
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Large pyomyoma after an urgent uterine
artery embolization (UAE)
Kirollos Bechay; Mariam Thomas*; Thomas Le; Ryan Beck; Kien Vuu; Brian Quinn
David Geffen School of Medicine at UCLA, Los Angeles, California, USA.
*Corresponding Author : Mariam Thomas, MD
Professor of Radiology at David Geffen School of Medicine at UCLA, Los Angeles, California, USA.
Vice Chair of Clinical Research, Olive View-UCLA Medical Center, Los Angeles, California, USA.
Email: thomasmariam0@gmail.com
Received : Sep 21, 2022
Accepted : Oct 21, 2022
Published : Oct 28, 2022
Archived : www.jcimcr.org
Copyright : © Thomas M (2022).
Citation: Bechay K, Thomas M, Le T, Beck R, Vuu K, et al. Large pyomyoma after an urgent uterine artery embolization (UAE). J Clin Images Med Case Rep. 2022; 3(10): 2128.
Introduction
Leiomyomas, or fibroids, are a common, benign tumor of the smooth muscle of the uterus, with a cumulative incidence of 70% in white women and 80% in black women by age 50 [1]. Suppurative leiomyoma, also referred to as pyomyoma, is a rare disorder of infarction with subsequent infection of a leiomyoma, which must be distinguished from other degenerative changes [2,3]. Incidence of the disease is unknown but previously estimated under 1% of operated fibroids [3], and there have been approximately 100 cases reported since 1945. The modes of infection are thought to be via direct extension from the uterine cavity, a lymphatic or a vascular route of bacterial seeding [3,4]. Pregnancy, the post-partum period, and uterine instrumentation, including dilatation and curettage (D&C) and C-section, are important risk factors for direct inoculation and account for the majority of pyomyoma cases that were reported [5,6]. Idiopathic pyomyomas also occur, such as in post-menopausal women; risk factors for ischemia, such as hypertension, diabetes, and atherosclerosis, increase the risk of pyomyoma [4,5]. Uterine Artery Embolization (UAE) is increasingly used as a non-invasive treatment for symptomatic fibroids and involves infarction of leiomyomas, which can rarely lead to pyomyoma [7,8]. We present a case of pyomyoma that developed after an urgent uterine artery embolization with a follow-up discussion of the relevant literature.
Case report
A 51-year-old G1P1 female was brought into the ED for heavy vaginal bleeding, paleness, and light headedness. Her medical history includes SLE and three thromboembolic strokes, for which she takes warfarin (5 mg daily). She also had abnormal uterine bleeding for 19 years, managed with leuprolide acetate, which was recently discontinued to assess for menopause. The patient had gone to the ED one week prior with similar symptoms but discharged as her hemoglobin was 13. At the time of admission, her hemoglobin had dropped to 7.2, requiring blood transfusion. Bleeding was temporized by vaginal packing and cervical foley balloon placement. The patient was started on doxycycline (100 mg) by the primary service in the setting of cervical instrumentation, and IR wasurgently consulted for a uterine artery embolization.
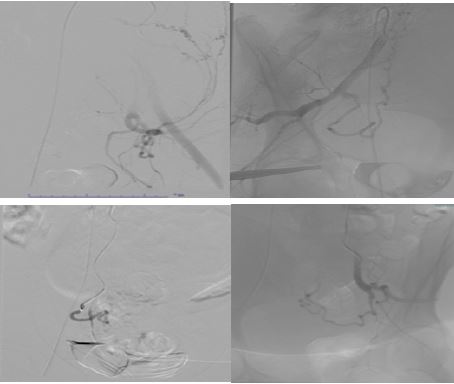
The patient was consented and taken to the fluoroscopy suite for the UAE. Micropuncture access was achieved through the right common femoral artery, and a 5-French pigtail flush catheter was used to perform a pelvic angiogram. Hypogastric catheterization was achieved with a 5-French VS1 catheter. The uterine arteries were then selected sequentially with a Progreat 2.8 microcatheter and guidewire. Embolization was performed with 600 micron and 800 micronpolyethylene glycol microspheres (Hydropearls), followed by gel foam pledglets until stasis was achieved. The patient tolerated the procedure well and without apparent complications. She was transferred to the medicine department, receiving another blood transfusion for down-trending hemoglobin, and was discharged after four days.
