
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
False occult hepatitis B virus infection with negative
HBsAg while positive HBeAg & overt DNA levels:
Case report and literature review
Qiankun Xuan1#; Sufeng Qiang2#; Xiaoyu Yu1; Zhouxiang Zhang2; Simin Yang1; Xiaona Li2; Wei Zhang2; Guangbo Li1*; Fei Fu2*
1Department of Laboratory Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai 200123, China.
2Department of Obstetrics and Gynecology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai 200123, China.
#Authors contributed equally to this work.
*Corresponding Author : Guangbo Li
Department of Laboratory Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai 200123, China.
Email: ligb2008@126.com
Fei Fu
Department of Obstetrics and Gynecology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai 200123, China.
Email: fufei0814@126.com
¶These authors contributed equally to this work.
Received : Sep 19, 2022
Accepted : Oct 18, 2022
Published : Oct 25, 2022
Archived : www.jcimcr.org
Copyright : © Guangbo L and Fei F (2022).
Abstract
Background: Occult Hepatitis B Infection (OBI) is characterized by the detection of Hepatitis B Virus (HBV) DNA in serum (usually HBV DNA < 200 IU/ml) or liver but negativity for hepatitis B surface antigen. The diagnosis of OBI is based on the sensitivity of assays used in the detection of HBV DNA and HBsAg. HBsAg assays with inadequate sensitivity or inability to detect HBV S variants may lead to a false negative HBsAg result and misdiagnosis of OBI in people with overt HBV infection. An OBI patient was followed 4 years with the analysis of HBV detection.
Methods: The Human Leucocyte Antigen (HLA)-A2 genotypes were determined by 2% agarose gel electrophoresis. The pre-S and S protein sequences were detected by sequencing analysis. The HBV markers and HBV DNA sequence and α-determinant of HBsAg were analyzed in the longitudinal sera, the whole follow up period was 4 years.
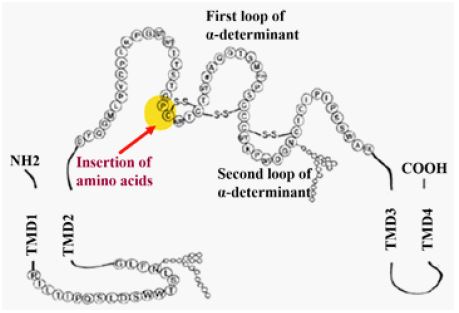
Results: The HBsAg was negative while HBV DNA level is comparable to overt infection, the HBeAg and HBsAb are positive at a low level. The pre-S and S protein sequencing analysis showed an insertion of four amino acids at 120~124 location next to antigenic determinant. The cloning analysis of the α determinant of HBsAg showed a unique immune escape mutant, there are insertion of four amino acids affects the formation of disulfide bond and then the formation of loop. Meanwhile, this insertion site is in Polymerase/Reverse Transcriptase Domain (RT).
Conclusions: Considering the overt HBV DNA infection and S-escape variants, this patient was a false OBI infection. No matter OBI or false OBI, all are difficult to diagnosed due to mutations in the S gene and low prevalence in clinical practice, Positive HBeAg and detectable HBV level are key clues to identify whether it is relative with OBI. Test for α determinant of HBsAg is key evidence to exclude whether it is a real OBI.
Keywords: Occult hepatitis B infection; Hepatitis B surface antigen; Hepatitis E antigen.
Citation: Xuan Q, Qiang S, Yu X, Li G, Fu F, et al. False occult hepatitis B virus infection with negative HBsAg while positive HBeAg & overt DNA levels: Case report and literature review. J Clin Images Med Case Rep. 2022; 3(10): 2121.
