
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Quetiapine augmentation of cognitive processing therapy
in veterans with posttraumatic stress disorder. Design and methodology of a pilot study
Muhammad R Baig1,2,3*; Jennifer L Wilson1,2; Robert D Beck1,2; Jennifer A Lemmer1,2; Adeel Meraj1; Anna Hernandez1; Eric C Meyer4; Jim Mintz3,5; Alan L Peterson1,3,6; John D Roache3,7
1Mental Health, South Texas Veterans Healthcare System, San Antonio, TX, 78229, USA.
2Polytrauma Rehabilitation Center, South Texas Veterans Healthcare System, San Antonio, TX, USA.
3Department of Psychiatry and Behavioral Sciences, University of Texas Health Science Center at San Antonio, San Antonio, TX, USA.
4Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA, USA.
5Department of Epidemiology and Biostatistics, University of Texas Health Science Center at San Antonio, San Antonio, Texas, USA.
6Department of Psychology, University of Texas at San Antonio, San Antonio, TX, USA.
7Department of Pharmacology, University of Texas Health Science Center at San Antonio, San Antonio, TX, USA.
*Corresponding Author : Muhammad Rais Baig
Mental Health, South Texas Veterans Healthcare System, 116 A, 7400 Merton Minter Blvd, San Antonio, TX, USA.
Tel: 210-617-5300 Extension: 18244;
Email: Muhammad.baig@va.gov
ORCID: 0000-0003-4589-7707
Received : Sep 21, 2022
Accepted : Oct 25, 2022
Published : Nov 01, 2022
Archived : www.jcimcr.org
Copyright : © Baig MR (2022).
Abstract
Background: The limited efficacy of first-line treatment of Posttraumatic Stress Disorder (PTSD) with selective serotonergic reuptake inhibitors commonly leads to the use of multiple medications that still fail to achieve symptomatic remission. VA/DOD guidelines identify trauma-focused psychotherapies as the evidence-based treatment for PTSD, but overall effectiveness is limited by reduced levels of patient engagement. Cognitive Processing Therapy (CPT) is the most widely-used trauma-focused therapy in the VA system for Veterans with PTSD. Our previous results based on a case series suggested that quetiapine mono therapy, but not risperidone or valproate, could increase engagement in CPT, thereby improving clinical outcomes through direct medication effects and indirectly through greater engagement in CPT.
Methods & results: We report the study protocol of a pilot study. This randomized, double blind placebo-controlled study was designed to evaluate the feasibility, safety, and preliminary efficacy of completing a randomized trial of quetiapine vs. placebo as an adjunct to promote patient engagement in CPT treatment for PTSD.
Conclusions: We expect that the success of this ongoing study should provide us with the preliminary data necessary to design a full-scale randomized trial.
Trial registration: NCT04280965
Keywords: Quetiapine; Cognitive processing therapy; Posttraumatic stress disorder; Veterans.
Abbreviations: AEs: Adverse Events; AUDIT: Alcohol Use Disorders Identification Test; CAPS-5: Clinician Administered PTSD Scale for DSM-5; CPT: Cognitive Processing Therapy; DSM-5: Diagnosis and Statistical Manual of Mental Disorder, Fifth Edition; DUDIT: Drug Use Disorders Identification Test; ECG: Electrocardiogram; GABA: Gamma-aminobutyric Acid; GAD-7: Generalized Anxiety Disorder-7; ISI: Insomnia Sleep Index; PCL-5: PTSD checklist for DSM-5; PHQ-9: Patient Health Questionnaire-9; PTGI: Post Traumatic Growth Inventory; PTSD: Posttraumatic Stress Disorder; SSRI: Selective Serotonin Reuptake Inhibitor; STVHCS: South Texas Veterans Health Care System; TFT: Trauma-focused Therapy; TSQM-9: Treatment Satisfaction Questionnaire for Medication-9; QTc: Corrected QT interval; UTHSCSA: University of Texas Health Science Center at San Antonio; WHODAS 2.0: World Health Organization Disability Assessment Scale; WHOQOL-BREFF: World Health Organization Quality of Life-BREF.
Citation: Baig MR, Wilson JL, Beck RD, Lemmer JA, Meraj A, et al. Quetiapine augmentation of cognitive processing therapy in veterans with posttraumatic stress disorder. Design and methodology of a pilot study. J Clin Images Med Case Rep. 2022; 3(11): 2130.
