
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Invasive ductal carcinoma of the breast presenting with
endometrial metastases in two patients
Arushi Thaper1*; Vikash Sinha2; Coy D Heldermon1
11Department of Medicine, University of Florida, Gainesville, FL, USA.
22Department of Radiology, University of Florida, Gainesville, FL, USA.
*Corresponding Author : Arushi Thaper, MD
Department of Medicine, University of Florida, USA.
Email: Arushi.Thaper@medicine.ufl.edu
Received : Sep 19, 2022
Accepted : Oct 18, 2022
Published : Oct 25, 2022
Archived : www.jcimcr.org
Copyright : © Thaper A (2022).
Abstract
We present 2 patients with invasive ductal carcinoma of the breast who had metastases to the endometrium. Both patients presented similarly with abnormal uterine bleeding. Gynecologic metastases are very infrequently seen amongst breast cancer patients, and even less frequently in patients with invasive ductal carcinoma by comparison to invasive lobular carcinoma. Our cases highlight the importance of considering metastatic disease as a potential diagnosis when breast cancer patients present with uterine bleeding.
Keywords: Breast cancer; Breast malignancy; Invasive ductal carcinoma; Endometrial metastasis.
Citation: Thaper A, Sinha V, Heldermon CD, et al. Invasive ductal carcinoma of the breast presenting with endometrial metastases in two patients. J Clin Images Med Case Rep. 2022; 3(10): 2119.
Background
In the United States, breast cancer is the second most common cause of cancer-related death in women, and globally it is the most common cause of cancer-related death in women [1]. More than 150,000 women in the United States live with a diagnosis of metastatic breast cancer [2]. Breast cancer most commonly metastasizes to the bone, liver, and lungs. Breast cancer metastasis to the gynecologic organs is uncommon. Conversely, metastatic disease found in the endometrial organs most frequently originates from other gynecologic sources. While invasive ductal carcinoma is the most common histologic subtype of breast cancer, the second most common subtype, invasive lobular carcinoma, more frequently presents with gynecological metastases. We present a case series of 2 breast cancer patients who were treated for invasive ductal carcinoma and presented years later with endometrial metas-tases manifesting with abnormal uterine bleeding.
Case series
Case 1
Case presentation: A 47-year-old female presented for abnormal uterine bleeding. Her medical history included left breast invasive ductal carcinoma (Grade I, ER/PR positive, HER-2 negative, strongly reactive for e-cadherin, T1cN0M0) diagnosed 6 years previously. At that time, her genetic testing was negative for mutations and sentinel lymph node biopsy was negative for metastasis. She was treated with left nipple-sparing mastectomy with clear margins, followed by recon-struction and tamoxifen for 5 years. Her oncotype score was 19. Her last menstrual period was 3 years prior to symptom onset. The presenting episode initially started as abdominal cramping which eventually escalated to in-clude abnormal uterine bleeding with the passage of clots.
Investigations: Her gynecologist performed a bimanual exam and found her uterus to be anteverted and enlarged (14-16 weeks size) with an irregular contour. An endometrial aspirate was sent for pathologic exam. Pathology results were consistent with metastatic adenocarcinoma of breast origin (ER positive, PR negative, HER-2 equivocal, e-cadherin intact). This was further supported by the tumor cells being strongly and diffusely reactive to GATA-3 and mam-moglobin, weakly reactive to GCDFP and CK7 and non-reactive to PAX8. Laboratory results were significant for hemoglobin of 9.8 g/dL (baseline 12-13 g/dL), and CA-125 of 132 U/mL (normal range 0-35 U/mL). Complete metabolic panel was within normal limits. Based on these findings, the patient underwent whole body PET-CT which showed a markedly thickened and FDG avid endometrium, a large and globular uterus and cervix, mild to moderate right-sided hydronephrosis and hydroureter secondary to an obstructing pelvic process, and large bilateral adnexal masses with layering blood products (Figure 1). It should be noted that FDG avidity of the endometrium can be seen as a non-specific finding.
