBP-CorV), the skin eruptions began to spread quickly across her fac (Figure 1). The patient had no personal or family history of autoimmune disease. Physical examination showed round reddish macules and plaques on the face and firm and slightly atrophic skin in the center of the skin lesions on palpation. As for laboratory test results, complete blood count, serum total protein, and erythrocyte sedimentation rate were within normal limits. Immunologic study results revealed normal for anticardiolipin antibody, complement C3 and complement C4, while weakly positive for the anticentro mere antibody. Serum levels of immunoglobulin were elevated at 92.42 mg/dL (reference range, 3.92-86.40 mg/dL) for IgG4. Serum protein electrophoresis showed a decreased level of albuminbutan elevated level of gamma globulin. Additionally, the serologic test results for syphilis, and HIV were negative while Hepatitis B was positive. Biopsy from the left facial specimen presented with perivascular infiltrates of non-atypical plasma cells in the dermis, while the epidermis was not involved (Figure 2A and B). The results of immunohistology revealed plasma cells were positive for CD138 (Figure 2C). Based on the findings above, a diagnosis of cutaneous plasmacytosis was rendered. The treatment of this patient mainly consists of systemic corticosteroid therapy and topical application of tacrolimus, but the effectiveness is limited. After the application of 532 nm laser treatment, the patient’s condition had significantly improved, and the color of facial plaque had subsided.
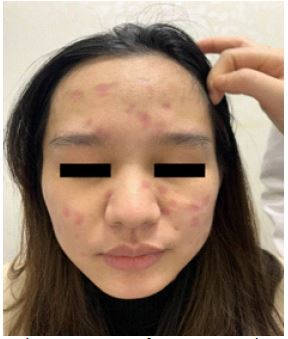
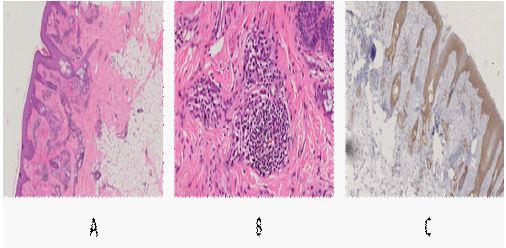
Figure 2A: Perivascular infiltrates of plasma cells inthe dermis and without epidermis involvement(hematoxylin-eosin, original magnification ×200).
Figure 2B: No atypical plasmacells were found(hematoxylin-eosin, original magnification ×400).
Figure 2C: The plasma cells were positive for CD138 (immunohistology, original magnification ×400).
Discussion
To date, this is the first case of an individual, without any other causes and related diseases, suffering from cutaneous plasmacytosis after receiving the WIBP and BBIBP-CorV vaccine. According to the temporal relationship between the occurrence of symptoms and the change of symptom severity, it is indicated, but it has not been proved that the vaccine may be related to the patient’s cutaneous plasmacytosis.
Considering the number of cutaneous plasmacytosis casesis extremely small and no such adverse events have been reported so far [4,5], the patient’s diagnosis might be a pure coincidence. In addition, given it was weakly positive for anticentromere antibody, and positive for hepatitis B surface antigen and hepatitis B core antibody, we did not exclude the possibility that cutaneous plasmacytosis was induced by potential autoimmune diseases or hepatitis B. However, although the patient had already been infected by hepatitis B virus, she had no family history and had never had alike symptoms until vaccination, more importantly, the condition of the illness got worsened with the increasing number of vaccinations. And in a retrospective study on a group of 6 patients with plasmacytosis, none of those six patients were reported to have had been infected by the hepatitis B virus [3]. Notably, the patient’s skin lesions appeared rapidly after the third vaccination, but there was no significant deterioration after the first and second vaccination. Therefore, these findingsabove further suggested that the vaccine might be related to the patient’s diagnosis.
Conclusion
Here by, this case illustrates an extremely rare adverse event of the COVID-19 vaccine and also provides certain referential value for doctors to diagnose the disease of cutaneous plasmacytosis in the future. However, none of these can deny the tremendous benefits of COVID-19 vaccine, nor the corroborated safety and efficacy of WIBP‐CorV and BBIBP‐CorV.
Declarations
Acknowledgments: We thank the patient for granting permission to publish this information.
Conflict of interest disclosures: None reported.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Watanabe S, Ohara K, Kukita A, Mori S. Systemic plasmacytosis. A syndrome of peculiar multiple skin eruptions, generalized lymphadenopathy, and polyclonal hypergammaglobulinemia. Arch Dermatol. 1986; 122: 1314-1320.
- Tokura Y, Yagi H, Yanaguchi H, Majima Y, Kasuya A, et al. IgG4-related skin disease. Br J Dermatol. 2014; 171: 959-967.
- Honda R, Cerroni L, Tanikawa A, Ebihara T, Amagai M, et al. Cutaneous plasmacytosis: report of 6 cases with or without systemic involvement. J Am Acad Dermatol. 2013; 68: 978-985.
- Xia S, Zhang Y, Wang Y, Wang H, Yang Y, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. The Lancet Infectious Diseases. 2021; 21: 39-51.
- Xia S, Duan K, Zhang Y, Zhao D, Zhang H, Xie Z, et al. Effect of an Inactivated Vaccine Against SARS-CoV-2 on Safety and Immunogenicity Outcomes: Interim Analysis of 2 Randomized Clinical Trials. JAMA. 2020; 324: 951-960.