
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
The value of preoperative FDG PET/CT in detecting groin metastases in vulvar cancer patients
Cecilie Hedegaard Hansen1*; Ole Mathiesen2; Kirsten Bouchelouche3; Katja Dahl4
1Department of Gynecology, Aarhus University Hospital, Denmark.
2Department of Gynecology, Aarhus University Hospital, Denmark.
3Department of Nuclear Medicine & PET Centre, Aarhus University Hospital, Denmark.
4Department of Gynecology, Aarhus University Hospital, Denmark.
*Corresponding Author : Cecilie H Hansen, MD
Department of Gynecology, Aarhus University Hospital, Denmark.
Email: 201307260@post.au.dk
Received : Sep 19, 2022
Accepted : Oct 18, 2022
Published : Oct 25, 2022
Archived : www.jcimcr.org
Copyright : © Hansen CH (2022).
Abstract
Objective: This retrospective study aimed to evaluate the diagnostic value of preoperative18F-Fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography (PET/CT) in detecting groin Lymph Node (LN) metastases in newly diagnosed vulvar cancer patients.
Methods: In the period 01.01.2014 to 31.12.2018, we retrospectively collected data by reviewing the medical record of 237 patients with diagnosed vulvar cancer referred to Aarhus University Hospital. In the study, 108 patients were included for final analysis. Inclusion criteria was that all women should have histology from the groin with either Inguinofemoral Lymph Node (IFLN) dissection, Sentinel Lymph Node (SLN) procedure or Ultrasound (US)-guided biopsy. In addition, all included patients underwent FDG PET/CT for primary staging of vulvar cancer before operation. Sensitivity, specificity, Positive and Negative Predictive Values (PPV and NPV) in predicting LN metastases were calculated in the overall study population. Results from FDG PET/CT were compared with histopathology as reference standard.
Results: All included women underwent a standardized patient investigation program. This included a thorough gynecological examination, a Magnetic Resonance Imaging (MRI) and FDG PET/CT scan. We found that PET/CT had a sensitivity of 90.9% (95% CI 70.8-98.9%), specificity of 67.4% (95% CI 56.5-77.2%), PPV of 41.7% (95%CI 27.6-56.8%) and a NPV of 96.7% (95% CI 88.5-99.6%).
Conclusion: In this relatively large single-center study, we found that FDG PET/CT has a high sensitivity and a high NPV in detecting LN metastasis in the groin. This supports, that FDG PET/CT is a valuable imaging modality in the management of vulvar cancer patients.
Keywords: Vulvar cancer; FDG PET/CT; Sentinel lymph node procedure; Lymph node metastases.
Citation: Hansen CH, Mathiesen O, Bouchelouche K, Dahl K, et al. The value of preoperative FDG PET/CT in detecting groin metastases in vulvar cancer patients. J Clin Images Med Case Rep. 2022; 3(10): 2120.
Introduction
Vulvar cancer accounts for 4-5% of gynecological cancers and 1% of all cancers in women [1]. In Denmark about 80-120 women are diagnosed annually with the disease, and in 90% the histology is of squamous cell type [2]. In Denmark patients are treated at one of two gynecological oncological centers, Aarhus University Hospital (AUH) or Rigshospitalet, responsible for treating vulvar cancer patients. The typical pattern of spread in vulvar carcinoma is via Lymph Nodes (LNs). Lymphatic drainage from the vulva is primarily to the inguinofemoral region and secondarily to the external and internal iliac LN stations. Hematogenous spread is relatively rare. Size and stromal invasion and particularly groin and distant metastases are important prognostic factors, and for that reason, detecting LN metastases is of highest clinical interest. In absence of groin and distant metastases, the 5-year overall survival rate is 86%, while presence of groin metastases and spread to surrounding tissues leads to a decrease in overall survival to approximately 51% [3]. Knowledge of LN status can be obtained by removal of all the inguinal LNs by Inguinofemoral Lymph Node (IFLN) dissection.
However, at the time of diagnosis approximately 70% of the IFLNs are negative for metastases and the procedure is associated with high rate of wound infection and lower limb morbidity, especially lower limb lymphedema, which can be a chronic and a disabling condition [4].
Therefore, current research in vulvar cancer is focused on identifying patients in whom IFLN dissection could be unnecessary in the attempt to reduce morbidity following IFLN dissection. In women with radiologically negative groin LNs and tumor size less than 4 cm, Sentinel Lymph Node (SLN) procedure is considered a safe and sufficient procedure with less post-operative complications compared to full groin lymphadenectomy [5-7].
