
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Corticospinal tract decussation alteration: A single case
of a healthy woman presenting with left fronto-parietal
intraparenchimal haemorrhage showing homolateral
symptoms and signs
Cane G1,2*; Mazzeo LA²; Vismara D²; Salmaggi A²
1Unit of Neurosurgery, Department of Clinical Surgical Diagnostic and Pediatric Sciences, University of Pavia, Pavia, Italy.
2Unit of Neurosurgery, Department of Neurosciences, Hospital A Manzoni, Lecco, Italy.
*Corresponding Author : Giorgio Cane
Unit of Neurosurgery, Department of Clinical Surgical Diagnostic and Pediatric Sciences, University of Pavia, Pavia, Italy.
Ph: +39 3286757806.
Email: cane.giorgio94@gmail.com
Received : Sep 14, 2022
Accepted : Oct 14, 2022
Published : Oct 21, 2022
Archived : www.jcimcr.org
Copyright : © Cane Gs (2022).
Abstract
Alterations in crossing CST pathways are rare findings which may cause diagnostic confusion and in some cases pose a real challenge. Some of these patients have a known genetic or congenital syndrome which correlates with CST crossing pattern alterations, but in many others the diagnosis is less intuitive due to the absence of conditions related.
Here in we present an isolated case of non decussating CST, presenting with homolateral symptoms after intracerebral fronto-parietal haemorrhage. The suspicion due to the symptomatology was then confirmed with DTI MR reconstructions.
Citation: Cane G, Mazzeo LA, Vismara D, Salmaggi A. Corticospinal tract decussation alteration: A single case of a healthy woman presenting with left fronto-parietal intraparenchimal haemorrhage showing homolateral symptoms and signs. J Clin Images Med Case Rep. 2022; 3(10): 2116.
Introduction
In healthy humans, about 75%-90% of the fibres of the Corticospinal tract (CST) cross the midline of the brain stem through the pyramidal decussation at the level of the medulla oblongata [1]. From there, the fibers of the CST travel through the lateral corticospinal tract and reach the neurons in the ventral horn of the grey matter of the spinal cord [1,2].
An uncrossed CST at the level of the pyramidal decussation is a rare anatomic variation and has been seldom found in healthy humans. Only seven cases have been described in formerly neurologically asymptomatic patients [3-9]. Furthermore, a partly uncrossed CST has been confirmed as the main anatomic pathology in rare genetic disorders, such as Congenital Mirror Movements (CMM) [10] and Horizontal Gaze Palsy with Progressive Scoliosis (HGPPS). Other raregenetic disorders may also occur with a crossing pathology of the CST (e.g., Dandy–Walker, Kallmann, or Joubert syndrome) [1].
Here, we review the literature on crossing pathologies of the CST from 1850 until today. We further present the case of a patient with acute speech disturbances and left-sided hemiparesis. Computed Tomography (CT), as well as diffusion-weighted Magnetic Resonance Imaging (MRI), revealed a left-sided ICH.
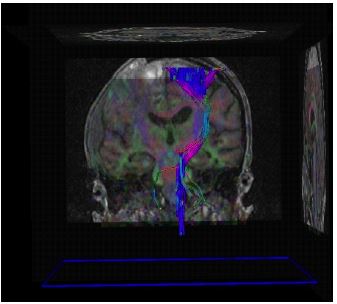
Subsequent Diffusion Tensor Imaging (DTI) with fiber tracking showed a highly asymmetric crossing of the CST at the level of the medulla oblongata. Thus, a partly uncrossed CST was identified as the anatomical substrate of the ipsilateral symptoms in this patient.
Background
CST pathologies in healthy humans
Crossing pathologies of the CST seem always to occur at the level of the medulla oblongata (pyramidal decussation) or below in the spinalcord, whereas the rest of the CST seems to develop normally [1,11,12].
There are no data available as to the prevalence of crossing pathologies in healthy humans. Since 1950, only seven previously healthy patients with uncrossed CST have been described. All seven patients had an unremarkable prior medical history and no pre-existing neurologic pathologies. Five of these cases presented with stroke symptoms and ipsilateral hemiparesis [3-7]; one had a cerebral tumour and ipsilateral paresis [8] and one showed ipsilateral motorevoked potentials during intraoperative monitoring of a vestibularschwannoma surgery [8].
Later, a study from Cuatico in 1979, suggested an ipsilateral motor innervation based on clinical findings, electroencephalography, and pneumoencephalography in another patient with [7]. Hosakawa et al. in 1996 demonstrated an uncrossed CST by somatosensory and motor evoked potentials and with a follow-up MRI showing ipsilateral Wallerian degeneration after thalamic hemorrhage [3]. The tenth case described was a patient with ipsilateral hemiparesis after putaminalhemorrhage, where functional MRI revealed ipsilateral activation through finger-tapping [5].