Introduction
A European Association for the Study of the Live (EASL) endorsed international workshop on occult HBV infection was held in Taormina (Italy). 2008 to review the biology and clinical implications of OBI [1]. After 10 years, “Update of the statements on biology and clinical impact of occult hepatitis B virus infection” was published to reach a consensus about OBI in Journal of Hepatology 2019 [2]. Clinical physicians are not familiar with the diagnosis and disease characteristics of OBI due to the low prevalence of OBI and slowly progress in the update of OBI Taormina statement. Occult HBV Infection (OBI) is defined as the presence of HBV DNA in the liver and/or HBV DNA in the blood of people who test negative for hepatitis B surface antigen (HBsAg) [2]. Recently published meta-analysis show the global prevalence of OBI is only 0.82% (95% CI 0.69 to 0.96) in general population. And the reported prevalence in china is similar with it, as low as 0.88% in general population [3]. As 2019 Taormina OBI statement described, OBI Prevalence rates have varied from as low as < 1% to as high as 87% but these results need to be interpreted with caution, because a number of factors can influence rates of OBI including the particular risk group studied, sampling issues, assay sensitivity, and the prevalence of HBsAg in the geographical region in which the study was conducted. Higher rates have also been found in individuals with risk factors for HBV infection, e.g., those coinfected with Hepatitis C Virus (HCV) (15%~33%) or Human Immunodeficiency Virus (HIV) (10%~45%), people who inject drugs (45%), and people on dialysis (27%). Prevalence rates are also higher in patients with HCC (62%), cryptogenic cirrhosis (32%), or those who have undergone liver transplantation (64%). In carefully conducted studies of blood donors, HBV DNA was detected in 0% to 4.6% of those who were HBsAg-negative and anti-HBc positive, with or without anti-HBs, with a median prevalence of 1%.
Let’s have a look at the diagnostic criteria of OBI, both 2008 and 2019 OBI Taormina statement were point out that the detection of HBV DNA in the blood or the liver of HBsAg negative individuals. While few people noticed the HBV DNA level requirement was very low < 200 IU/ml (about 1,000 copies/ml) since 2008 version. Cases with serum HBV DNA levels comparable to those usually detected in the different phases of serologically evident (overt) HBV infection have to be considered as ‘‘false” OBI and the identification of S-gene variants is essential for a correct diagnosis and for the possible clinical implications [1]. Since the mutation in HBsAg was first recognized in 1990, several HBV variants with residue substitutions, deletion, or insertion in the α determinant have emerged worldwide in various conditions. Such variants may result in immune prophylaxis failure and false negative in detection of HBsAg. Therefore, the use of multivalent anti-HBs antibodies in the HBsAg assays is strongly recommended for optimal detection of these variants.
Here we described one “OBI”patients who were negative for HBsAg with positive HBeAg and HBV DNA overt infection for 4ys, at last the S antigen variation was confirmed, which reminded us that the patient was a false OBI.
Case report
70y-old woman, hospitalization for cerebral ischemia caused by hypertension and appeared abnormal hepatitis B markers pattern during routine hospitalization detection in Dec 2017. HBV serologicmarkers, detected by the commercial qualitative Enzyme Immunoassay (EIA) kits (CMIA, Architect System, Abbott Laboratories), were HBsAg negative and Anti-HBc/ Anti-HBe negative, but positive for anti-HBs (>1000 mIU/ml) and HBeAg (60.64 S/Co). Serum HBV DNA level, detected by a real-time PCR kit (Sheng Xiang Biotech) with Roche Z480 Real-Time PCR System was found 3.82 × 104 IU/mL, all liver function tests were generally normal, such as ALT (13 U/l), AST (26 U/l), total bilirubin level (9.7 μmol¬¬/l), PT (12.2 s), INR (1.01), FIB (3.4 g/l), APTT (24.6 s), TT (18.5 s), AFP (2.16 ng/ml). All autoimmunity indexes were normal. She denied any history of HBV infection and family HBV infection history. Her vaccination history of hepatitis B is not known. She denied any history of blood transfusion, jaundice, and any liver disease. She never been treated with interferon or anti-HBV nucleoside/nucleotide analogs, Additionally, she denied any risk factors for HBV infection such as HCV or HIV infection or inject drugs. During hospitalization in cardiovascular department, the patient was regard as OBI and assumed no need to receive CHB management because of the absence of HBsAg and normal ALT and AST. Since that the patient was hospitalization every year because of coronary atherosclerotic heart disease between 2017-2022. Due to her history of OBI the patient was reexamined hepatitis B markers during every hospitalization. HBV markers, liver function and liver B-ultrasound examination were recorded in the following 4 ys (Table 1). During the follow up period, the ALT and AST and total bilirubin levels were generally normal, and the last time HBV DNA level was detected 2.72 × 104 IU/mL in July 2021 which is comparable with the first time in 2017.