18F-Fluorodeoxyglucose (FDG)-Positron Emission Tomography/Computed Tomography (PET/CT) is widely used for evaluation, staging, and restaging of many cancers. However, only few mainly small studies with conflicting results have evaluated the role of FDG PET/CT for detecting LN metastases in vulvar cancer [8]. Recently, a retrospective study with 160 vulvar cancer patients reported good sensitivity and Negative Predictive Value [NPV] in discriminating metastatic from non-metastatic LNs [9]. According to the NCCN (National Comprehensive Cancer Network) Guidelines, whole body FDG PET/CT should be considered for vulvar cancer tumors >2 cm or if metastases are suspected due to abnormal physical examination [10].
The aim of this study was to investigate the diagnostic value of preoperative FDG PET/CT in detecting groin LN metastases in newly diagnosed vulvar cancer patients.
Methods
Study design
This study is retrospective and has been approved by the Danish Data Protection Agency.
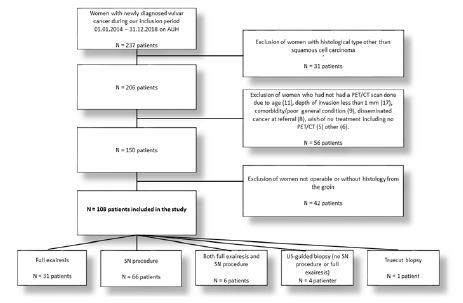
We collected data on women diagnosed with vulvar cancer at AUH, in the period 01.01.2014 to 31.12.2018. To be included, the women should have followed the usual investigation pro program. Excluded from the study were patients having histological types other than squamocellular carcinoma. Furthermore, we excluded patients without an FDG PET/CT performed, due to various reasons e.g., very high age and poor general condition, depth of invasion less than 1 mm, comorbidity or known disseminated cancer when referred to the hospital. Some patients did not have an FDG PET/CT done, since they did not wish further investigations. Finally, patients not operable or without histology from the groin were excluded. See flowchart in Figure 1.
The medical record of each patient included in the study was reviewed and data concerning tumor- and patient characteristics were collected (Table 1 and 2). For BMI and age we calculated the median. For the remaining background data regarding tumor- and patient characteristics, we calculated the percentage contribution for each characteristic.
Table 1: Table presenting patient characteristics of all 108 included women.
| Characteristics | No. | % |
|---|---|---|
| Age at diagnosis | ||
| Median (range) | 67.5 (27-87) | |
| BMI | ||
| Median BMI* (range) | 26.15 (15.1-51.3) | |
| HPV status | ||
| Positive | 8 | 7.4% |
| Negative | 35 | 32.4% |
| Not available | 65 | 60.9% |
| Lichen Sclerosus | ||
| Yes | 38 | 35.2% |
| No | 14 | 13% |
| Not available | 56 | 51.9% |
| Smoking status | ||
| Smoker | 31 | 28.7% |
| Ex-smoker | 19 | 18% |
| Never smoked | 56 | 51.9% |
| Not available | 2 | 1.9% |
| Diabetes | ||
| Yes | 22 | 20.4% |
| No | 86 | 79.6% |
Patient investigation program
At AUH the patient investigation program is standardized and organized as an interdisciplinary collaboration between different specialties. The investigation program and treatment are developed according to national guidelines based on present evidence.
Patients with biopsy-verified vulvar cancer, are referred to the Department of Gynecology, AUH. All biopsies are reviewed by a specially trained gyn-onco pathologist. If depth of invasion, defined by the pathologist, is > or = 1 mm, the patient is examined with a Magnetic Resonance Imaging (MRI) and a FDG PET/CT scan. Scans are used to describe local spread of the tumor including LN metastases to the groin, and distant metastases.
The pathological results and scans are discussed at a multidisciplinary conference with participants of highly specialized onco-gynecologists, oncologists, pathologists, specialists in nuclear medicine, CT and MRI radiologists.