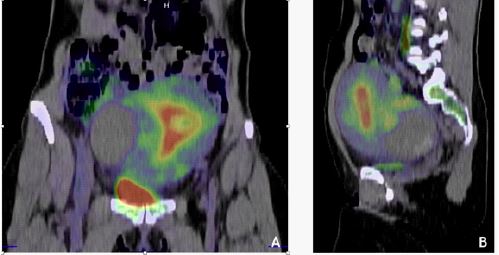
Coronal (A) and sagittal (B) PET/CT images demonstrate increased FDG uptake within the endometrium.
Differential diagnosis: Given that this patient was treated with tamoxifen, endometrial carcinoma was high on the differential for her uterine bleeding. Additional differential diagnoses included benign polyp, leiomyoma, other primary gynecologic malig-nancy (e.g. cervical) and, far less likely, metastatic disease.
Treatment: The patient underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, and cystoscopy. Pathology from the procedure once again confirmed metastatic breast adenocarcinoma with bilateral lymph node involve-ment. Afterwards, she underwent adjuvant chemotherapy with dose-dense doxorubicin for 4 cycles, followed by paclitaxel weekly for 12 weeks. Upon completion of chemotherapy, she was started on oral letrozole.
Outcome and follow-up: It has now been 2 years since recurrence, resection, and chemotherapy for this patient’s metastatic breast adeno-carcinoma. She continues to follow closely with medical oncology for surveillance. She is still taking oral letrozole. Her most recent whole body PET-CT showed no evidence for any active or recurrent tumor.
Case 2
Case presentation: A 56-year-old female presented with abnormal uterine bleeding. Her medical history includes hypertension, diabetes, obesity, and invasive ductal carcinoma of breast (ER 100, PR 100, HER-2 1+, positive for e-cadherin, T1N1M0) diagnosed 3 years prior. At that time, she was treated with central lumpectomy with clear margins. Adjuvant chemotherapy was recommended after surgical excision, however the patient declined and elected to only pursue endocrine therapy with anastrozole to preserve quality of life. Surveillance imaging including mammogram, MRI, and PET-CT were all benign. Her presenting episode of abnormal uterine bleeding began with spotting and progressed to heavy daily blood loss severe enough to cause lightheadedness. Her last menses was 8 years prior to symptom onset.
Investigations: Speculum exam performed at her gynecologist’s office revealed active bleeding, a large, vascular, polyppolypoid structure occluding the endocervical canal, and a smaller endocervical polyp as well. The smaller polyp was removed and sent for pathologic exam which resulted as a benign endocervical polyp. CBC showed Hgb 11.4 g/dL (baseline 11-12 g/dL). The patient subsequently underwent hysteroscopy with endometrial sampling and polypectomy. Pathology results were consistent with metastatic carcinoma, most similar to breast carcinoma (ER/PR positive, HER-2 negative). The tumor cells were compared to prior breast carcinoma pathology and found to be morphologically similar, GATA3 positive (diffuse and strong), with rare mammaglobin, and negative for PAX5 and PAX8. Afterwards, the patient underwent whole body PET-CT which showed FDG avidity in the endometrium in addition to adenopathy in the right neck and mediastinum, increased FDG update in the right thyroid, and metastatic lesions in the liver and bones (Figure 2).
Differential diagnosis: Much like the first patient, the differential diagnosis for this patient’s abnormal uterine bleeding initially included leiomyoma, benign endocervical polyps, endometrial carcinoma, other primary gynecologic malignancies, and metastatic disease.
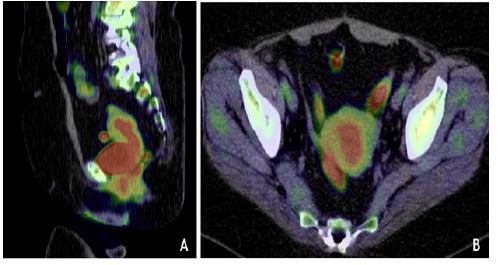
Sagittal (A) and axial (B) PET/CT images demonstrate increased FDG uptake within the endometrium.
Treatment: The patient presented to medical oncology again for further treatment and was started on fulvestrant, palbociclib and zolendronic acid. Her thyroid findings from the PET-CT were followed with a thyroid ultrasound which showed dominant right mid thyroid lobe nodule measuring up to 1.2 cm, with follow up recommended for 1 year.
