
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Linitis prostatica: A unique case of circumferential
narrowing of the rectum
Benjamin Schmeusser1*; Joseph Wiedemer2; Eric Fichtenbaum3
1Wright State University, Boonshoft School of Medicine, Dayton, OH, USA.
2Department of Urology, Brown University School of Medicine, Providence, RI, USA.
3Ohio Health Urology, Columbus, OH, USA.
*Corresponding Author : Benjamin Schmeusser
Boonshoft School of Medicine, Wright State University, 3640 Colonel Glenn Hwy, Fairborn, OH 45324, Dayton, OH, USA.
Phone: 513-910-4355
Email: schmeusser.2@wright.edu
Received : Sep 19, 2022
Accepted : Oct 19, 2022
Published : Oct 26, 2022
Archived : www.jcimcr.org
Copyright : © Schmeusser B (2022).
Keywords: Prostate cancer; Linitis plastica; Metastasis; Rectum.
Citation: Schmeusser B, Wiedemer J, Fichtenbaum E. Linitis prostatica: A unique case of circumferential narrowing of the Rectur. J Clin Images Med Case Rep. 2022; 3(10): 2122.
Introduction
Linitis plastica is a rare desmoplastic phenomenon typically seen secondary to metastatic gastric cancer. First identified in 1779 and often referred to as “leather bottle stomach”, this finding is most often seen in female patients of Asian descent and suggests a poor prognosis. Histopathological findings of linitis plastica consist of malignant infiltrate with sub-mucosal hypertrophy in muscular and connective tissues resembling bands of filaments similar to linen, hence “linitis.” Linitis plastica is almost never associated with prostate cancer with fewer than 5 known cases ever published in the medical literature, all of which manifest in the rectum. Previous cases have described typical findings including a characteristic “target-sign” on contrast-enhanced Computed Tomography (CT) imaging and follow-up Magnetic Resonance Imaging (MRI) studies, which were only first reported in 2018. We present an extremely rare case of secondary linitis plastica from metastatic prostate cancer that highlights a myriad of clinical consequences in respect to modern day oncologic workups.
Case description
A 67 year-old Hispanic man was admitted for severe diarrhea. Past medical history included a 30 pack year smoking history and urinary retention secondary to benign prostatic hyperplasia, effectively managed with tamsulosin and finasteride. On digital rectal examination, the patient was noted to have a diffusely enlarged and firm prostate. Furthermore, his rectum was found to be diffusely narrowed with a lumen of about 1 cm and a circumferential mass located at the base of the prostate. Though the remainder of his laboratory evaluation was normal, a subsequent prostate specific antigen level of 199.4 ng/dL supported a diagnosis of prostate cancer.
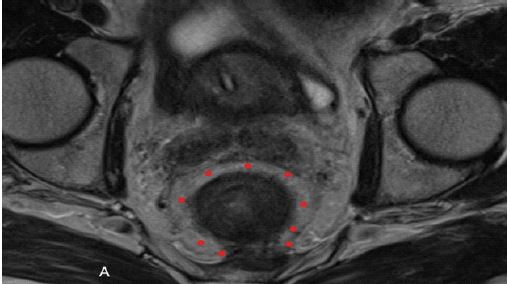
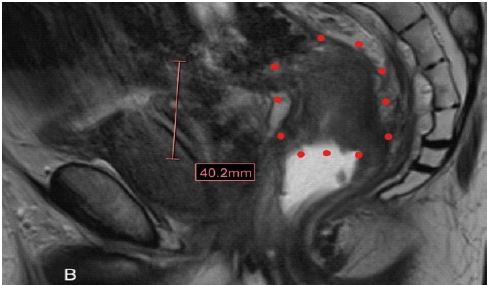
CT imaging revealed enlarged right iliac pelvic lymph nodes, and rectal narrowing with a 1 cm lumen and proximal obstruction. Dual-energy X-ray absorptiometry scan was negative for bone metastases. An MRI of the pelvis was obtained (Figures 1 and 2), which represents a “target-sign” appearance consistent with linitis plastica of the rectum. Separate tissue biopsies of both rectum and prostate confirmed a diagnosis of metastatic prostate adenocarcinoma. The patient was referred to medical oncology for further follow-up and was started on androgen deprivation therapy.
Discussion
This case and imaging represents rare metastasis of prostate cancer to the rectum, producing findings of linitis plastica of the rectum. Linitis plastica broadly refers to any gastrointestinal organ or hollow structure experiencing a diffuse narrowing and loss of pliability associated with inflammation, primary malignancy, or metastatic processes [1,2]. Most commonly, linitis plastica describes a rare morphologic variant of gastric cancer (leather bottle stomach); however, when associated with the rectum, primary linitis plastica has an incidence of < 0.1% of all colon cancers [3] and more often occurs as a metastatic process, such as from the stomach (most commonly), breast, prostate, gallbladder, and bladder [4-6]. We believe that this case strongly merits discussion in the academic community given its rare incidence, vast treatment implications, and possibly increased identification given prostate imaging and trends in prostate cancer screening.