Table 2: Tumor characteristics.
| Tumor characteristics | No | % |
|---|---|---|
| Focal site of tumor | ||
| Multifocal | 17 | 15.7% |
| Unifocal | 91 | 84.3% |
| Surgery of the groin | ||
| SN | 66 | 61.1% |
| Full exairesis | 31 | 28.7% |
| Only US-guided biopsy | 4 | 3.7% |
| SN in one groin, full exairesis in the other groin | 6 | 5.6% |
| True cut biopsy | 1 | 0.9% |
| Distance of tumor from midline | ||
| Over 1 cm | 27 | 25% |
| Under 1 cm | 80 | 74.1% |
| Not specified | 1 | 0.9% |
Subsequently, the patient investigation program includes a thorough gynecological examination, if needed in general anesthesia. The examination is performed by an onco-gynecologist and an oncologist with the purpose of evaluating tumor size and localization, any involvement of urethra and/or rectum or anus, uni- or multifocal lesions and distance to midline. These tumor characteristics are registered in the medical record for each patient.
Surgical procedure
Treatment depends on the results of the MRI, FDG PET/CT and the gynecological examination. Surgery is considered if the tumor is restricted to vulva and not involving urethra or rectum, except from the most distal 1 cm of urethra. If the depth of invasion is ≥1 mm, surgery of the groin with either SLN procedure or IFLN dissection, will be offered.
If groin LNs are palpable and malignancy suspected, or malignancy is suspected on MRI and/or FDG PET/CT, an US-guided biopsy of the suspicious node is performed. When biopsy-verified LN metastases are found, SLN procedure is not performed.
Otherwise, SLN procedure is offered when tumor is < 4 cm, unifocal and depth of invasion is > or = 1 mm. Indications for primary IFLN dissection are when tumor is > or = 4 cm and depth of invasion >1 mm, or if tumor is multifocal [11].
If tumor is located < 1 cm from the midline SLN procedure or IFLN dissection is performed bilaterally. Deviations from the patient investigation program can be made due to individualization because of for example age or the general condition of the patient.
FDG PET/CT
FDG PET/CT images were performed with a 64-slice General Electric Discovery 690 PET/CT (General Electric Healthcare, Little Chalfont, Buckinghamshire, UK). Capillary blood glucose was measured to ensure glucose levels were < 150 mg/dL before scanning. After a minimum of 6 hours of fasting, the patients were injected i.v. with 4 MBq/kg 18F-FDG. After injection, the patients rested for 60 min., whilst ingesting an iodide-containing per oral contrast media and water (16 mL Omnipaque (240 mg iodide/mL) in 500 mL water). Shortly before the scan, the patients were asked to empty their bladders. At 60 min. after the injection of FDG, a high dose CT with contrast i.v was performed followed by PET with a scan time of 2-5 min. per bed position (depending on Body Mass Index [BMI]) from the base of the skull to the upper thigh with the patient supine. Unless patients had contraindications to i.v contrast, an automated injection was performed of an iodide-based contrast medium in a weight-adjusted dose at 0.8 mL/kg (Omnipaque 300 mgl/ml). CT images were acquired at 120 kV and reconstructed into a 512 x 512 matrix with a slice thickness 2.5 mm. The attenuation corrected PET data were reconstructed iteratively using a three-dimensional Ordered-Subset Expectation Maximization (OSEM) algorithm. Images were reconstructed into a 400x400 matrix with a slice thickness of 2 mm. Voxel size in the final reconstructed PET-image was 2 x 2 x 2 mm.
PET images were transferred to a clinical software viewing platform (Hybrid viewer, version 1.4, Hermes Medical Solutions, Stockholm, Sweden) and made available for analysis, interpretation, and description by adiagnostic team consisting of an experienced radiologist and an experienced specialist in nuclear medicine, both with many years of experience in reporting FDG PET/CT. Increased FDG uptake in LNs (SUVmax higher than liver SUVmax) were reported as suspicious of malignancy. On CT, LNs measuring more than 10 mm in the short axis diameter were suspicious of malignancy.
Statistical analyses
The histological results from the investigation of LNs were considered the golden standard. We found the histological results by exploring the medical journals and we used histology from either SLN, IFLN dissection, US-guided biopsy or truecut biopsy. We compared the histological findings with the results of the FDG PET/CT scan to finally calculate the Positive Predictive Value (PPV), Negative Predictive Value (NPV), sensitivity and specificity in predicting groin LN metastases. These were our primary outcomes. Stata 16.1 analytic software (Stata Corp LP, College Station, TX) was used for the statistical analyses.
Regarding patient characteristics, we analyzed data by calculating percentages of characteristics concerning HPV, Lichen Sclerosus, smoking status and diabetes. For data concerning BMI and age, we found the median including the range.