Background
The only two medications approved by the U.S. Food and Drug Administration for the treatment of Posttraumatic Stress Disorder (PTSD), sertraline and paroxetine, are both Selective Serotonin Reuptake Inhibitors (SSRI’s) [1]. However, an Institute of Medicine review concluded that SSRI efficacy is limited, particularly for males suffering from PTSD due to military combat exposure [2,3]. Whereas, VA/DOD guidelines identify trauma-focused psychotherapies as having the strongest evidence for treating PTSD [4].
Cognitive Processing Therapy (CPT) has gained wide-acceptance as a standard of care PTSD treatment in VA and DoD practice settings [5]. However, patients and therapists alike may have concerns with CPT regarding its potential to evoke negatively evaluated trauma-related emotions. These concerns may contribute to hesitance to engage in CPT treatment in the first place or to continue in treatment long enough to achieve complete remission or otherwise attain symptom reductions [6-8]. Our preliminary findings of mental health services within a rehabilitation program suggest that even with a robust integrated mental healthcare program, almost half of the Veterans reject CPT outright, and half of those who do initiate drop-out [9]. Therefore, while CPT has a large effect size for therapy-compliant patients, there is considerable room for improvement in the areas of patient engagement and achieving greater overall remission rates [10,11].
In studies seeking to identify new psychopharmacologic treatments for PTSD, neither adjunctive use of risperidone [12] nor valproate monotherapy [13] were superior to placebo to lessen PTSD symptoms. In contrast, a small, placebo-controlled trial of quetiapine monotherapy, an atypical antipsychotic with a broad spectrum of actions at several receptors, did report significantly reduced arousal and reexperiencing of PTSD symptoms in veterans [14,15]. These actions make it well suited to repurpose an already approved drug for a randomized trial approach to evaluate its use as an adjunct to usual care in the VA System. Quetiapine’s ability to reduce irritability, anxiety, and improve sleep without impairing sleep architecture is a distinct benefit over other options and theoretically may benefit patients undergoing CPT [16-19]. Unfortunately, local VA treatment guidelines specify that off-label use of atypical antipsychotics such as quetiapine is permitted only after at least two failed trials of SSRIs.
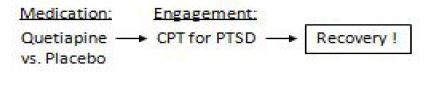
Recent considerations for the design of clinical trials focused on PTSD treatment have suggested that we identify target systems involved in fear extinction and explore medications that enhance the targeted approach of trauma-focused therapies [20-28]. In a search for psychosedative medications that may enhance engagement in CPT, we reported case series data showing that quetiapine monotherapy, but not risperidone or valproate, increased engagement in therapy for 86% of 21 veterans, and 50% of those (i.e., 43% overall) achieved remission of PTSD [29]. Consistent with this, we propose that quetiapine may be an efficacious medication treatment for enhancing patient engagement in trauma-focused therapy and thereby improving recovery outcomes for veterans with PTSD who are offered CPT as a standard of care therapy (Figure 1). Positive efficacy results in a full-scale trial should inform new VA guidelines for clinical practice by showing that quetiapine-related improvements in patient engagement may be the most effective approach to assure that VA resources achieve the best possible outcome for veterans. In the current report, we describe the study protocol of an ongoing, randomized, double-blind, placebo-controlled pilot study examining the effects of quetiapine vs. placebo as an adjunct on engagement in CPT treatment in veterans with PTSD.
Research objectives and hypotheses
We seek to conduct a pilot trial evaluating patient safety and feasibility of administering quetiapine to veterans with PTSD with the expectation that it will enhance engagement of veterans in trauma-focused therapy with CPT. Our study design is a randomized, placebo-controlled, double-blind comparison of quetiapine versus placebo administered as an adjunct to a 13-week treatment period involving CPT for PTSD. The aims of the study are to evaluate the effect of quetiapine on engagement in CPT treatment, insomnia, and anxiety, recovery and putative mechanisms by which it may facilitate recovery, and to test the conceptual model for promotion of recovery in Veterans receiving CPT treatment for PTSD. There are three main hypotheses that pertain to changes in outcomes of interest during the treatment phase (weeks 1-14). Hypothesis 1 proposes that participants who receive quetiapine, as compared to placebo, will evidence significantly greater engagement in CPT treatment and improvement in insomnia and anxiety. Hypothesis 2 centers on the rehabilitation outcomes and proposes that participants who receive quetiapine, as compared to placebo, will evidence enhanced recovery at week 14, measured as a latent variable comprised of functional disability, Quality of Life, and PTSD symptom severity. Hypothesis 3 is that quetiapine will promote recovery through its effects on treatment engagement, insomnia, and anxiety.