The laboratory department can’t explain why this patient can present with positive HBeAg situation in OBI. So they clone analysis of the α determinant of HBsAg showed a unique immune escape mutant, and there are insertion of four amino acids affects the formation of disulfide bond and then the formation of loop (Figures 1,2).
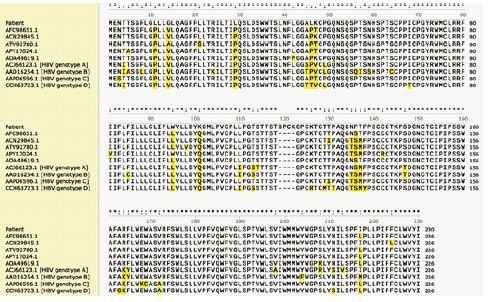
It is well known that there is an overlap of gene coding sequence between S protein and Pol protein. The 336~ 679 amino acids are the polymerase/reverse transcriptase domain of HBV. In this patient, this insertion of four amino acids in S protein also located in polymerase/reverse transcriptase domain indicating RT activity change during HBV infection (Figure 3).

Table 1: Biochemical, serological, and virological follow-up data.
| ref | 2017.12 | 2018.3 | 2019.4 | 2019.6 | 2019.8 | 2019.10 | 2020.6 | 2021.7 | |
|---|---|---|---|---|---|---|---|---|---|
| ALT (U/l) | < 40 | 13 | 36 | 11 | 14 | 31 | 24 | 17 | 13 |
| AST (U/l) | < 35 | 26 | 23 | 17 | 18 | 25 | 18 | 14 | 14 |
| TBIL (umol/l) | < 15 | 9.7 | 6.2 | 6.2 | 9.7 | 9.8 | 8.6 | 9 | 8.2 |
| PT (s) | 11~13 | 12.2 | 17.9 | / | / | / | / | / | 12.5 |
| INR | 0.8~1.5 | 1.01 | 1.55 | 0.97 | 1.09 | 0.96 | 0.93 | 0.93 | 1.06 |
| FIB (g/l) | 1.8~3.5 | 3.4 | 4.37 | / | / | / | / | / | 2.72 |
| APTT (s) | 25~31.3 | 24.6 | 30.8 | / | / | / | / | / | 2.72 |
| APTT (s) | 25~31.3 | 24.6 | 30.8 | / | / | / | / | / | 22.9 |
| TT (s) | 14~21 | 18.5 | 16.3 | / | / | / | / | / | 17.8 |
| AFP (ng/ml) | ≤7 | 2.16 | 1.77 | 1.67 | 1.75 | 1.86 | 1.79 | 2 | 1.7 |
| HBsAg (IU/ml) | < 1 | − (0.650) | − (0.377) | − (0.287) | − (0.330) | − (0.371) | − (0.288) | − (0.394) | − (0.397) |
| Anti-HBs (mIU/ml) | < 10 | >1000 | >1000 | >1000 | >1000 | >1000 | >1000 | >1000 | >1000 |
| HBeAg (S/Co) | < 1.0 | 60.64 | 134.4 | 62.69 | 27.9 | 17.72 | 12.79 | 10.4 | 11.82 |
| Anti-HBe (S/Co) | > 1.0 | − (1.3) | − (1.39) | − (1.1) | 0.994 | − (1.01) | − (1.06) | − (1.09) | − (1.03) |
| Anti-HBc (S/Co) | > 1.0 | 0.009 | 0.007 | 0.007 | 0.008 | 0.008 | 0.007 | 0.007 | 0.006 |
| HBV DNA (IU/ml) | / | 3.82E+04 | / | / | / | 6.82E+05 | / | / | 2.72×104IU/mL |
| HCV DNA(IU/mL) | < 50 | < 50 | < 50 | < 50 | < 50 | < 50 | < 50 | < 50 | < 50 |
| HIV antibody | Negative | Negative | Negative | Negative | Negative | Negative | Negative | Negative | Negative |
| HLA | / | HLA-A2 | / | / | / | HLA-A2 | / | / | HLA-A2 |
| B-ultrasound show: hepatic steatosis | - | Yes | - | Yes | Yes | - | - | Yes |
Table 2: The course of endoscopic treatments.