Results
During our inclusion period, 237 patients with a diagnose of unspecified vulvar cancer were consecutively examined at AUH. 129 patients were excluded not fulfilling the inclusion criteria, mainly due to histological type other than squamous cellular carcinoma (31 patients) or due to lack of histology from the groin/not operable (42 patients). The primarily reason for lack of histology was due to disseminated disease on FDG PET/CT and therefore referral to the Oncological Department for treatment with radiation therapy and/or chemotherapy. For further exclusion criteria, see flowchart in Figure 1. Overall, 108 women were analyzed. All underwent vulvar surgery with either IFLN dissection (31 patients), SLN procedure (66 patients), both IFLN and SLN (6 patients), only US-guided biopsy (4 patients) or truecut biopsy (1 patient).
For data concerning patient characteristics, we found that the median age was 67.5 years (range 27-87). For BMI the median was 26.15 (range 15.1-51.3). Most of the patients had never smoked (51.9%), though still a high proportion were current smokers (28.7%). For further characteristics, see Table 1. For data concerning tumor characteristics, we found that tumors were mainly unifocal (84.3%) and placed less than 1 cm (74.1%) from the midline. Finally, histology was primarily obtained from lymph nodes removed using SLN procedure (61.1%). See Table 2.
Primary outcomes
The primary outcomes are illustrated in Table 3.
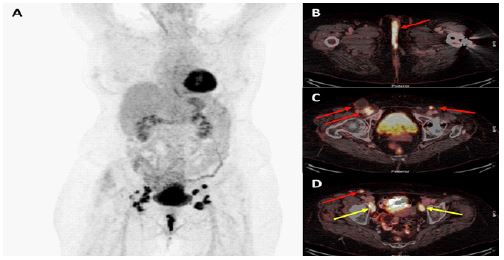
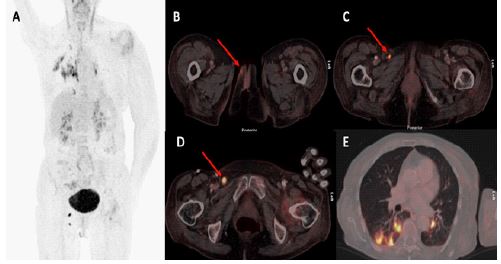
We found that FDG PET/CT had a high sensitivity of 90.9% (95% CI 70.8-98.9%) and an even higher NPV of 96.7% (95% CI 88.5-99.6%). We found a quite lower specificity of 67.4% (95% CI 56.5-77.2%) and a PPV of 41.7% (95% CI 27.6-56.8%) (Table 3). Our primary outcomes are based on a patient-by-patient basis, meaning we counted and analyzed on patients and not on numbers of LNs in the groins. Figure 2 and 3 show example of primary staging with FDG PET/CT in two vulvar cancer patients.
Table 3: Primary outcomes: Sensitivity, specificity, PPV and NPV.
| Primary outcomes | Histological metastatic spread to the groin | No histological metastatic spread to the groin | |
|---|---|---|---|
| PET/CT positive | N = 20 | N = 28 | PPV: 41.7% (95% CI 27.6-56.8%) |
| PET/CT negative | N = 2 | N = 58 | NPV: 96.7% (95% CI 88.5-99.6%) |
| Sensitivity: 90.9% (95% CI 70.8-98.9%) | Specificity: 67.4% (95% CI 56.5-77.2%) |
Discussion
The purpose of this study was to investigate the efficacy of FDGPET/CT to detect LN metastases to the groin in newly diagnosed vulvar cancer patients. Groin LN metastases are an important prognostic factor, since metastases to the groin decreases the 5-year overall survival rate considerably [3]. Considering the importance and worse prognosis of false negative results due to under treatment, we chose to focus on sensitivity and NPV as our primary data for analysis. The more false negative results, the lower sensitivity and NPV. The study showed that FDGPET/CT had a high sensitivity of 90.9% (95% CI 70.8-98.9%) and an even higher NPV of 96.7% (95% CI 88.5-99.6%). Contrary, we found a low specificity of 67.4% (95% CI 56.5-77.2%) and a PPV of 41.7% (95%CI 27.6-56.8%) in detecting groin LN metastases.
Few previous studies have investigated the role of FDG PET/CT in detecting groin LN metastases in vulvar cancer patients using histopathology as reference. These studies have reported varying results with sensitivities ranging from 50 to 100% and NPV from 57 to 100% (2; 9; 12-19). This variation may be explained by e.g. the differences in study designs and different reference standard. Some studies were retrospective, like our study, while others were performed prospectively. A consideration is that in rare diseases, data may be collected from various centers to allow a higher number of included patients introducing potential bias. In our study, we did not collect data from different centers, though vulva is relatively rare disease. Instead we collected data only from AUH securing homogeneity and patient being treated after exact same patient investigation program.
