
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Radiographic presentation of a multi-compartmental atypical giant lipoma of the lower extremity
Niel Patel*; Rohini Krishnan; Nitin Desai
Saint Louis University School of Medicine, USA.
*Corresponding Author : Niel Patel, BS
Saint Louis University School of Medicine, 1402 South Grand Boulevard, Saint Louis, MO, 63104, USA.
Email: niel.patel@health.slu.edu
Received : Sep 20, 2022
Accepted : Oct 20, 2022
Published : Oct 27, 2022
Archived : www.jcimcr.org
Copyright : © Patel N (2022).
Keywords: Atypical lipoma; Giant lipoma; Soft tissue mass; Multi-compartmental mass.
Citation: Patel N, Krishnan R, Desai N. Radiographic presentation of a multi-compartmental atypical giant lipoma of the lower extremity. J Clin Images Med Case Rep. 2022; 3(10): 2124.
Description
A 61-year-old female with no significant past medical history presented with painless progressive left lower extremity weakness and foot drop resulting in altered gait over the course of two years prior to seeking care. Examination revealed a hypertrophied left lower extremity, steppage gait, and 1 out of 5 strength with left ankle dorsiflexion. Initial x-ray of the affected ankle was unremarkable.
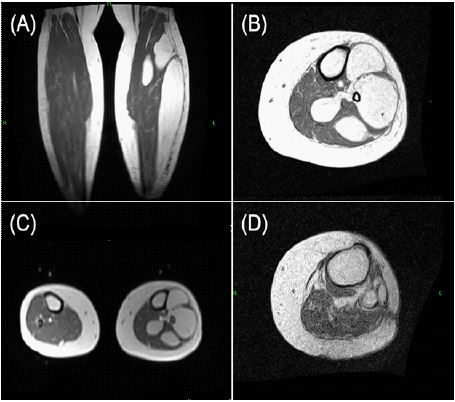
Further imaging of the affected extremity was performed via Magnetic Resonance Imaging (MRI), which revealed a large multi-compartmental fat containing mass occupying the anterior, lateral, and deep posterior compartments from the knee joint to just above the ankle joint (Figure 1A-C). Given the extensive spread of the mass and resulting gait alteration, surgical intervention was pursued with complete resection of the tumor. Postoperative pathology revealed the mass to be consistent with an atypical lipomatous tumor with generally mature adipocytes and occasional cytologic atypia. Following resection, the patient’s gait improved with physical therapy and repeat MRI after six months revealed normal postoperative changes without signs of tumor recurrence (Figure 1D).
Lipomas are the most common soft-tissue tumors and can be difficult to distinguish from rarer, malignant masses given their wide variety of presentations [1]. Lipomas can be characterized by their location, size, and underlying pathological features. In this image, we present a multi-compartmental giant lipoma extending from the knee to the ankle, with the term giant referring to lipomas greater than 10 cm in diameter or 1000 g in mass [2]. Tissue examination from this mass revealed an atypical pathology, which is the most common subtype of lipomas and commonly presents as a painless, slow-growing mass. Additional common subtypes include pleomorphic and myxoid lipomas, among many additional rarer cytologies including liposarcoma [3].
The differential diagnosis for lower extremity soft-tissue masses found on radiographic imaging is broad, adding to the challenges of identifying these tumors. Alternative diagnoses may include masses of muscle etiology (muscle hematomas, myositis ossificans, muscle strains), vascular etiology (hemangiomas, deep vein thrombosis), and other connective tissue structures (Baker’s cyst, fascial tear) [4].
Giant lipomas, especially those in multiple compartments of an extremity, can often cause symptoms due to compression of surrounding structures. In this case, the patient’s foot drop was presumed to be due to peroneal nerve compression and leg muscle atrophy. Despite their benign nature, giant lipomas also have a risk of malignant transformation to liposarcoma and warrant at minimum a biopsy for further evaluation [5]. For patients willing to undergo surgery, wide margin excision is a preferred treatment option [5]. However, with giant lipomas, the risk of recurrence remains, and patients should undergo continued surveillance following surgical intervention to assess for relapse [2,3]. Overall, when presented with a soft-tissue mass, clinicians should utilize radiographic and pathological findings to assist with identifying and categorizing lipomas, allowing for more informed treatment and surveillance strategies.
Declarations
Conflict of interest and disclosures: The authors deny any conflict of interest or financial disclosures. Patient consent for image publication was obtained prior to manuscript submission.
Funding: None
References
- Johnson CN, Ha AS, Chen E, Davidson D. Lipomatous Soft-tissue Tumors. J Am Acad Orthop Surg. 2018; 26: 779-788.
- Morales Morales CA, González Urquijo M, Morales Flores LF, Sánchez Gallegos MN, Rodarte Shade M, et al. Giant intramuscular thigh lipoma: A case report and review of literature. Int J Surg Case Rep. 2021; 82: 105885.
- Mascarenhas MRM, Mutti LA, Paiva JMG, Enokihara MMSES, Rosa IP, Enokihara MY, et al. Giant atypical lipoma. An Bras Dermatol. 2017; 92: 546-549.
- Constantinou M, Vicenzino B. Differential diagnosis of a soft tissue mass in the calf. J Orthop Sports Phys Ther. 2005; 35: 88-94.
- Al-Ani Z, Fernando M, Wilkinson V, Kotnis N. The management of deep-seated, lowgrade lipomatous lesions. Br J Radiol. 2018; 91: 20170725.