Methods & results
All study procedures are approved and monitored by the University of Texas Health Science Center at San Antonio Institutional Review Board and South Texas Veterans Health Care System (STVHCS) Research and Development Committee. In addition, all study participants complete a written informed consent prior to any study procedure and are eligible to receive other standard of care treatments within their VA.
Study population
We plan to randomize a sample of 20 male and female veterans, between ages of 18-65, for the double-blind treatment phase (10 per treatment group), who meet study inclusion/exclusion criteria outlined below.
Inclusion criteria
1. All treatment seeking adult male or female veterans between the ages 18-65 years.
2. Meet PTSD diagnosis having a Clinician Administered PTSD Scale for DSM-5 (CAPS-5) of 25 or greater at screening.
3. Participants requiring other medication for general medical conditions such as antihypertensive medications for hypertension, anti-thyroid medications for hyperthyroidism, and/or anti-epileptic medications, divalproex, levetiracetam, or carbamazepine for seizure disorder or post traumatic headaches may be included if treatment has been stable for at least 4 weeks prior to screening.
4. Able to read and write English.
Exclusion criteria
1. Pregnant or lactating women and those of child-bearing potential not using a reliable method of contraception;
2. Meeting DSM-5 criteria for schizophrenia, bipolar disorder, or schizoaffective disorder;
3. Any history indicating major neurocognitive disorder (dementia) or intellectual disability as determined by study physician;
4. Currently taking any of the exclusionary medications including typical or atypical antipsychotic medication;trazodone, mirtazapine, prazosin, benzodiazepines, and/or non-benzodiazepine hypnotics;
5. Known intolerance to quetiapine;
6. History of clinically unstable heart, lung, liver, renal or endocrinological condition, diabetes mellitus, and/or seizure disorder;
7. Substance use disorder severe enough to require medical detoxification or inpatient hospitalization in the past month;
8. Current, ongoing serious suicidal or homicidal risk as assessed by study physician;
9. Current or known history of cardiac arrhythmia or QTc interval ≥475 milliseconds;
10. Currently engaged in other psychotherapeutic treatment;
11. Individuals with lack of stable contact information (including lack of a telephone number).
12. Individuals under criminal investigation or pending legal charges with potential incarceration.
Notes: Concomitant chronic daily benzodiazepine and/or non-benzodiazepine hypnotics may impair progress with CPT. An individual taking any of these medications for the sole purpose of improving sleep that elects to undergo an adequate wash-out period of at least 5 half-lives under the care of the individual’s clinical provider, wouldn’t be excluded by this criterion.
Study site
The treatment study will be conducted within the STVHCS in San Antonio. Participants will be recruited by clinical referrals from mental health staff.
Study procedures
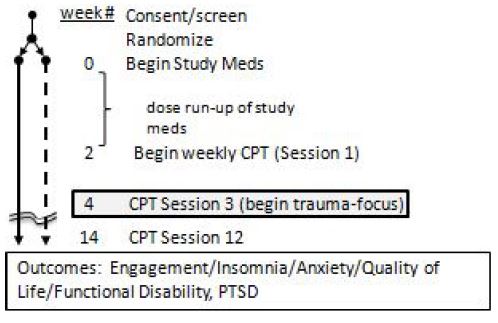
This is a double-blind, placebo-controlled 14- week pilot study in which participants will be randomized to receive quetiapine (n =10) or placebo (n = 10). Prescreening will be accomplished by review of patient’s medical record, speaking to the patient’s treating clinician, and interview by the study coordinator in person (if possible) or by telephone to eliminate any obviously ineligible participants and determine the likelihood of eligibility. During chart review, lab data from clinical care will also inform study coordinator regarding an individual’s likely eligibility. After prescreening, potentially eligible individuals will be scheduled for written informed consent and a formal screening visit. Participants who pass the eligibility screening will be scheduled for randomization as soon as possible after screening. Sequentially eligible participants will be assigned to receive either 1) placebo or 2) quetiapine by the Research Pharmacist to a randomized sequence established prior to the study. The participants, study physician, clinical prescribers and psychologists, and study coordinator will remain blinded to treatment assignment. After randomization, all patients will begin a 2-week stabilization period before beginning CPT. During this time, patients will receive a flexible dose regimen based upon tolerability and clinical response to maximize engagement in rehabilitation treatment by initiating quetiapine or placebo treatment 2 weeks before starting CPT treatment. Flexible dosing will begin with 25 mg at bedtime and titration up to 200 mg daily if needed. Matching placebo will permit apparent dose adjustments to be accomplished by adjusting the number of tablets prescribed. Medication treatment will be maintained throughout 14-week study period including the 12 session CPT. Doses will be adjusted as clinically indicated (Figure 2).