To the best of our knowledge, there have been fewer than 5 reported cases of linitis plastica of the rectum secondary to prostate cancer metastasis [2,7]. In a 2018 report, a 78 year old man presented with constipation. Further workup revealed rectal narrowing, thickening, and hardening on digital rectal examination and sigmoidoscopy. His prostate specific antigen level was 409 ng/dL. CT and MRI imaging revealed wall thickening and a characteristic target sign, with biopsy revealing the submucosa and muscularis propria being invaded by prostate adenocarcinoma [2]. In 2021, a similar case was reported in which a 66 year old man presented with tenesmus, constipation, and fecal incontinence and a prostate specific antigen level of 180.6. Digital rectal exam and sigmoidoscopy, similarly, revealed narrowing and hardening. CT and MRI imaging revealed a target sign appearance of the rectum. Biopsy of the rectal walls ultimately revealed prostate adenocarcinoma [7].
Importantly, our case and the other two reported cases had similar presentations, which may help in identifying future patients with similar disease. All patients were in the 6-7th decade of life, presented with abnormal bowel movements, narrowing and hardening of the rectum on physical examination, and a characteristic target sign on CT/MRI imaging of the prostate. Furthermore, none of these patients presented with bone metastasis. Metastatic prostate cancer typically does not typically present with complaints of gastrointestinal upset or abnormal bowel movements, as Denonvillier’s fascia inhibits posterior infiltration [7]. An erroneous assumption to treat this linitis plastica and metastatic prostate cancer as if its etiology were of gastrointestinal origin would have deleterious consequences from the pursuit of unnecessary treatments and diagnostic workup.
This case highlights the importance of routine prostate cancer screening in all patients. A progressive decline in prostate cancer screening with prostate specific antigen levels and digital rectal examinations has been occurring since the United States Prevention Task Force recommended against it in 2012. Prostate cancer incidence has increased following these recommendations, including more aggressive disease at time of presentation [8]. Though secondary LP or malignancy of the rectum from PC is a rare phenomenon, it is possible that the increasing frequency of pelvic MRI imaging to monitor and diagnose PC [9,10], combined with a progressive decline in prostate cancer screening resulting in more aggressive prostate cancer presentations [8], could result in increased discovery of linitis plastica of the rectum secondary to prostate cancer. Additionally, this case highlights the need for verifying other abnormalities while working up patients for prostate cancer prior to beginning treatment. Interpreting these rectal changes as separate from the prostate cancer could have been detrimental due to vast differences in treatment and prognosis of metastatic versus localized prostate cancer.
Conclusion
Prostate cancer metastasis to the rectum is a rare phenomenon, and, in even rarer cases, may present as rectal linitis plastica. In the event that linitis plastica of the rectum is identified, prostate cancer should be in the differential diagnosis. Stereotypical findings may include a target-sign on rectal CT/MRI imaging, rectal thickening and narrowing, and changes in bowel movements. Increased imaging of the prostate and rectum, in addition to decreased prostate cancer screening resulting in more advanced disease presentation, may result in increased finding of linitis plastica of the rectum.
Key messages
● Linitis plastica of the rectum is a rare phenomenon, and, even more rarely, may occur secondary to prostate cancer metastasis.
● Linitis plastica of the rectum involves narrowing, hardening, and thickening of the rectal tissue.
● Computed tomography or magnetic resonance imaging of linitis plastica of the rectum reveals a target sign appearnce
● Prostate cancer metastasis to the rectum may result in linitis plastica of the rectum and produce findings of altered bowel habits and elevated prostate specific antigen levels.
● Linitis plastica of the rectum secondary to prostate cancer metastasis highlights the need for routine prostate cancer screening with digital rectal examination and prostate specific antigen levels
References
- Rubesin SE. Gallery of double-contrast terminology. Gastroenterol Clin North Am. 1995; 24: 259–288.
- You JH, Song JS, Jang KY, et al. Computed tomography and magnetic resonance imaging findings of metastatic rectal linitis plastica from prostate cancer: A case report and review of literature. World J Clin Cases. 2018; 6: 554–558.
- Mastoraki A, Papanikolaou IS, Sakorafas G, et al. Facing the challenge of managing linitis plastica--review of the literature. Hepatogastroenterology. 2009; 56: 1773–1778.
- Katon RM, Brendler SJ, Ireland K. Gastric linitis plastica with metastases to the colon: a mimic of Crohn’s disease. J Clin Gastroenterol. 1989; 11: 555–560.
- Balthazar EJ, Rosenberg HD, Davidian MM. Primary and metastatic scirrrhous carcinoma of the rectum. AJR Am J Roentgenol. 1979; 132: 711–715.
- Bhutani MS. EUS and EUS-guided fine-needle aspiration for the diagnosis of rectal linitis plastica secondary to prostate carcinoma. Gastrointest Endosc. 1999; 50: 117–119.
- Khor V, Khairul-Asri MG, Fahmy O, et al. Linitis plastica of the rectum secondary to metastatic prostate cancer: A case report of a rare presentation and literature review. Urol Ann. 2021; 13: 442–445.
- Shah N, Ioffe V. A Trend Toward Aggressive Prostate Cancer. Rev Urol. 2020; 22: 102–109.
- Kang SK, Mali RD, Prabhu V, et al. Active Surveillance Strategies for Low-Grade Prostate Cancer: Comparative Benefits and Cost-effectiveness. Radiology. 2021; 301: E380.
- Eklund M, Jäderling F, Discacciati A, et al. MRI-Targeted or Standard Biopsy in Prostate Cancer Screening. N Engl J Med. 2021; 385: 908–920.