
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Advancing MRI in patients with cardiovascular
implantable electronic devices
Judson B Wing*; Jeff Madison; Tom McElderry; Kristin K Porter
The University of Alabama at Birmingham, AL 35294, USA.
*Corresponding Author : Judson B Wing
The University of Alabama at Birmingham, AL 35294, USA.
Phone: 205-913-3008;
Email: jbwing@uab.edu
Received : Sep 20, 2022
Accepted : Oct 21, 2022
Published : Oct 28, 2022
Archived : www.jcimcr.org
Copyright : © Wing JB (2022).
Abstract
Current medical practice separates Cardiovascular Implantable Electronic Devices (CIED) into two categories, conditional and nonconditional. Many physicians have been taught that patients with nonconditional CIEDs should never have MRI scans due to negative effects that the magnetic field could have on the device. Recent research has been published suggesting that MRI scans have little to no negative impact on these patients. The ability to do MRI scans on nonconditional CIED patients would lead to better patient care and outcomes along with helping to prevent misdiagnoses.
Keywords: MRI safety; MRI contraindications; Cardiac devices; Pacemaker; Defibrillator.
Citation:Wing JB, Madison J, McElderry T, Porter KK, et al. Advancing MRI in patients with cardiovascular implantable electronic devices. J Clin Images Med Case Rep. 2022; 3(10): 2127.
Introduction
In many cases once a patient receives a Cardiovascular Implantable Electronic Device (CIED) such as a pacemaker, Implantable Cardioverter-Defibrillator (ICD), Cardiac Resynchronization Therapy (CRT) pacemaker, or CRT defibrillator they will never receive Magnetic Resonance Imaging (MRI) again. Many physicians believe that these cardiac devices immediately exclude a patient from receiving an MRI due to the possibility of severe adverse effects. Recent publications have concluded that in many cases MRIs can be performed safely, and they can provide benefit in overall patient care. Further research and establishing better guidelines as to when the clinical benefit of MRI outweighs adverse effect risk in CIED patients would improve overall patient outcomes and provide great clinical utility. Additionally, MRI scans could help prevent a misdiagnosis much like the case discussed below.
Case presentation
Mr. X is a 63-year-old male with a past medical history ofchronic obstructive pulmonary disease, coronary artery disease, rheumatoid arthritis and possible heart failure with prior ICD placement, who presented for evaluation of brain mass lesions for which Neurosurgery was consulted. The patient’s family was present at the bedside and provided history as well as records from his prior admission. They report that the patient had developed several days of severe headaches. He was evaluated by his primary care physician, and a CT scan of the head demonstrated multiple brain mass lesions. He was then admitted to the Neurosurgical ICU that same day. He was immediately evaluated by several doctors, and as part of the workup for his lesions he underwent CT chest, abdomen, and pelvis, which demonstrated lung nodules. His medical records show that three attempts were made to obtain tissue diagnosis by Cardiothoracic and by Interventional Radiology. One of the tissue samples came back as non-diagnostic, while the other two attempts were unsuccessful. The patient was then seen by Hematology & Oncology; they believed that the lung nodules were bronchogenic carcinoma. The plan for the patient was to discharge him home with dexamethasone and to schedule 10 sessions of whole brain radiation.
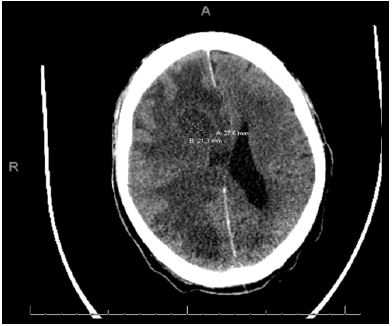
The patient was readmitted to hospital on midway through the next month. His family reported that during this admission he began to have generalized tonic-clonic seizure. Keppra was then prescribed, and he was discharged home on hospice. He was initially in his usual normal state of health, but a day later the patient developed a severe headache and increased somnolence that prompted him to go to the Emergency Department. On exam he was arousable but confused. A CT scan was then obtained. The scan showed peripheral enhancement in right frontal and occipitoparietal lesions surrounded by extensive vasogenic edema causing concern for intracranial metastatic disease. Intracranial abscesses were less likely.The CT also showed approximately 10mm of leftward midline shift with subfalcine herniation secondary to extensive mass effect from the right frontal lobe lesion.