Assessments
A full list of study measures and assessment procedures is outlined in Table 1.
Table 1: Schedule of visits/assessments
| V0 | V1 | TEL | V2 | V3 | V4 | V5 | V6 | V7 | V8 | V9 | V10 | V11 | V12 | V13 | TEL | TEL | TEL | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Assessments | Scr | WK | WK | WK | WK | WK | WK | WK | WK | WK | WK | WK | WK | WK | MO | MO | MO | ||
| 1 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 3 | 6 | 12 | ||||
| Informed Consent | X | ||||||||||||||||||
| Med History & Physical Exam | X | ||||||||||||||||||
| LEC-5 | X | ||||||||||||||||||
| CAPS-5 (by phone) | X | X | |||||||||||||||||
| NSI | X | X | |||||||||||||||||
| PHQ-9 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| AUDIT | X | X | |||||||||||||||||
| DUDIT | X | X | |||||||||||||||||
| Engagement | X | X | X | X | X | X | X | X | X | X | X | X | |||||||
| ISI | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| GAD-7 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| PCL-5 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| WHOQOL BREF | X | X | X | X | X | X | X | ||||||||||||
| WHODAS 2.0 | X | X | X | X | X | X | X | ||||||||||||
| TSQM-9 | X | X | X | X | X | X | X | ||||||||||||
| Blind Integrity | X | ||||||||||||||||||
| Medication Diary | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||
| Medication Dosing | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||||
| Adverse Effects | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||||
| Psychotherapy | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | |||||||
| Vital Signs | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |||||
| Labs | X | X | X | ||||||||||||||||
| ECG | X | X | X |
Abbreviations: CAPS-5: Clinician-Administered PTSD Scale for DSM-5; PCL-5: PTSD Checklist for DSM-5; ISI, Insomnia Sleep Index; GAD-7: Generalized Anxiety Disorder-7; WHODAS 2.0: World Health Organization Disability Assessment Schedule 2.0; WHOQOL-BREF: World Health Organization Quality of Life-BREF; PHQ-9, Patient Health Questionnaire; PTGI: Post Traumatic Growth Inventory; AUDIT: Alcohol Use Disorders Identification Test; DUDIT: Drug Use Disorders Identification Test; TSQM-9: Treatment Satisfaction Questionnaire for Medication-9; ECG: 12-Lead Electrocardiogram.
Notes: Shown are procedures completed at visits (V#) / weeks (WK) of study. Screening (Scr) occurs at V0 and medication initiation occurs at V1.
Primary outcome measures
The primary outcome measures for this study are: (1) trial feasibility, (2) engagement in CPT, anxiety, and insomnia, and (3) recovery.
Feasibility
We will collect information on number of potentially eligible veterans approached, the number screened, and the number randomized. This information will allow us to determine patient acceptability, and the logistic feasibility of recruiting participants into a full-scale, randomized, double-blind, placebo-controlled trial that requires antipsychotic medication versus placebo in combination with CPT.
Measures of engagement in CPT treatment
After 2 weeks of quetiapine or placebo dosing, participants will begin CPT. CPT lasts for 12 weekly sessions but trauma exposure doesn’t begin until session #3 (Visit 4) when participant is asked to write a full account of the most traumatic event with sensory details. A significant number of PTSD patients terminate treatment prior to session #4, in which the completed account is reviewed and read aloud by the patient, which suggests strongly that the emotional difficulty of directly engaging with trauma content is a substantial barrier to treatment engagement. We have established two measures of engagement in CPT treatment. The first is continuing CPT treatment at least until session # 4 (i.e., when trauma account is due). The second measure is the participant’s self-report on engagement in therapy measured by emotional engagement graded on a scale from 0 (not very engaged) to 10 (fully engaged) at every visit by the participant; a score of 7 or higher is the desired response and self-reported completion of homework. We also will record the number of sessions of CPT completed by the participants. Non-compliance with the CPT treatment reported by the therapist will also be documented. The completions status will be confirmed after discussion with the therapist and number of sessions of CPT completed by the participants will also be recorded.
Anxiety
Change in anxiety will be assessed using a well validated and quick and easy to administer self-administered, the Generalized Anxiety Disorder 7 item (GAD-7) scale [30].
Insomnia
Change in insomnia will be assessed using the Insomnia Severity Index (ISI) [31]. The ISI is short (7 items), easy to complete, and it has been used in evaluating insomnia in veteran populations [32]. We considered several alternative primary outcome measures for this study and dismissed them for the following reasonse: Polysomnography is too burdensome and costly. Sleep diaries are equally valid and sensitive, but they are more burdensome. The ISI has been validated against both polysomnography and sleep diary assessments in clinical trials [33]. Lastly, although the Pittsburgh Sleep Quality Index is a popular measure of overall sleep disturbances however ISI is preferred for insomnia [34].