The only cases that visualized the uncrossed CST through DTI and fiber tracking were published by Alurkar et al. in 2012 [6], Ku et al. in 2017 [8], and Persad et al. in 2021 [9] where all described a completely ipsilateral course of the CST.
CST pathologies in genetic disorders
In addition to these rare acquired cases in previously healthy patients, crossing pathologies of the CST have been described in different congenital diseases. In these diseases, three possible anatomic variants have been described: (i) mainly ipsilateral CST with some crossing fibers at the pyramidal decussation, (ii) mainly ipsilateral CST with some crossing fibers at the spinal level, and (iii) completely ipsilateral CST with no crossing at all [1]. Furthermore, crossing pathologies constitute the main pathology only in two congenital conditions, CMM [10] and HGPPS [13-15]. CMM are caused by mutations of the genes DCC and RAD51 [16], where as HGPPS is caused by a mutation of the ROBO3 gene [14,15]. In the mouse model, all these genes have been shown to code for factors expressed by CST neurons, mainly responsible for guiding the neurons through the midline during embryonic development [1]. There is one substantial difference between the two diseases; whereas in HGPPS there is no crossing of the CST at all, in CMM some fibres of the CST still cross at the pyramidal level, resulting into the occurrence of mirror movements. Mirror movements seem to occur only when there are some crossing CST fibers left, but not if they do notcross at all. This is supported by other genetic diseases where patients with partly uncrossed CST (Kallmann, Klippel–Feil, Joubert, Möbius, and Gorlin syndromes) also present with mirror movements [11,17-19], where as patients with genetic diseases with no crossingat all (e.g., Dandy–Walker syndrome) do not [20]. Even though crossing pathologies of the CST have been described in these genetic syndromes, there are no data available on the frequency of occurrence or the clinical impact of these crossing pathologies in each of these syndromes.
Case report
The patient, a 52 yo woman, presented in the evening with dizziness and instability. Found at home by her husband on the floor, unresponsive and brought to our hospital DEA.
The patient results as an healthy woman with an history of neurosurgical operation at the age of 3 years for a left parieto-occipital lesion excision with an uncertain histologic diagnosis of arachnoid cyst.
Pathological history:
- at the age of 3 yo the patient was operated to remove a left parietal arachnoid cyst;
- in 2015 orthopaedic intervention for malleolus fracture;
- no chronic diseases known;
- right handed;
- dermal hipersensitivity to piperacillin/tazobactam in anamnesis;
- no pharmacotherapies or coagulopathies known.
At the presentation the patient was awake, non responsive, non executing easy tasks, with left hemiplegia and localizing painful stimulus on the right side of the body.
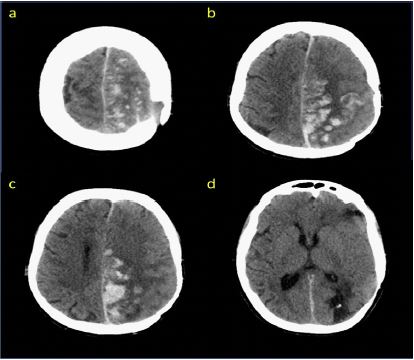
Executed in emergency brain CT scan which found left, fronto-parietal, intracerebral hemorrhage (Figure 1).
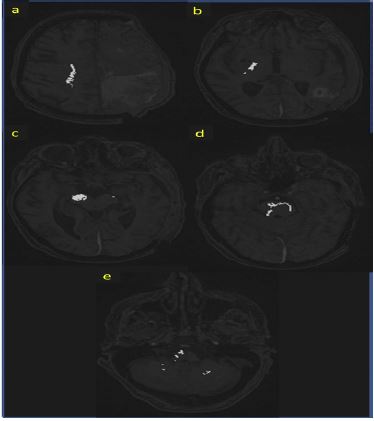
As a more detailed study a brain CT-angiography, panagiography and MR where made: “Large left frontal parenchimal hemorrhage independent from arterial perfusion territory. Inside the lesion was found the presence of pseudocystic formation showing haematic level. The SSS was open to the blood flow and both the internal carotids where fibrodysplastic”. After 24 h from presentation a rapid neurologic and neuroradiologic worsening which drove to an urgent operation of left fronto-parieto-temporal osterodural decompression and partial hemorrhage evacuation (Figure 2).
Due to the paucity of informations and clues, a brain tissue biopsy was made which found a morphologic aspect compatible with amyloid cerebral angiopathy (article under submission).
After the intervention a progressive neurologic improvement was seen: Patient became awake, responsive, executing, with aphasia, stable left hemiplegia but with less hyper tone.
After 20 days she showed a new neurologic worsening whit appearance of tension under the skin flap. At CT scan a new bleeding in the left hemisphere was found. In this case surgical indication wasn’t given.