The high NPV and sensitivity in our study is in accordance with the results reported in a Dutch study by Collarino et al [20]. Like most of the other studies, this is a prospective study with a small study group consisting of 33 patients, all scheduled for IFLN dissection. As in our study, they report a high sensitivity of 95.2% and NPV of 96.4%. Moreover, their data results in a relatively low specificity of 75% and PPV of 69%.
Similar results are reported in another recent study by Rufini et al. from 2021, which is methodologically very similar to our study being a single center study with a retrospective design [9]. Opposite other studies this study is characterized by a relatively large study population of 160 included patients. LN status were evaluated using two qualitative methods; PET alone and FDG PET/CT. A sensitivity of 78.9%, specificity of 78.2%, PPV of 61.2% and NPV of 89.4% were found when combining PET and CT. Though, sensitivity is not as high as in our study, the NPV for detection of metastatic lymph nodes were still high.
A high NPV indicates that a negative FDG PET/CT with great accuracy predicts the absence of LN metastases to the groin. The high NPV found in our study, as well as in other similar studies, supports the clinical importance of FDG PET/CT in selecting vulvar cancer patients with unifocal tumors less than 4 cm for groin SLN procedure [9]. The low PPV means, that a positive FDG PET/CT is not highly predictive for groin LN metastases. Thus, a positive FDG PET/CT needs to be interpreted with caution.
In our study, we also found a low PPV of 41.7% indicating that a PET positive LN in the groin not necessarily means metastasis to the LNs. This is in contrast to the results from a study by Cohn et al [13]. They analyzed their results on a patient-by-patient basis, like we did in our study, as wells as by a groin-by-groin basis. On a groin-by-groin basis they found FDG PET/CT to have a sensitivity of 67%, specificity of 95%, PPV of 86%, and NPV of 86%. On a patient-by-patients basis they report a sensitivity of 80%, specificity of 90%, PPV of 80% and a NPV of 90% [13]. However, the authors report a quite lower sensitivity, which was due to more false-negative findings, especially on a groin-by-groin basis. It is interesting and worth noticing, that when analyzing on a groin-by groin basis instead of patient-by-patient basis, results are affected significantly. The authors suggest that false negative findings might be due to either micro-metastases or completely tumor necrotic LNs which are metabolically inactive, leading to false-negative PET findings. Similar, it is well known that reactive benign LNs can have FDG uptake, resulting in false positive results. This is a pitfall when analyzing on a patient-by-patient basis as well as on a groin-by-groin basis. All patients underwent groin lymphadenectomy, either unilateral or bilateral.
FDG PET/CT is widely used in the management of different cancers. The possibility of combining anatomical as well as functional imaging is the main advantage when using this imaging modality. The benefits range from diagnosing, treatment planning and to evaluating a treatment response. FDG PET/CT can identify even small signs of cancer very early resulting in early diagnosis and staging. FDG PET/CT may detect small but not enlarged LN metastases, whereas both MRI and CT rely on size and structural characteristics. No other commonly used imaging modalities such as Ultrasound (US), CT or MRI are just as precise [21]. The advantages of FDG PET/CT are widely known and has therefore become standard procedure in the clinical management of different cancers world-wide [21]. Our study support the significant role of FDG PET/CT in the investigation program of vulvar cancer patients.
Though, there are also well-known challenges associated with the use of FDG PET/CT. FDG PET/CT demonstrates the FDG uptake (a marker of glucose metabolism) in the tissue, which is increased in most malignancies, but increased FDG uptake can also be seen in benign, and in normal tissue with physiological uptake. Consequently, increased FDG uptake is not specific for metastases [22]. Beside metastases, FDG uptake is correlated with inflammatory activity or infection, limited uptake in very small tumors (micro-metastases), hyperglycemia and hyperinsulinemia resulting in altered uptake or reactive LNs due to e.g. earlier groin surgery [23]. These pitfalls are important knowledge for the physician interpreting the images [24], but it is also important for the surgeons when using FDG PET/CT as part of the standard procedure in the management of vulvar cancer patients.