| Author year, country | Number of cases | Biochemical, virological characteristics | serological characteristics | HBV infection history and treatment experience | sequencing of the S gene |
|---|---|---|---|---|---|
| Z. Han et al. 2015, China [4] | Case 1 56 y-old man | ALT(U/I): normal AST(U/I): normal HBV DNA (IU/ml): 234-567 |
HBsAg: - HBsAb: + HBeAg:+ HBeAb: - HBcAb: + |
assumed to have resolved HBV infection. treatment naive | double mutations (A1762T and G1764A) in BCP no mutations in the pre C/C gene the α determinant sequences were all mutant type |
| Case 2 81-y-old man | ALT(U/I): normal AST(U/I): normal HBV DNA (IU/ml): 1130-135 |
HBsAg: - HBsAb: + HBeAg:+ HBeAb: - HBcAb: + |
diagnosed with HCC while not known HBV infection history. | double mutations (A1762T and G1764A) in BCP, no mutations in the pre C/C gene, three residue substitutions in the α determinant (Ile126The, The131Asn and Met133Thr) | |
| Y. H. Zhou et al. 2009, China [5] | Case 1 50-year-old man | ALT(U/I): normal AST(U/I): not done HBV DNA: 370–491 copies/ml |
HBsAg: - HBsAb: + HBeAg:+ HBeAb: - HBcAb: + |
Not known | the insertion is a perfect repeat of the preceding 15 nts. This insert resulted in 5 amino acids insertion between residues 128 and 129 in HBsAg, which is in the α determinant. HBV variant had mutations both in preS2 and S proteins. |
Finally, considering the overt HBV DNA infection and S-escape variants, this patient was confirmed as a false OBI infection after literature review. Post hoc analysis shows there was some important information ignored. Such as, noninfectious physicians did not pay attention to the patient’s HBV DNA overt infection, the conflict situation about positive HBeAg coexist with negative HBsAg is unusual in OBI. After all, Insensitivity commercial kits in detecting HBsAg mislead the diagnose especially for noninfectious physicians.
Literature review
To give an overview of OBI with positive HBeAg, we also performed a literature review in PubMed using the following keywords: (Occult hepatitis B [MeSH Terms]) AND (positive HBeAg) and choose Filters applied: Case Reports. Totally there are 10 articles and we identified only 3 articles reported appearance of HBeAg in OBI. (Table 2).
Discussion
The case we reported here was HBsAg negative but positive for HBeAg and HBV DNA overt infection, at first it was diagnosed as OBI because in the opinion of noninfectious physicians that HBsAg-/HBV DNA+ means OBI, they are not familiar with OBI due to the global prevalence of OBI is only 0.82% [3]. Even in 2018 AASLD CHB Guideline [7], there is no special section to discuss OBI. In 2017 EASL [8] and 2019 CHINA CHB Guideline [9], the definition of OBI was only mentioned HBsAg-/HBV DNA+ while not mentioned the requirement of HBV DNA < 200 IU/ml. only in the Taormina Statements of OBI 2008/2019 which highlight that HBV DNA is the only reliable diagnostic marker of OBI and the low HBV DNA required less than 200 IU/ml. The molecular basis of OBI can be explained as the low level of transcriptionally active cccDNA in OBI cases results in low or undetectable HBV RNA transcription and subsequent protein translation and expression. The low viral load is an indicator that the immune system is effective in controlling HBV (even if it is not definitively cleared) in most OBI patient. HBV DNA level is a key factor in determining treatment and follow-up, and false OBI patients could miss the optimal treatment. Hence, here is needed to highlight HBV DNA overt infection is a key clue to imply the possibility of active chronic hepatitis B. Because noninfectious physician is unfamiliar with this HBV DNA level requirement, it is very significant reporting this case.
