
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Metatypical basal cell carcinoma invasion of
the central nervous system
Arushi Thaper1*; Matthew Doran Bloom1; Astrid Marina Zorrilla1; Zachary A Taylor1; Vikash Sinha2; Coy Don Heldermon1
1Department of Medicine, University of Florida, Gainesville, FL, USA.
2Department of Radiology, University of Florida, Gainesville, FL, USA.
*Corresponding Author : Arushi Thaper, MD
Department of Medicine, University of Florida, USA.
Email: Arushi.Thaper@medicine.ufl.edu
Received : Sep 19, 2022
Accepted : Oct 17, 2022
Published : Oct 24, 2022
Archived : www.jcimcr.org
Copyright : © Thaper A (2022).
Abstract
Metatypical basal cell carcinoma is a rare skin cancer. Compared to basal cell carcinoma, this tumor type is more aggressive and has higher incidence of metastasis. We present the case of a 45-year-old female with metatypical basal cell carcinoma of the scalp with invasion of the central nervous system.
Keywords: Metatypical basal cell carcinoma; Skin cancer; Basal cell carcinoma; Central nervous system; Metastasis.
Citation: Thaper A, Bloom MD, Zorrilla AM, Taylor ZA, Sinha V, et al. Metatypical basal cell carcinoma invasion of the central nervous system. J Clin Images Med Case Rep. 2022; 3(10): 2118.
Introduction
Metatypical basal cell carcinoma is a rare subtype of basal cell carcinoma. Although grossly similar to basal cell carcinoma, it is more aggressive with a higher likelihood of metastases [1]. To date, metatypical basal cell carcinoma has been poorly defined both clinically and pathologically, with no general acceptance in the literature. However, studies have differentiated this tumor from basal cell carcinoma, especially in regards to its mitotic rate [2]. Given the aggressiveness of this variant, management often involves complex surgical planning. Chemotherapy, radiation and targeted therapy have also been used for non-surgical candidates [3]. We present the case of a 45-year-old female with metatypical basal cell carcinoma of the scalp with aggressive invasion into the central nervous system.
Case presentation
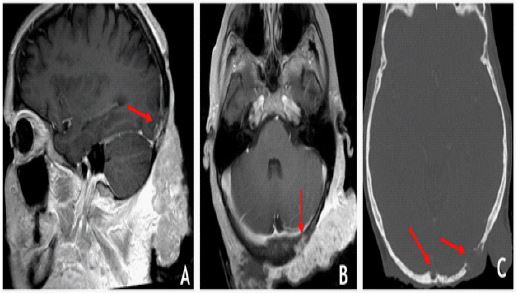
A 45-year-old female presented with bleeding, purulent drainage and larval colonization from a known metatypical basal cell carcinoma of the left occipital scalp. 1 year prior, she was found to have an unresectable, 13.7 cm x 3.2 cm exophytic, ulcerated mass that had been present for at least 6 months per the patient’s account (Figure 1). Histopathology showed poorly differentiated carcinoma with clear cell change, consistent with metatypical basal cell carcinoma. The mass invaded the muscumusculature, occipital skull and likely the underlying dura as seen on MRI and CT Imaging (Figure 2). She initially achieved disease stabilization for 6 months with vismodegib, a small-molecule inhibitor of the Hedgehog signaling pathway. She was then put on capecitabine for 4 months followed by 2 months of topical imiquimod cream.
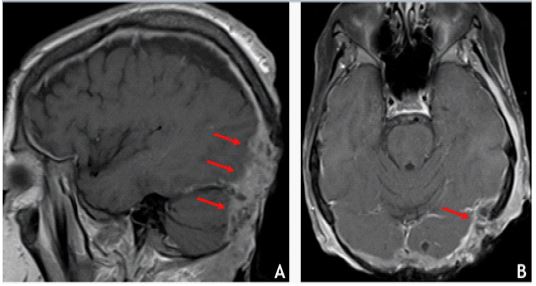
During the current hospitalization, she underwent a brain MRI revealing progressive disease with inferior and lateral extension into the left temporal scalp and ear. There was also direct tumor invasion of the occipital lobes (Figure 3). She did not have any neurological symptoms. Various treatment options were discussed, and she opted for palliative radiotherapy. She eventually transitioned to hospice care.
Discussion
Metatypical basal cell carcinoma is a rare non-melanoma skin cancer with features of both squamous and basal cell carcinoma. It is clinically indistinguishable from basal cell carcinoma and diagnosis relies on accurate histological evaluation. Underreporting may arise due to the rarity in diagnosis combined with the lack of awareness of the histological subtype [1].

In one study, the most commonly affected primary site was the cervico-facial area followed by the trunk, limbs and scalp. 10% of patients had ulceration and 2.5% had infiltrative lesions [2]. In another retrospective study, disease recurrences were common in up to 1/3 patients [3]. Regarding treatment, the standard of care is wide local excision [1] and it has been suggested that margins should be wider than that of a basal cell carcinoma [2]. Patients should be evaluated for local node involvement as well as distant sites of metastasis [1]. For patients who are not surgical candidates, radiotherapy, chemotherapy, or targeted therapy with vismodegib have been reasonable alternatives [4].
Metatypical basal cell carcinoma is considered an aggressive subtype of basal cell carcinoma. Cases may be under reported due to the rarity in diagnosis and unfamiliarity with this histological subtype [1]. Treatment involves wide local excision, with radiation, chemotherapy and targeted therapy as other options for non-surgical candidates [3].
References
- De Stefano A, Dispenza F, Petrucci AG, Citraro L, Croce A, et al. Features of biopsy in diagnosis of metatypical basal cell carcinoma (Basosquamous Carcinoma) of head and neck. Otolaryngologia Polska. 2012; 66: 419-423.
- Tarallo M, Cigna E, Frati R, Delfino S, Innocenzi D, et al. Metatypical basal cell carcinoma: A clinical re-view. Journal of Experimental & Clinical Cancer Research. 2008; 27: 1-6.
- Chaabane A, Bacha D, Ayachi K, Kilani H, Kanchel F, et al. Metatypical Basal Cell Carcinoma: A 6-Year Retrospective Study. Skinmed. 2019; 17: 24-28.
- Pabst A, Klinghuber M, Müller G, Vandersee S, Werkmeister R, et al. Extensive bony metastases from fa-cial metatypical basal cell carcinoma: A case report. British Journal of Oral and Maxillofacial Surgery. 2019; 57: 82-84.