The patient neurological outcome was poor and consisted in: Awake, spontaneous eyes opening, no responsiveness or execution; unstable eye contact, ciliary reflex present; left hemiplegia and localizing painful stimulus on the right side.
After all acute issues were resolved the patient was discharged to a long-term care center.
Conclusion
In acute conditions such as hemorrhagic stroke, CST pathology should be considered in case of discordant clinical findings. For neurosurgeons, the knowledge of genetic disorders that may be associated with an uncrossed CST, and the possibility of an uncrossed CST in patients with no known neurologic/genetic diseases, may be essential in an intraoperative setting, with need for neuromonitoring.
DTI is a potent imaging technique and allows a detailed examination of white matter pathways but is also prone to technical artefacts and has limitations. Resolving crossing fibers is not always possible and requires both adequate data acquisition and postprocessing.
Unfortunately, in our patient we did not conduct electrophysiologic studies (e.g., motor/sensory evoked potentials) due to poor clinical conditions.
References
- Welniarz Q, Dusart I, Roze E. The corticospinal tract: Evolution, development, and human disorders. Dev. Neurobiol. 2017; 77: 810–829.
- Mott FW. The Sensory Motor Functions of the Central Convolutions of the Cerebral Cortex. J. Physiol. 1894; 15; 464-i2.
- Hosokawa S, et al. Ipsilateral hemiplegia caused by right internal capsule and thalamic hemorrhage: demonstration of predominant ipsilateral innervation of motor and sensory systems by MRI, MEP, and SEP. Neurology. 1996; 46: 1146–1149.
- Yamamoto H, Bogousslavsky J. Ipsilateral hemiparesis and pyramidal tract abnormalities. Neurology. 1998; 50: 316.
- Terakawa H, et al. Ipsilateral hemiparesis after putaminal hemorrhage due to uncrossed pyramidal tract. Neurology. 2000; 54: 1801–1805.
- Alurkar A, et al. Ipsilateral stroke with uncrossed pyramidal tracts and underlying right internal carotid artery stenosis treated with percutaneous transluminal angioplasty and stenting. A rare case report and review of the literature. Neuroradiol J. 2012; 25: 237–242.
- Cuatico W. The phenomenon of ipsilateral innervation. One case report. J. Neurosurg. Sci. 23: 81–86.
- Ku J, et al. Ipsilateral Motor Innervation Discovered Incidentally on Intraoperative Monitoring: A Case Report. Neurosurgery. 2017; 80: E194–E200.
- Persad AR, Gould L, Norton JA, Meguro K, et al. Uncrossed corticospinal tracts presenting as transient tumor-related symptomatology. Acta Neurochir. (Wien). 2021; 163: 947–951.
- Méneret A, Welniarz Q, Trouillard O, Roze E, et al. Congenital mirror movements: from piano player to opera singer. Neurology. 2015; 84: 860.
- Filippopulos FM, et al. Uncrossed corticospinal tract in health and genetic disorders: Review, case report, and clinical implications. Eur. J Neurol. 2021; 28: 2804–2811.
- Carrasco Moro R, Castro Dufourny I, Martínez San Millán JS, Cabañes Martínez L, Pascual JM, et al. Ipsilateral hemiparesis: The forgotten history of this paradoxical neurological sign. Neurosurg. Focus. 2019; 7: E7.
- Haller S, Wetzel SG, Lütschg J. Functional MRI, DTI and neurophysiology in horizontal gaze palsy with progressive scoliosis. Neuroradiology. 2008; 50: 453–459.
- Abu Amero KK, al Dhalaan H, al Zayed Z, Hellani A, Bosley TM, et al. Five new consanguineous families with horizontal gaze palsy and progressive scoliosis and novel ROBO3 mutations. J Neurol. Sci. 2009; 276: 22–26.
- Bosley TM, et al. Neurologic features of horizontal gaze palsy and progressive scoliosis with mutations in ROBO3. Neurology. 2005; 64: 1196–1203.
- Gallea C, et al. RAD51 deficiency disrupts the corticospinal lateralization of motor control. Brain. 2013; 136: 3333–3346.
- Farmer SF, Ingram D A, Stephens JA, et al. Mirror movements studied in a patient with Klippel-Feil syndrome. J. Physiol. 1990; 428; 467–484.
- Krams M, et al. Kallmann’s syndrome: Mirror movements associated with bilateral corticospinal tract hypertrophy. Neurology. 1999; 52: 816–822.
- Mayston MJ, et al. Mirror movements in X-linked Kallmann’s syndrome. I. A neurophysiological study. Brain. 1997; 120: 1199–1216.
- Lagger RL. Failure of pyramidal tract decussation in the Dandy-Walker syndrome. Report of two cases. J. Neurosurg. 1979; 50: 382–387.