PTSD symptom severity
PTSD Checklist for DSM-5 (PCL-5) is a 20-item validated self-report measure which is widely implemented throughout the VA clinics to screen individuals for PTSD, make a provisional PTSD diagnosis, and monitor symptom change during and after treatment [35]. A PCL-5 score of 34 is considered an optimal cutoff level for the diagnosis of PTSD [36]. Evidence has suggested that 10 point change in PCL score represents reliable and clinically significant change [35].
Quality of life
The World Health Organization Quality of Life (WHOQOL) BREF is a 26 item self-report questionnaire to assess functioning and quality of life from the patient’s perspective over the past 2-week period [37]. It is a measure of conceptual domains of quality of life: Material and physical well-being, relationships with other people, social, community and civic activities, personal development and fulfillment, independence, and recreation. It is a reliable and valid instrument utilized in physically and psychologically disabling conditions including PTSD.
Disability
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) is a 12 item self-report to measure functional disability over the past 30-day period [38]. It assesses 6 domains of functioning: cognition, mobility, self-care, getting along, life activities, and participation.
Secondary outcome measures
The secondary outcomes include: (1) The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) [39] will be used to establish PTSD diagnostic status at the screening and end of study (Visit 11). CAPS-5 is a gold standard diagnostic interview for PTSD, developed by National Center for PTSD. We will enroll participants who meet diagnostic criteria for PTSD and who have a CAPS-5 score of >25 and will repeat assessment at end of treatment to determine clinically significant change in the scores. PTSD diagnosis will be determined using the PTSD diagnosis algorithm recommended by the National Center of PTSD which requires at least moderate ratings (2 or more) on at least 1 B item (items #1-5), 1 C item (items #6-7), 2 D items (#8-14), and 2 E items (items #15-20) of the CAPS-5. (2) The Patient Health Questionnaire (PHQ)-9 will monitor for change in depressive symptoms, suicidality by the item # 9, and homicidality by an added question [40]. (3) The Post Traumatic Growth Inventory (PTGI) will measure change in cognition about positive outcomes [41]. (4) Substance use will be assessed by Alcohol Use Disorders Identification Test (AUDIT) [42], and Drug Use Disorders Identification Test (DUDIT) [43] and treatment satisfaction by the Treatment Satisfaction Questionnaire for Medication-9 (TSQM-9) [44].
Quetiapine has risks and side effects. Quetiapine may cause sedation and extra-pyramidal symptoms. The medications in the atypical antipsychotic class prescribed at high dose, for longer duration of treatment, in severely mentally ill individuals increase the risk for diabetes and heart diseases by causing metabolic dysregulation. We will thoroughly screen for metabolic risk factors by medical history and physical examination, vital signs, ECG, and basic laboratory tests. Basic laboratory tests to assess metabolic parameters and ECG will be repeated at the end of study (Visit 14) to verify whether or not adverse changes were observed in these parameters. Quetiapine has also been shown to cause prolongation of QTc interval which can contribute to cardiac arrhythmias therefore we will exclude veterans with prolonged QTc ≥450 milliseconds. Quetiapine use has been associated with respiratory dysfunction in patients with obstructive sleep apnea. Study participants will be screened for sleep apnea and compliance with continuous positive airway pressure use will be assessed and encouraged at every visit. At risk non-compliant participants will be discontinued from further participation in the study.
Participant safety will be monitored at each weekly visit and Adverse Events (AEs) will be documented. The study coordinator will collect and record side effects, worsening of PTSD symptoms, or suicidal ideations data from participants every week and the study physician will be alerted to clinically manage side effects and implement remedial procedures as indicated.
We will assess blind integrity at the end of each subject’s treatment (i.e. visit 13) by asking the participants and the investigator to guess the placebo or quetiapine treatment assignment [45]. Assessments will be completed by asking: “Which pills do you think you (or participants) were taking in this study, quetiapine or placebo (sugar pill)?” “And why do you think that?”