Knowledge about advantages and disadvantages of FDG PET/CT has also been important when interpreting data from our study. A high NPV is one of our main results. This indicates that a PET negative LN most likely does not contain metastases. This may have therapeutic consequences. According to current protocol, a negative FDG PET/CT is followed by SLN procedure if other criteria for SLN procedure are fulfilled. Though SLN procedure is considered a safe method, side effects may occur as it is a surgical procedure [5]. Associated side effects are for instance wound infection and lower limb morbidity, though the risk of side effects is lower than surgery with full IFLN dissection. According to data from our study, patients with a negative FDG PET/CT most likely have a healthy groin, since few are false-negative. This leads to questioning whether it is in fact necessary with surgery of the groin, especially in the case of high-risk patients (e.g.very high age, severe comorbidity, high BMI), where the risk of complications due to surgery is increased. In addition, these patients might have difficulties tolerating any complications. Though, on the other hand, current guidelines are based on older published studies, especially the first Groningen International Study on sentinel nodes in vulvar cancer (GROINSS-V) [7] from which indications for SLN are mainly based. SLN procedure is considered an overall safe method when performed by highly specialized surgeons (5; 25). Furthermore, metastases to the groin is the most important prognostic factor, meaning overlooking metastases can be fatal [3]. Under treatment of false-negative patients consequently worsening the prognosis could justify possible overtreatment of this group. A final consideration concerning the high NPV in our study is the potential possibility of expanding the criteria for SLN procedure. To avoid morbidity due to IFLN dissection, SLN procedure might be performed on vulvar cancer patients also with multifocal disease and/or tumors larger than 4 cm if the PET/CT is negative. Evidence to guide such an extension of indications for SLN procedure is of course needed and might be investigated in future studies.
A low PPV is a result of false-positive FDG uptake in non-malignant LNs. This means, that the finding of a positive LN on FDG PET/CT scan does not necessarily correlate with metastases to the groin. As mentioned, benign reactive LNs may have increased FDG uptake. This is important knowledge prior to planning of further treatment strategy for the patient. The finding of false-positive results in the groin can have a negative impact by resulting in unnecessary concerns, hospital visits, further examinations, IFLN dissection and subsequent morbidity.
False-positive findings can be due to increased FDG uptake in benign LNs following vulvar biopsy or shaving, which may lead to difficulty in interpretation of metastases. High levels of FDG uptake in large, necrotic and inflamed tissues leading to false-positive results seem to be the major limiting factor to the effectiveness of using whole body PET/CT in the management of vulvar cancer patients [22]. Thus, it is important to be aware of common pitfalls when reporting FDG PET/CT in vulvar cancer patients [24].
Another consideration with the routine use of FDG PET/CT as part of the patient investigation program is incidental findings as a result of scanning the whole body [26]. The possibility of finding distant metastases of vulvar cancer is obviously beneficial, although seldom. Though, in some cases, by searching the whole body for metabolic and anatomic alterations, this may result in findings of unexpected malignancies [26]. It could have a positive impact by potentially resulting in earlier diagnosis leading to earlier treatment of the malignant finding. However, the findings may also be insignificant, due to FDG uptake in non-malignant conditions. Since unexpected findings cannot be neglected, patients might undergo unnecessary concerns and time-consuming processes. These might include invasive procedures, also associated with potential side effects and complications in the diagnosis of cases with incidental findings.
Our study had some limitations. The data are based on a single center study. It could be beneficial since the clinical investigators are often continuously involved. Though, a single center trial is often associated with a relatively smaller study population. Especially vulvar cancer studies are often characterized by relatively few included patients due to the rare occurrence of the disease.
A great strength of this study is the homogeneity. In Denmark and in our study only a few pathologists and a few surgeons are managing the investigation program and treatment of vulvar cancer patients. All patients are discussed at highly specialized MDT conferences (gynecologists, oncologists, pathologists, specialists in nuclear medicine, CT and MRI radiologists). Thus, patients are treated by the same highly specialized team, working after the same protocol, meaning the patients are examined the same way. This ensures high standard and high quality in the investigation program, which strengthen the study. However, despite highly specialized team and SLN considered as golden standard, it is worth questioning whether the histological result is always correct. According to the GROINSS-V study [7], SLN procedure is a safe method in early stage vulvar cancer in diagnosing metastases to the groin. Still, the histological result depends on both the surgeon and the pathologist. Even though the highly specialized team has a great routine and expertise, failures may happen. Malignant tissue is removed by the surgeon based on a predefinition of the area, but some patients might be more difficult operating, e.g patients with a high BMI. In those cases, there is a risk that the surgeon is not able to find the SLN. Furthermore, there is a risk of overlooking small metastases by the pathologist.