The Taormina Statements of OBI also propose the concept of “False” OBI: Cases with serum HBV DNA levels comparable to those usually detected in the different phases of serologically evident (overt) HBV infection have to be considered as ‘‘false” OBI and are usually due to infection by HBV variants with mutations in the S gene (escape mutants) producing a modified HBsAg that is not recognized by some or all commercially available detection assays [1]. So, in this patient, the laboratory department clone analysis of the α determinant of HBsAg again because they think maybe the routine HBsAg assays with inadequate sensitivity or inability to detect HBV S variants may lead to a false negative HBsAg result. Our report reveals a unique insertion, and which shows that an insertion of amino acids at 120~124 location affects the formation of disulfide bond and then the formation of loop. It is well known that there is an overlap between S protein and Pol protein. Furthermore, we found this new insertion site is in Polymerase/reverse trantranscriptase domain indicating this insertion might involve in HBV pathogeny. Finally, considering the HBV DNA level was as high as 38,200 U/ml and confirmed immune escape mutant existed. Post hoc analysis show it is a false OBI based on the Taormina Statements.
Another thing needs to be pay attention is why HBeAg was persistent positive in this patient? It is well documented that HBeAg is associated with active replication and its appearance usually combined with HBsAg seroconversion and/or an increase of serum HBV DNA which means hepatitis B reactivated in OBI patients. As the result of literature search show, 7 out of 10 articles are described the reactivation of HBV [10-16], only 3 articles report 4 cases with HBeAg positive in confirmed OBI. Furthermore, all patients were containing S gene escape while only 2 cases reported HBV DNA level < 200 IU/ml. The first case Y.-H. Zhou et al reported in 2009 only discussed that the test of HBeAg may find out HBV carriers with mutant HBsAg and no more other comments about HBeAg positive. The second case Paparella C et al reported in 2010 claimed that they speculated that this patient either experienced a reactivation of a latent HBV infection, linked to the selection of escape mutants, or acquired an infection sustained by an HBV strain carrying one significant mutation in the ‘s’ gene. In both instances, the weak replication competence of this mutant or the neutralizing effect, albeit incomplete, of the pre-existing anti-HBs antibodies, justifies the occult pattern. Another 2 cases with HBV DNA above 200 IU/ml were described in one article published by Z. Han et al. in 2015. They think infection with the S gene escape mutants may also be the true OBI and regard the patients with negative HBsAg but positive HBeAg may represent a unique type of OBI. Test for HBeAg would be critical to identify such type of OBI.
We try to figure out whether HBeAg positive is a unique type of OBI or not. There is one recently published data collected 1,261 HBsAg-/HBV DNA+ blood donor plasmas identified in 29 blood centers located in 19 different provinces in China were shipped to the National Center for Clinical Laboratories (NCCL) between January 2010 and December 2013 [17], Samples confirmed as HBsAg-/HBV DNA+ (HBV DNA load < 200 IU/mL) which are anti-HBc and/or anti-HBs positive were classified into the OBI group. Samples that were both anti-HBc and anti-HBs negative were excluded in the absence of follow-up because a pre-seroconversion window period could not be ruled out. Among the 1,261 blood donors initially screened, 918 donors (72.8%) were proved to be OBI carriers. Host and viral markers were available for 906 OBI donors. But none of them was reported as HBeAg positive or discussed as unique OBI with positive HBeAg. We think this is the up to date the biggest OBI database and used the unified testing method of central laboratory which is more reliable than those case reports. Taken together, we think HBeAg positive with HBsAg-/HBV DNA+ is a key clue to imply the possibility of active chronic hepatitis B rather than a unique type of OBI while it needs more data to confirmed.
Last but not least is about how to manage these true or false OBI patient. For true OBI cases, Currently, antiviral therapy is not recommended for individuals with OBI in guideline and 2019 Taormina Statements update of OBI, which mentioned current drug to eradicate cccDNA and integrated HBV DNA is likely impossible. But OBI may result in transmission of HBV infection to blood or organ transplant recipients, and reactivation of HBV replication in patients receiving cancer chemotherapy or other immunosuppressive therapies, those at moderate risk may receive prophylactic antiviral therapy and if not, they should be closely monitored, and antiviral therapy initiated at the earliest sign of HBV reactivation. Risk stratification, indications for prophylactic antiviral therapy and frequency of monitoring are described in professional society guidelines.