Materials
Medication dosing
All the participants will continue their standard care prescribed medication. Study drug will be initially dispensed to participants soon after randomization, occurring on the same day as randomization (i.e., Visit 1) so that participants can start taking study medication on the first night immediately following randomization. Initial dose titration will occur during the first two weeks of the study. A participant’s initial titration will be accomplished during one to three dose evaluation telephone calls by the study physician. Using information gathered from participant feedback regarding tolerance of study medication and potentially supplemented by results of clinical assessment, the prescriber will sequentially titrate study medication upward or downward as tolerated. This dose escalation method is comparable to what would be utilized in clinical practice and could therefore be generalized to the intended treatment population. Quetiapine vs. placebo will be initiated at the dose 25 mg at bedtime and then increased up to 200 mg daily as clinically indicated. Dose adjustments will be made in 25-50 mg increments and after at least 14 days of dosing, participants will begin CPT with a VA trained therapist for 12 weekly sessions. Participants will be maintained on their maximally tolerated dose until completion of Visit 13, at which point study medication will be tapered down to the next lower dose for three nights before being discontinued altogether. No taper will be necessary for participants whose maximally tolerated dose was the lowest possible dose. Any change in study medication dose will be documented on the designated Case Report Form. A note will be entered in the CPRS to record the reason for the dose change, document that the change was communicated to the participant and that the participant verbalized an understanding of the change. The participants will be instructed to bring their pill bottles with them to each post-baseline visit to allow pill-count measures of medication compliance. Compliance with the study drug will also be assessed using participant report. The participant will be instructed to return any remaining supply in his/her possession. The Research Pharmacy will maintain the drug accountability log. Participants who does not initiate and continue study medication for at least 2 weeks or first CPT session will be terminated.
Cognitive processing therapy (CPT)
All participants will receive individual weekly CPT as a standard of care within the STVHCS. At STVHCS CPT is delivered in twelve 60-minute sessions following the model established by Resick et al [5]. Which includes the trauma narrative component. For this study, we will exclude participants who previously completed a course of CPT but will permit those with ongoing PTSD symptoms who previously dropped out with the hypothesis that quetiapine randomization may help them to complete. Our study will use clinical standard of care procedures for participants who miss sessions. In our clinic, 12 sessions of CPT are generally delivered in 16-20 weeks. Thus, we have defined treatment endpoints as having completed CPT treatment or until 20 weeks of therapy time elapses. The participants will not be allowed to participate in any other clinical study, start a new medication, or a psychotherapeutic treatment during study participation.
Safety
Participants will be provided with emergency contact information for the study staff. In circumstances such as hospitalization or serious side effects such as suicidal or homicidal ideations, participants will contact the study staff. If the situation requires, the blind will be broken for emergency medical necessity (emergency unmasking), wherein knowledge of the study treatment assignment will influence the medical treatment of the participant, participants will be transferred to an emergency department or inpatient psychiatric unit. Participation in the trial will be terminated and a study discontinuation visit will be scheduled when feasible. Participants will be thanked for study participation and the study physician will coordinate indicated care with the mental health service.
Analysis plan
This pilot study is not designed for efficacy or mechanistic hypotheses testing [46,47]. As a rough guide to future planning, conventional effect sizes will be calculated with 95% confidence limits [48]. For dimensional scales (e.g., PCL-5, ISI, GAD-7, WHOQOL-BREFF, WHODAS 2.0, CAPS-5), effect sizes will be model-based estimates of pre-post treatment change divided by baseline standard deviations (e.g., bias-adjusted Hedges’g). Cohen’s index (h) [49], odds ratios, and number needed to treat will be calculated for proportions. Although the statistical power of this study is limited, we will perform statistical analyses appropriate for an adequately powered study to identify data analysis issues germane to future planning, e.g., data management and scoring, missing data, data distributions, outliers, nature of trends over time, covariance structures. Statistical analyses will be intent to treat, using all available data from randomized participants regardless of extent of participation in treatment.
For dimensional measures related to clinical outcome (i.e., PCL-5, ISI, GAD-7, and 12-point self and therapist report measure of engagement), comparison of means will be done with general or generalized linear mixed effects regression models with repeated measures, with fixed effects of treatment, time, and the treatment by time interaction (e.g., SAS MIXED, GLIMMIX). When measures are assessed only at two time points, the treatment by time interaction is a test of the difference in pre-post change (i.e., CAPS-5, WHOQOL-BREFF, WHODAS 2.0, PTGI). For dichotomous measures of treatment engagement, statistical analyses will be done using chi-square tests. Either logistic or proportional hazard survival regression analysis will be used to determine if baseline descriptive and clinical characteristics predict treatment completion.