A final great strength is the use of Civil Personal Registration (CPR) number which is the Danish form of social security number. This ensures great control of data on our included patients enabling us to have a secure access to identify all patients. Since data is registered in the electronically medical journal, we had the opportunity to review the journals safe and very thoroughly.
Conclusion
In our study, we found that primary staging with FDG PET/CT scan had a high sensitivity and a high NPV in detecting LN metastasis to the groin in vulvar cancer patients. Consequently, FDG PET/CT seems to be an effective imaging modality for better planning of patient groups suitable for surgical procedures, especially selection of patients for SLN procedure. Thus, FDG PET/CT may have an important implication on the clinical management of vulvar cancer patients. FDG PET/CT may allow high-risk patients to avoid surgical procedures to minimalize risk of morbidity in selected patients, and potentially allow for an expansion of indications of SLN procedure. However, due to the low PPV, a PET positive LN in the groin is not a guarantee for metastasis to the LNs, since FDG uptake in benign tissue can be seen. In addition, it might be associated with uncertainty, unnecessary concerns, hospital visits, further examinations, IFLN dissection and subsequent morbidity.
Available evidence on the impact of FDG PET/CT in detecting LN metastases in vulvar cancer patients is currently sparse. Thus, the role of FDG PET/CT in vulvar cancer patients need to be further evaluated in larger prospective multicenter trials.
Highlights
- FDG PET/CT is increasingly used for primary staging and detection of recurrence in vulvar cancer patients.
- There are only sparse data on the efficiency of PET/CT in vulvar cancer patients.
- Our data support FDG PET/CT as being effective for primary staging of vulva cancer patients and therefore useful for better therapy planning of patient groups suitable for surgical procedures.
Declarations
Conflict of interest: The authors have no funding and conflicts of interest to disclose.
Author contribution section: KD and OM conceived the idea to the study. KD, OM and CH designed the study. CH collected the data and presented data for analysis. KD presented analysis tools and performed the statistical analysis for our primary outcomes. CH analyzed on background information. CH and KB designed the figures. CH was the lead author on designing and writing the manuscript with contributions to sections from all co-authors. KD, OM and KB supervised the project and KD was the main supervisor. All authors reviewed the results, contributed to the final manuscript and approved the final version.
References
- Zweizig S, Korets S, Cain JM. Key concepts in management of vulvar cancer. Best practice & research. Clinical obstetrics & gynaecology. 2014; 28: 959-966.
- Dolanbay M, Ozcelik B, Abdulrezzak U, Serin IS, Kutuk MS, et al. F-18 fluoro-D-glucose (FDG)-Positron Emission Tomography (PET)/Computed Tomography (CT) in planning of surgery and sentinel lymph node screening in vulvar cancers. Archives of gynecology and obstetrics. 2016; 293: 1319-1324.
- Board CnE. 2021. Vulvar Cancer: Statistics. https://www.cancer.net/cancer-types/vulvar-cancer/statistics
- Land R, Herod J, Moskovic E, King M, Sohaib SA, et al. Routine computerized tomography scanning, groin ultrasound with or without fine needle aspiration cytology in the surgical management of primary squamous cell carcinoma of the vulva. Int J Gynecol Cancer. 2006; 16: 312-317.
- Collarino A, Fuoco V, Garganese G, Pereira Arias-Bouda LM, Perotti G, et al. Lymphoscintigraphy and sentinel lymph node biopsy in vulvar carcinoma: Update from a European expert panel. European journal of nuclear medicine and molecular imaging. 2020; 47: 1261-1274.
- Skanjeti A, Dhomps A, Paschetta C, Tordo J, Giammarile F, et al. Sentinel Node Mapping in Gynecologic Cancers: A Comprehensive Review. Seminars in nuclear medicine. 2019; 49: 521-533.
- Oonk MH, van Hemel BM, Hollema H, de Hullu JA, Ansink AC, et al. Size of sentinel-node metastasis and chances of non-sentinel-node involvement and survival in early stage vulvar cancer: results from GROINSS-V, a multicentre observational study. The Lancet. Oncology. 2010; 11: 646-652.
- Triumbari EKA, de Koster EJ, Rufini V, Fragomeni SM, Garganese G, et al. 18F-FDG PET and 18F-FDG PET/CT in Vulvar Cancer: A Systematic Review and Meta-analysis. Clin Nucl Med. 2021; 46: 125-132.