Fewer discussion about False OBI case can be found, Not arnicola A, et al. reported a false OBI developed in a patient with psoriatic arthritis under infliximab and methotrexate therapy which published in 2014 [18]. The definition of False OBI is based on HBV infection occur without the warning of the seroconversion and achieved very high level of serum HBVDNA, although HBsAg is always undetectable, Interestingly, no matter this OBI patient was firstly treated with Infliximab plus Methotrexate in 2005 or this OBI patient firstly referred to the author in Dec 2010, theHBV DNA has not been performed either. Until half a year later the HBV DNA increased to 85554 U/mL with HBsAg still negative and it was reported as a False OBI.
Here we discussed false OBI is quite different with above cases, we want to highlight with clinical physicians to pay attention to “False” OBI which means it isan infectious CHB rather than OBI, because their DNA is overt infection and HBsAg is not recognized by some commercially available HBsAg assays. If we use the criteria of Chinese CHB guidelines published in 2019, patients with HBV DNA positive (>20 IU/ml), and ALT sustained elevated (>ULN) are the Indications for antiviral therapy. Recently published case report maybe can give us some pointers [19], it reported an “OBI” with positive HBeAg and HBsAg-/HBV DNA+ (2.32 × 103 IU/ml) and received ETV treatment, 4 weeks after initiation of ETV treatment HBV DNA dropped below 100 IU/ml (Minimum detection value line) and maintained for 6 months. After that the patient spontaneously stopped taking ETV for 6 month and then the HBV DNA rebounded to 2.79 × 103 IU/ml, the patient was encouraged to continue ETV treatment and achieve HBV DNA undetectable again. But unfortunately, the patient spontaneously stopped ETV therapy again and finally the patient had become a chronic HBV infection with drug resistance. In the discussion the author didn’t analysis why patient stop treatment again and again, it is reasonable to speculate that patient lack of disease cognition about OBI, as we know even in hepatitis B patients, it is difficult to manage long-term compliance, let alone OBI.
Limitations
There are limitations to the present study, first, it is a case report and never received the consultation from Infection department; second, this is the first time to report a unique insertion of amino acids at 120-124 location which need to verify the modifications of the HBsAg production pattern.
Conclusion
In conclusion, the significance of this case report is to highlight 2 update points with all infectious and non-infectious physicians, one is the diagnosis of OBI, which is based on the detection of HBV DNA less than 200 IU/ml since 2008 Taormina Statements published, another point is about CHB treatment criteria which patients with HBV DNA positive (>20 IU/ml) and ALT sustained elevated (>ULN) is the Indications for antiviral therapy.
Funding statement: This work was supported by Shanghai Municipal Commission of Health and Family Planning (No. PKJ2018-Y05).
Author statement: Qiankun Xuan, Guangbo Li: Conceptualization, Methodology. Sufeng Qiang: Data curation, Writing-Original draft preparation. Zhouxiang Zhang, Simin Yang, Xiaona Li: Data collection, Investigation. Wei Zhan: Documents management. Fei Fu, Xiaoyu Yu: Writing- Reviewing and Editing.
References
- Raimondo G, Allain JP, Brunetto MR, et al. Statements from the Taormina expertmeeting on occult hepatitis B virus infection. J Hepatol. 2008; 49: 652–657.
- Giovanni Raimondo, Stephen Locarnini, Teresa Pollicino, Massimo Levrero, Fabien Zoulim, et al. Lok. Update of the statements on biology and clinical impact of occult hepatitis B virus infection. Journal of Hepatology. 2019; 71: 397–408.
- Dong Ze Ji , Xiao Yu Pang , Dan Ting Shen , Shu Na Liu , Hemant Goyal , Hua Guo Xu, et al. Global prevalence of occult hepatitis B: A systematic review and meta-analysis, J Viral Hepat. 2022; 29: 317-329.