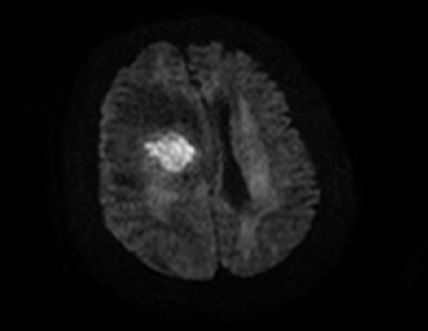
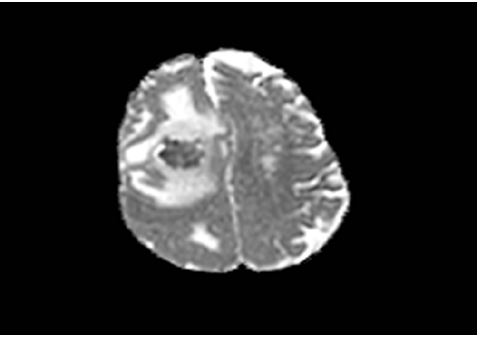
An MRI scan was then performed and showed that there were unchanged large right frontal and temporal occipital peripherally enhancing lesions. There was significant surrounding vasogenic edema and associated mass effect with partial effacement of the right lateral ventricle and 9 mm leftward midline shift. There was mild dilatation of the left lateral ventricle. The right frontal lobe lesion measured 2.8 x 3.1 x 3.4 cm and the temporal occipital lesion measured 3.4 x 2.3 x 2.4 cm. These lesions demonstrated an irregular T2 hypointense rim that involved both the lesions with irregularity and partial border thickening. The diffusion-weighted images demonstrated extensive central restricted diffusion. The source perfusion images also demonstrated a hypointense rim that surrounded these lesions. No other abnormal enhancing lesions were identified. There was no elevated rCBV on the provided perfusion images. The impression of this MRI was that this patient had two large peripheral-enhancing right frontal and temporal occipital lesions with extensive surrounding vasogenic edema and associated mass effect with 9 mm leftward midline shift. There was extensive diffusion restriction centrally within the lesions that was suspicious for abscesses. However, a heavily centrally necrotic neoplasm would be in the differential; further evaluation with SWI images could have been helpful in characterization.


The MRI directed the neurosurgery team to a substantially different therapy than the one that was developed on the patient’s previous admission. This therapy included a right craniotomy with resection of masses. The frozen section was consistent with abscesses. The gram stain came back positive for gram positive rods. A diagnosis of Nocardia was made. The patient was then treated with intravenous antibiotics. The patient went on to make a full neurologic recovery.
Discussion/ Conclusion
This case shows that MRI can serve as a diagnostic tool in cases where some people might believe that MRI is contraindicated. Using MRI in certain patients with cardiac devices could help prevent misdiagnosis and provide significant benefit in patient outcomes and management. 1 out of 50 Americans over the age of 75 years old will receive a CIED, and 1 out of 3 of these patients will need an MRI at some point in their life [4]. However, many hospitals across the country still have absolute contraindications to using MRI for patients with cardiac devices.
Recent studies suggest that MRI is safe in patient populations that we previously believed would have substantial negative results from the scans [1]. One study scanned 1000 patients with pacemakers and 500 patients with ICDs [3]. They found that MRI resulted in rare complications and no deaths [3]. Furthermore, a systematic review of 5625 patients with non-conditional CIEDs underwent 7196 MRI scans [5]. Their findings also resulted in no patient deaths or implantable-defibrillator shocks and an extremely low incidence of complications [5]. Further research into the risk of MRI in nonconditional device patientscould lead to revisions in protocols associated with conditional and nonconditional cardiac device MRI capabilities. The Canadian Cardiovascular Society, Canadian Society for Cardiovascular Magnetic Resonance, and Canadian Heart Rhythm Society have recommended that new standardized protocols be developed for scanning patients with CIEDs [2]. Development of these protocols could provide substantial patient benefit leading to better patient management. This research and education will require a significant commitment of time and resources but could vastly improve the quality of patient care.
Notes on patient consent
Due to potential risks to patients and to the high variabilityof the factors impacting this risk, a detailed evaluation of each request for an MRI should be performed. Upon completion of the evaluation, a risk/benefit analysis should be shared with the patient and/or the patient’s medical decision maker. The patient or medical decision maker should provide informed consent to the examination in writing before the examination. The radiologist should customize the MR scanning protocol to best accommodate the clinical goals for the examination, while limiting the patient’s exposure to the risks associated with it. The policy for MRI imaging at our institution for patients with CIED devices that are not conditional includes evaluation by the cardiac electrophysiology team and imaging with standard MRI protocols in Normal Scan mode. However, all patients who have implanted defibrillators require monitoring by Radiology nursing staff during MRI imaging (per manufacturer recommendations).
References
- Gupta SK, Ya’qoub L, Wimmer AP, Fisher S, Saeed IM. Safety and Clinical Impact of MRI in Patients with Non-MRI-conditional Cardiac Devices. Radiol Cardiothorac Imaging. 2020; 2: e200086.
- Primary Panel, Ian Paterson D, White JA, Butler CR, Connelly KA, Guerra PG, et al. 2021 Update on Safety of Magnetic Resonance Imaging: Joint Statement From Canadian Cardiovascular Society/Canadian Society for Cardiovascular Magnetic Resonance/Canadian Heart Rhythm Society. Can J Cardiol. 2021; 37: 835-847
- Russo RJ, Costa HS, Silva PD, Anderson JL, Arshad A, et al. Assessing the Risks Associated with MRI in Patients with a Pacemaker or Defibrillator. N Engl J Med. 2017; 376: 755-764.
- Deshpande S, Kella D, Padmanabhan D. MRI in patients with cardiac implantable electronic devices: A comprehensive review. Pacing Clin Electrophysiol. 2021; 44: 360-372.
- Munawar DA, Chan JEZ, Emami M, Kadhim K, Khokhar K, et al. Magnetic resonance imaging in non-conditional pacemakers and implantable cardioverter-defibrillators: A systematic review and meta-analysis. Europace. 2020; 22: 288-298.