The patient had a one-week follow-up visit at the gynecology clinic, where her INR was elevated to 5.98, and she was instructed to go to the ED. Although the patient reported decreased bleeding, she reports the color is darker and a new, foul smell from her vagina for two days. She also reported lethargy, decreased appetite, and constipation. She was nontender on exam and was wearing a foul-smelling pad mildly soaked with a dark brown discharge. Hemoglobin was decreased to 7, while she was discharged at 8.2. Labs were notable for leukocytosis (up to 24.8 cells/uL), anemia, supratherapeutic INR (up to 8.5), AKI, transaminitis, elevated fibrinogen, and CRP. Coumadin was held, and INR decreased to 3. She became febrile to 38.4 degrees but was hemodynamically stable. CT of the abdomen and pelvis demonstrated a markedly distended uterus with a central area of necrosis and numerous foci of gas. The uterus measured 22.3 x 13.8 x 17.0 cm with a necrotic, gaseous core measuring 16.2 x 10 x 12.2 cm. She was diagnosed with sepsis due to pyomyoma, most likely as a complication from her UAE.
IV antibiotics were initiated (cefepime, doxycycline, metronidazole), and anticoagulation was reversed with Vitamin K and two units of fresh frozen plasma. INR was measured at 1.8. Total Abdominal Hysterectomy (TAH) was performed two days after admission, with the removal of most of the cervix (~6 cm). A large and irregular uterus was observed, but without turbid material in the abdomen. Omental and bladder adhesions to the uterus were noted and were carefully dissected. The abdominal cavity was then copiously irrigated with warm saline. The removed uterus and cervix were then sent for pathological assessment. There was an estimated 350 cc of blood loss, and the surgery was well-tolerated. Purulent discharge from the pyomyoma was sent for culture and grew Group B streptococcal species and Proteus mirabilis. On postoperative day two, the patient had a seizure which was controlled with levetiracetam. On postoperative day four, the patient developed a superficial wound cellulitis which was treated with a course of antibiotics. There were no other complications; the anemia, acute kidney injury, and transaminitis all improved, and the patient was discharged on postoperative day 11, with closely scheduled follow-ups. On pathological assessment, the enlarged and distorted uterus weighed 2140 grams, with protruding and necrotic myoma, the largest measuring 13 cm, 6 cm and 4 cm. There were many foreign body granulomas, likely the material from the embolization.


Discussion
Uterine Artery Embolization (UAE) is a non-invasive, endovascular procedure with the goal of causing ischemia and necrosis of fibroids in order to reduce their size. For approximately 30 years, UAE has been increasingly utilized for symptomatic leiomyomas, with an average reduction of uterine size by 48%, bulk symptom reduction of 77% after 6 months, and control of menorrhagia at 85% after 6 months [9,10]. Multiple large studies have demonstrated the safety and efficacy of UAE, with lower complication rates than the surgical alternatives [10]. Due to the induced infarction of the fibroid, pyomyoma is a rare and unique complication of UAE which must be considered by clinicians.
At least 13 cases of pyomyoma secondary to UAE have been reported since 1945, ranging in patients aged 28 to 65 years and all were greater than 7 cm [5,11-14]. It is thought that the UAE predisposes the development of a pyomyoma by deliberately infracting the fibroid, increasing the likelihood of infection. Vaginal procedures, such as the vaginal packing and intracervical catheterization in the present case, may further provide a nidus for infection. The 13 cm myoma in the present case is the largest pyomyoma secondary to UAE reported, to the best of our knowledge. Most patients presented with pain, fever and leukocytosis, as did our patient. Our patient also presented with malodorous vaginal discharge, which was noted only in two other cases [11]. Neither the type nor amount of embolic material has been suggested as a risk factor for pyomyoma development [15]. Time to the presentation from UAE to pyomyoma ranged from 6 to 56 days, placing our patient’s diagnosis at postoperative day 7 as a relatively acute complication. The CT findings of an enlarged uterus, necrosis, and foci of gas in the current case were typical of those reported pyomyomas after UAE. Once pyomyoma is diagnosed, hysterectomy with an exploratory laparotomy is the preferred treatment; abscesses, ulcers and adhesions involving the fallopian tubes, ovaries, appendix, bladder and omentum have been reported in these cases [11]. The omental and bladder adhesions noted in the present case were not unique in that sense. 8 of the 13 cases underwent a hysterectomy, while the remaining underwent uterine-conserving transcervical hysteroscopic treatment or a conservative laparoscopic approach [11,12,16]. All patients recovered well and were discharged typically within a week. The discharge of 11 days after hysterectomy in the current case was thus lengthier than average, likely due to the patient’s complications of seizure and superficial cellulitis.