Outcome and follow-up: The patient is currently being actively treated with the aforementioned therapy regimen. She is tolerating the regimen well except for an increase in creatinine requiring dose reduction of zoledronic acid and mild anemia.
Discussion
Breast cancer typically metastasizes to the liver, lungs, and bone. Endometrial metastases, such as the endometrial and cervical lesions presented in these cases, are far less common. Mazur et al. studied 325 female patients with gynecologic metastatic disease and found that the most common primary source of malignancy was ovarian or endometrial [3]. The most common source of extra-gynecological metastases to the endometrial tract were gastro-intestinal malignancies (37.6%) followed by breast carcinoma (34.9%). Additionally, the ovaries and vagina are the most common gynecological sites of metastasis, whereas endometrial and cervical metastasis, as seen in these cases, are less common [3].
As in both of these cases, the most common presenting symptom of endometrial metastasis is abnormal uterine bleeding. Often, patients treated for hormone receptor positive breast cancers are maintained on medications such as tamoxifen (as in case 1), a selective estrogen receptor modulator. Tamoxifen can cause endometrial hyperplasia and increases risk for primary endometrial carcinoma, both of which can also present as abnormal uterine bleeding, making the diagnosis of endometrial metastatic disease more challenging. Diagnosis is clarified using biopsy [4]. Endometrial hyperplasia is less common with anastrozole, an aromatase inhibitor, used by the patient in case 2 prior to her disease recurrence. In fact, anastrozole has been proven to be effective for treatment of endometrial hyperplasia [5]. Few case reports have been published of patients on anastrozole therapy who have had gynecologic metastases, and even fewer with invasive ductal carcinoma rather than invasive lobular carcinoma [6]. Thus, it is important for clinicians to consider the possibility of metastatic disease as an etiology for abnormal uterine bleeding in patients treated for breast cancer.
Additionally, these cases are unusual because both patients have invasive ductal carcinoma. Invasive ductal carci-noma is by far the most common histologic subtype of breast cancer, however, a study by Lamovec et al. which analyzed autopsy records for 261 breast cancer patients found that invasive lobular carcinoma metastasizes more frequently to the endometrial organs than invasive ductal carcinoma [7]. Additionally, Borst et al. used a tumor registry to analyze metastatic sites of 2605 breast cancer patients and found that the rate of metastasis to the gy-necological system was 4.6% in invasive lobular carcinoma and only 0.8% for invasive ductal carcinoma [8].
We have presented 2 interesting and unusual cases of endometrial metastases from invasive ductal carcinoma presenting as abnormal uterine bleeding. Despite the low rate of endometrial metastatic disease in breast cancer patients, it is important for clinicians to consider the possibility of metastatic disease when breast cancer patients present with uterine bleeding in order to ensure prompt and effective treatment.
References
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer Statistics, 2021. CA Cancer J Clin. 2021; 71: 7-33.
- Waks AG, Winer EP. Breast Cancer Treatment: A Review. JAMA. 2019; 321: 288-300.
- Mazur MT, Hsueh S, Gersell DJ. Metastases to the female genital tract. Analysis of 325 cas-es. Cancer 1984; 53: 1978-1984.
- Maymon R, Czernobilsky B, Lifschitz Mercer B, et al. Metastatic breast carcinoma mani-festing as postmenopausal uterine bleeding in a patient on tamoxifen therapy. Eur J Gynaecol On-col. 1996; 17: 319-321.
- Agorastos T, Vaitsi V, Pantazis K, et al. Aromatase inhibitor anastrozole for treating endo-metrial hyperplasia in obese postmenopausal women. Eur J Obstet Gynecol Reprod Biol. 2005; 118: 239-240.
- Arslan D, Tural D, Tatlı AM, et al. Isolated uterine metastasis of invasive ductal carcinoma. Case Rep Oncol Med. 2013; 2013: 793418.
- Lamovec J, Bracko M. Metastatic pattern of infiltrating lobular carcinoma of the breast: An autopsy study. J Surg Oncol. 1991; 48: 28-33.
- Borst MJ, Ingold JA. Metastatic patterns of invasive lobular versus invasive ductal carcino-ma of the breast. Surgery. 1993; 114: 637-641.