- Rufini V, Garganese G, Ieria FP, Pasciuto T, Fragomeni SM, et al. Diagnostic performance of preoperative [(18)F] FDG-PET/CT for lymph node staging in vulvar cancer: A large single-centre study. European journal of nuclear medicine and molecular imaging. 2021; 48: 3303-3314.
- Koh WJ, Greer BE, Abu Rustum NR, Campos SM, Cho KR, et al. Vulvar Cancer, Version 1.2017, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network: JNCCN. 2017; 15: 92-120.
- Opdateret juni 2018. Retningslinier for visitation, diagnostik, behandling og kontrol af vulvacancer. http://www.dgcg.dk/index.php/component/content/article/81-arbejdsgruppe/178-horing-for-retningslinier-for-vulvacancer
- Lin G, Chen CY, Liu FY, Yang LY, Huang HJ, et al. Computed tomography, magnetic resonance imaging and FDG positron emission tomography in the management of vulvar malignancies. European radiology. 2015; 25: 1267-1278.
- Cohn DE, Dehdashti F, Gibb RK, Mutch DG, Rader JS, et al. Prospective evaluation of positron emission tomography for the detection of groin node metastases from vulvar cancer. Gynecol Oncol. 2002; 85: 179-184.
- Kamran MW. Whole-body [18F] fluoro-2-deoxyglucose positron emission tomography scan as combined PET-CT staging prior to planned radical vulvectomy and inguinofemoral lymphadenectomy for squamous vulvar cancer: A correlation with groin node metastasis. European journal of gynaecological oncology. 2014; 35: 230-235.
- Robertson NL, Hricak H, Sonoda Y, Sosa RE, Benz M, et al. The impact of FDG-PET/CT in the management of patients with vulvar and vaginal cancer. Gynecol Oncol. 2016; 140: 420-424.
- Garganese G, Collarino A, Fragomeni SM, Rufini V, Perotti G, et al. Groin sentinel node biopsy and (18)F-FDG PET/CT-supported preoperative lymph node assessment in cN0 patients with vulvar cancer currently unfit for minimally invasive inguinal surgery: The GroSNaPET study. Eur J Surg Oncol. 43: 1776-1783.
- Crivellaro C, Guglielmo P, De Ponti E, Elisei F, Guerra L, et al. 18F-FDG PET/CT in preoperative staging of vulvar cancer patients: Is it really effective? Medicine (Baltimore). 2017; 96: e7943.
- Collarino A, Garganese G, Valdes Olmos RA, Stefanelli A, Perotti G, et al. Evaluation of Dual-Timepoint (18)F-FDG PET/CT Imaging for Lymph Node Staging in Vulvar Cancer. J Nucl Med. 2017; 58: 1913-1918.
- Oldan JD, Sullivan SA. Positron emission tomography-computed tomography for inguinal nodes in vulvar cancer. World journal of nuclear medicine. 2018; 17: 139-144.
- Collarino A, Garganese G, Valdés Olmos RA, Stefanelli A, Perotti G, et al. Evaluation of Dual-Timepoint (18)F-FDG PET/CT Imaging for Lymph Node Staging in Vulvar Cancer. J Nucl Med. 2017; 58: 1913-1918.
- Cazzato RL, Garnon J, Shaygi B, Koch G, Tsoumakidou G, et al. PET/CT-guided interventions: Indications, advantages, disadvantages and the state of the art. Minimally invasive therapy & allied technologies: MITAT: Official journal of the Society for Minimally Invasive Therapy. 2018; 27: 27-32.
- Perry LJ, Guralp O, Al Niaimi A, Zucker NA, Kushner DM, et al. False positive PET-CT scan and clinical examination in a patient with locally advanced vulvar cancer. Gynecologic oncology case reports. 2013; 4: 29-31.
- Griffeth LK. Use of PET/CT scanning in cancer patients: Technical and practical considerations. Proceedings (Baylor University. Medical Center) 2005; 18: 321-330.
- Kilcoyne A, Chow DZ, Lee SI. FDG-PET for Assessment of Endometrial and Vulvar Cancer. Seminars in nuclear medicine. 2019; 49: 471-483.
- Achimas Cadariu P, Harter P, Fisseler Eckhoff A, Beutel B, Traut A, et al. Assessment of the sentinel lymph node in patients with invasive squamous carcinoma of the vulva. Acta Obstet Gynecol Scand. 2009; 88: 1209-1214.
- Saif MW, Tzannou I, Makrilia N, Syrigos K. Role and cost effectiveness of PET/CT in management of patients with cancer. The Yale journal of biology and medicine. 2010; 83: 53-65.