The diagnosis of pyomyomas may be difficult due to their rarity and often insidious onset of presentation. The triad of fibroids, sepsis, and an unidentified source of infection should raise suspicion for pyomyoma [2]. Other common presenting signs include fever, abdominal pain, and vaginal discharge or bleeding. Leukocytosis is a common finding, but bacteremia is not. In a literature review of 70 cases since 1945, 58 demonstrated leukocytosis >11,000 cells/uL, while blood cultures were positive in only 21 of 63 cases that reported blood cultures [6]. Cultures from the pyomyoma, however, are often positive and an organism was identified in 54 of 61 cases, with the most common being E. coli, Staphylococcal species, Streptococcal species, and Enterococcal species [6]. Proteus mirabilis, which grew in cultures from the present case, is a rare cause of pyomyoma which was reported only twice before [17,18].
Several imaging modalities can aid the diagnosis of pyomypyomyoma, including ultrasonography, Computer Tomography (CT) scan and MRI [4,18-21]. Transvaginal ultrasound may reveal an enlarged uterus with a heterogenous, echogenic mass and acoustic shadowing due to gas. CT-scan often reveals a heterogenous mass with cystic components, necrotic debris, and an enhancing peripheral rim. Gas is also a common finding, although this may be a normal finding after uterine artery embolization [7,8,12,15]. Rupture of a pyomyoma may additionally present with intraperitoneal free air and discontinuity of the myoma wall [18]. On MR examination, the cystic components of pyomyoma appear hypointense on T1 and a fibrous capsule may be appreciated [19]. Furthermore, Diffusion Weighted Imaging (DWI) excels at localizing abscesses and may play a role in guiding biopsy to confirm the diagnosis before surgery [20].
An important differential of abdominal pain, leukocytosis and fever after UAE is Post-Embolization Syndrome (PES). A mild leukocytosis is found in 86% of patients after UAE, with clinically elevated levels in 21% of patients, an estimate of the incidence of PES [22]. Foul-smelling vaginal discharge, high-grade leukocytosis or presentation greater than a week after the procedure are all suspicious for an infectious process [8]. Symptomatic responsiveness to antibiotics should be another sign of an infectious process, as in pyomyoma.
Prior to 1945 and the introduction of intravenous antibiotics, mortality of pyomyoma was estimated between 33-70%, even with hysterectomy [3]. Since then, the prognosis has improved dramatically with an estimated mortality of 5.3%, and < 2% since 1990 [6]. In the four deaths since 1945, two received only antibiotics and one additionally received percutaneous drainage, as they were too ill to undergo surgery [6]. This highlights the standard of treatment, which is hysterectomy or myomectomy of the pyomyoma, in addition to IV antibiotics. Although hysterectomy is usually preferred, uterine preserving surgery with hysteroscopy has been successfulas well [11,12].
References
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM, et al. High cumulative incidence of uterine leiomyoma in black and white women: Ultrasound evidence. Am J Obstet Gynecol. 2003; 188: 100-107.
- Greenspoon JS, Ault M, James BA, Kaplan L. Pyomyoma associated with polymicrobial bacteremia and fatal septic shock: Case report and review of the literature. Obstet Gynecol Surv. 1990; 45: 563-569.
- Miller I. Suppurating Fibromyomas: Report of a Case with a Review of the Literature. Am J Obstet Gynecol. 1945; 50: 522-526.