Recovery will be measured by a latent variable analysis using scores of three highly correlated indicator variables including the WHODAS 2.0, WHOQOL-BREF, and PCL-5. To reduce Type I error and account for the substantial overlap among functional disability, quality of life, and PTSD symptoms, we will: i) utilize preliminary factor analysis to create composite functional impairment factor scores for Veterans at three time points. The first time point will be at baseline (screening). Composite factor scores will also be created for their level of functional impairment at the visit 7 (week 8) interview and the end of study (Visit 13 (week 14)); ii) Scores on each of the measures will be standardized on the mean and standard deviation of each across the three time points prior to the factor analyses, so that comparisons can be made across time; iii) For each time point, a single, standardized factor will be extracted that accounts for the majority of the variance in the indicator variables; and iv) We expect that factor loadings for the indicators will be also quite high across all three time points, providing strong empirical support for an overall “functional impairment” factor.
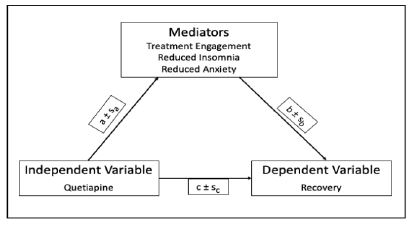
Hypothesis 3 proposes that quetiapine promotes recovery by increasing treatment engagement and reducing insomnia and anxiety. The mediation hypothesis is typically represented in a triangular diagram (Figure 3), which depicts a direct causal path from treatment to outcome (path c), and an indirect path from treatment through the mediator (path a) to outcome (path b). If mediation is complete, path c disappears, but partial mediation is also possible. The paths and standard errors are estimated with appropriate (i.e., linear, logistic) regression models or Simultaneous Equation Modeling (SEM), which estimates the causal paths and standard errors simultaneously. The product of those paths (a x b) equals the decrement in the direct path due to mediation. The Figure shows the simplest case with only one mediator, but it is readily expanded to include more. The statistical significance of the indirect effect can be tested parametrically with estimates of its standard error, but bootstrapping is generally considered preferable because the distribution of the indirect effect is typically non-normal. Macros for these computations in SPSS and SAS can be downloaded from the internet (e.g., the PROCESS macro, available at: [50]).
Discussion
The current study is the first study to evaluate quetiapine augmentation of CPT given as a standard of care for individuals with PTSD. Emotional processing theory posits that fear activation is an essential component of successful PTSD treatment, and the degree of emotional response during trauma-focused therapy has been associated with the magnitude of clinical improvement [51]. However, it is not clear that the physiologic arousal that occurs with emotional reactions per sec, is a necessary component of fear extinction learning or is just a secondary consequence of the more critical component of extinction involving fear-related stimuli under the safe conditions of therapy [52]. This project is innovative in that it challenges the presumption that psychosedative medication effects may be counter-therapeutic.
Previous studies using alprazolam have suggested that psychosedation with benzodiazepines may be counter-therapeutic because of impaired fear extinction learning during virtual reality-based exposure therapy [53-55]. However, these negative effects of benzodiazepines could be due to γ-Aminobutyric Acid (GABA)-mediated impairment of the learning that must occur with trauma-focused therapies [55]. A recent pilot trial of intranasal oxytocin compared with placebo showed lower PTSD symptoms and higher working alliance scores when combined with prolonged exposure therapy, which suggests that pharmacological reductions of symptoms are possible, while preserving the benefits of psychotherapy intervention [28].
We initially considered a randomized, double-blind, placebo-controlled comparison of quetiapine vs. placebo in patients for whom existing medications are discontinued. However, this introduces the problem that the 50% of participants receiving placebo only would be completely denied of psychotropic standards of care in significantly symptomatic individuals. We then considered the provision of adding back certain allowable standard of care medications such as sertraline, trazodone, and/or prazosin open label to address breakthrough anxiety, sleep, and depression. However, this was dismissed due to the possibility that added rescue medicines could interact with CPT outcomes and confuse interpretability of data. We also considered blinding by compounding active drug mixed with corn starch to fill opaque size gelatin capsules prepared by the VA research pharmacist and medication dispensed in equal number of capsules to both quetiapine and treatment as usual group. This approach raised several issues related to integrity of the blinding and feasibility. We thought of embracing a randomized, open-label trial comparing quetiapine monotherapy with TAU polypharmacy practices that exclude use of quetiapine. It raised the concern regarding expectations and engagement variables associated with discontinuation of standard of care and substitution to a new investigational drug. We decided against placebo-controlled add-on to the standard medication initially for tolerability concerns due to sedative effects in addition to other sedating medications but finally decided to conduct a trial of quetiapine vs placebo add-on to existing standard of care medications. We have prohibited concomitant use of other sedative medications to prevent the danger of additive sedative side effects for those who receive quetiapine. However, this should not be a problem limiting recruitment because our recently completed pilot study and VHA Support Service Center shows that only 15 to 20% of patients in STVHCS are prescribed these medications, with about 5-10% actually taking them as prescribed.