- Zhenge Han, Yong Liu, Jinshun Pan, Yongchun Bi, Jingli Liu, Yi-Hua Zhou, et al. Occult hepatitis B virus infection with positive hepatitis B e antigen. Clinica Chimica Acta. 2015; 438: 266–268.
- Yi-Hua Zhou, Jianxin Zhou, Lei Li, Yongchun Bia, Yong Liua, Jinshun Pana, Chao Wu, et al. A novel hepatitis B virus mutant coexisting with wild type virus in a carrier with negative HBsAg yet positive HBeAg and anti-HBs. Journal of Clinical Virology. 2009; 46: 363–366.
- Concetta Paparella, Filomena De Rosa, Roberta Longo, Giuseppina Cappiello, Antonella Ursitti, Marisa Rosa, Massimo Morosetti, Alberto Spanò. Appearance of HbeAg in an occult persistent hepatitis B virus infection. Intervirology. 2010; 53: 173–175.
- Norah A Terrault, Anna SF Lok, Brian J McMahon, Kyong Mi Chang, Jessica P Hwang, Maureen M. Jonas, Robert S Brown Jr., Natalie H Bzowej, John B Wong, et al. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Hepatology. 2018; 67: 4.
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017; 67: 370-398.
- Chinese Infection Disease. 2019; 37: 12.
- Fabbri, et al. Reactivation of occult HBV infection in an HIV/HCV Co-infected patient successfully treated with sofosbuvir/ledipasvir: A case report and review of the literature. BMC Infectious Diseases. 2017; 17: 182.
- Junichi Muraishi, Michihiko Shibata, Yuichi Honma, Masaaki Hiura, Shintaro Abe, et al. Reactivation of Occult Hepatitis B Virus Infection 27 Months after the End of Chemotherapy Including Rituximab for Malignant Lymphoma. Intern Med. 2017; 56: 1967-1971.
- Talotta, et al. Reactivation of occult hepatitis B virus infection under treatment with abatacept: A case report. BMC Pharmacology and Toxicology. 2016; 17: 17.
- Hiroshi Kamitsukasa, Masanobu Iri, Akihisa Tanaka, Shigeo Nagashima, Masaharu Takahashi, et al. Spontaneous reactivation of Hepatitis B Virus (HBV) infection in patients with resolved or occult HBV infection. Journal of Medical Virology. 2015; 87: 589–600.
- Wenjun Du, Zhaomin Zheng, Shaolei Han, Shumin Ma, Shijun Chen, et al. HBV reactivation in an occult HBV infection patient treated with prednisone for nephrotic syndrome: Case report and literature review. BMC Infectious Diseases. 2013; 13: 394.
- Susan A Feeney, Conall McCaughey, Alison P Watt, Moulod R El Agnaf, Neil McDougall, et al. Coyle1 reactivation of occult hepatitis B virus infection following cytotoxic lymphoma therapy in an anti-HBc negative patient. Journal of Medical Virology. 2013; 85: 597–601.
- Takaaki Imamura, Osamu Yokosuka, Tetsuhiro Chiba, Tatso Kanda, Hiroshige Kojima, et al. Lamivudine treatment in a patient with hepatitis B virus reactivation after allogenic peripheral bone marrow transplantation, Leukemia & Lymphoma. 2005; 46: 6: 915-917.
- Lu Zhangac, Le Chang, Syria Laperche, Huimin Jia, Junpeng Zhao, Xinyi Jiang, et al. Occult HBV infection in Chinese blood donors: Role of N-glycosylation mutations and amino acid substitutions in S protein transmembrane domains. Emerging Microbes & Infections. 2019; 8: 1337-1346.
- A Notarnicola, F Iannone, G Lopalco, M Covelli, G Lapadula, et al. A false occult hepatitis B virus infection developed in a patient with psoriatic arthritis under infliximab and methotrexate therapy. Reumatismo. 2013; 65: 298-301.
- Yuan C, Peng J, Xia R, He J, Qiu T, Yao Y, et al. Reactivation of Occult Hepatitis B Virus Infection During Long-Term Entecavir Antiviral Therapy. Front. Microbiol. 2022; 13: 865124.