- Karcaaltincaba M, Sudakoff GS. CT of a Ruptured Pyomyoma. Am J Roentgenol. 2003; 181: 1375-1377.
- Read S, Mullins J. Spontaneous Ruptured Pyomyoma in a Nulligravid Female: A Case Report and Review of the Literature. Case Rep Obstet Gynecol. 2018; 2018: 1-6.
- Azimi-ghomi O, Gradon J. Pyomyoma: Case Report and Comprehensive Literature Review of 75 Cases Since 1945; SM J Case Reports. 2017; 3.
- Kitamura Y, Ascher SM, Cooper C, et al. Imaging manifestations of complications associated with uterine artery embolization. Radiographics. 2005; 25: 119-133.
- Rezai S, Elmadjian M, Hastings A, et al. Pyomyoma Following Uterine Artery Embolization (UAE) – Dual Case Report and Review of Literature. Obstet Gynecol Int J. 2016; 4: 33-37.
- Hutchins FL, Worthington Kirsch R, Berkowitz RP. Selective uterine artery embolization as primary treatment for symptomatic leiomyomata uteri. J Am Assoc Gynecol Laparosc. 1999; 6: 279-284.
- Keung JJ, Spies JB, Caridi TM. Uterine artery embolization: A review of current concepts. Best Pract Res Clin Obstet Gynaecol. 2018; 46: 66-73.
- Yu Q, Gabriel G, Hoffman M, Sanampudi S, Jassim T, Raissi D, et al. Uterine-sparing management of pyomyoma after uterine fibroid embolization. Radiol Case Reports. 2019; 14: 1031-1035.
- Busshoff J, Thangarajah F, Morgenstern B. Uterus-preserving management of pyomyoma: Case report of a rare complication after uterine artery embolization. Case Reports Women’s Heal. 2022; 34: e00405.
- Ezzedine D, Ndubizu C, Kayani S, David A. Pyomyoma after uterine artery embolization: A case report. Case Reports Women’s Heal. 2020; 26: e00186.
- Song H, Seo JW, Shin W. Pyomyoma after Uterine Artery Embolization for Postpartum Hemorrhage Misdiagnosed as Uterine Necrosis. J Korean Soc Radiol. 2018; 78: 63.
- Obele CC, Dunham S, Bennett G, Pagan J, Sung LY, et al. A Case of Pyomyoma following Uterine Fibroid Embolization and a Review of the Literature. Case Rep Obstet Gynecol. 2016; 2016: 1-5.
- Pinto E, Trovão A, Leitão S, Pina C, Mak F kok, et al. Conservative Laparoscopic Approach to a Perforated Pyomyoma After Uterine Artery Embolization. J Minim Invasive Gynecol. 2012; 19: 775-779.
- Weiss G, Shenker L, Gorstein F. Suppurating myoma with spontaneous drainage through abdominal wall. N Y State J Med. 1976; 76: 572-573.
- Yeat SK, Chong KM, Pan HS, Cheng WC, Hwang JL, Lee CC, et al. Impending sepsis due to a ruptured pyomyoma with purulent peritonitis: A case report and literature review. Taiwan J Obstet Gynecol. 2005; 44: 75-79.
- Ono H, Kanematsu M, Kato H, et al. MR imaging findings of uterine pyomyoma: Radiologic-pathologic correlation. Abdom Imaging. 2014; 39: 797-801.
- Peris H, del Riego J, Criado E, et al. Value of diffusion-weighted magnetic resonance imaging in the diagnosis of pyomyoma. Radiol Case Reports. 2022; 17: 137-141.
- Abulafia O, Shah T, Salame G, et al. Sonographic Features Associated With Post-Uterine Artery Embolization Pyomyoma Abbreviations CT, computed tomography Case Report. J Ultrasound Med. Published online. 2010: 839-842.
- Ganguli S, Faintuch S, Salazar GM, Rabkin DJ, et al. Postembolization Syndrome: Changes in White Blood Cell Counts Immediately after Uterine Artery Embolization. J Vasc Interv Radiol. 2008; 19: 443-445.