Conclusion
We expect that the success of this ongoing study should provide us with the preliminary data necessary for a full-scale randomized trial. Positive efficacy results in a full-scale trial should inform new VA guidelines for clinical practice by showing that quetiapine-related improvements in patient engagement and retention may be the most effective approach to assure that VA resources achieve the best possible outcome for veterans.
Declarations
Ethics approval and consent to participate: All study procedures are approved and monitored by the University of Texas Health Science Center at San Antonio Institutional Review Board and STVHCS Research and Development Committee. The study was conducted in accordance with declaration of Helsinki. In addition, all study participants completed a written informed consent prior to any study procedure and were eligible to receive other standard of care treatments within their VA.
Consent for publication: The views expressed herein are solely those of the authors and do not reflect an endorsement by or the official policy or position of the South Texas Veterans Healthcare System, the University of Texas Health Science Center at San Antonio, the University of Texas at San Antonio, the University of Pittsburgh, the Department of Veterans Affairs, or the U.S. government.
Availability of data and material: Final data sets underlying all publications resulting from this pilot study will be shared pursuant to a Data Use Agreement (DUA) appropriately limiting use of the dataset and prohibiting the recipient from identifying or re-identifying (or taking steps to identify or re-identify) any individual whose data are included in the dataset. We will make sufficient data and descriptors available to confirm conclusions in the publication, run duplicate statistical analysis, and perform additional analyses.
Competing interests: The authors declare that they have no conflict of interest.
Funding: This project is supported by the UTHSCSA School of Medicine Grantseekers 2.0 Pilot Program grant funded to MRB and American Psychological Foundation Walter Katkovsky Research Grants (WKRG) program grant funded to JLW and RDW. The aim of the WKRG program is to stimulate research that combines psychotherapy with an adjunct psychoactive substance. [More information about the WKRG program is available at https://www.apa.org/apf/funding/katkovsky. The funding sources had no involvement in the study design, the collection, analysis and interpretation of data, the writing of this manuscript, or the decision to submit this manuscript for publication.
Authors’ contributions: MRB had full access to all the information about the study and take full responsibility for the accuracy of the information provided. MRB and JDR designed the study. JM, ALP, and ECM provided critical review of the protocol and manuscript for important intellectual content. MRB, RDB, JLW, and JAL provided clinical supervision of participants. MRB drafted the manuscript. All authors read and approved the final manuscript.
Acknowledgements: The authors thank the participants in this study for their invaluable contribution. Megan Atkinson and Jamie Timmerman provided administrative support. Dr. Baig’s salary is supported by the Department of Veterans Affairs.
The authors thank the participants in this study for their invaluable contribution. We thank the psychotherapists for their diligent care of our participants in providing CPT especially Emma Mata-Galán, Psy.D., Jeremy Crostley, Ph.D. ABPP, and Holly Darling, LCSW, LCDC.
References
- Krystal JH, et al. It Is Time to Address the Crisis in the Pharmacotherapy of Posttraumatic Stress Disorder: A Consensus Statement of the PTSD Psychopharmacology Working Group. Biol Psychiatry. 2017.
- Friedman MJ, et al. Randomized, double-blind comparison of sertraline and placebo for posttraumatic stress disorder in a Department of Veterans Affairs setting. J Clin Psychiatry. 2007; 68: 711-720.
- Treatment of Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment. 2014, Committee on Treatment of Posttraumatic Stress Disorder. Institute of Medicine: Washington, DC, USA.
- (DoD), V.A.V.D.o.D., Managment of Posttraumatic Stress Disorder and Acute Stress Reaction (2017), in Clinical Practice Guidelines 2017 U.S. Department of Veterans Affairs
- Patricia A Resick, Candice M Monson, Kathleen M Chard. Cognitive Processing Therapy: Veterans/Military Version: Therapist’s manual. Department of Veterans’s Affairs: Washington, DC. 2014.
- Miles SR, et al. Fear of Losing Emotional Control Is Associated With Cognitive Processing Therapy Outcomes in U.S. Veterans of Afghanistan and Iraq. J Trauma Stress. 2015; 28: 475-479.
- Hundt NE, et al. It didn’t fit for me: A qualitative examination of dropout from prolonged exposure and cognitive processing therapy in veterans. Psychol Serv, 2018.
- Belleau EL, et al. Pre-treatment predictors of dropout from prolonged exposure therapy in patients with chronic posttraumatic stress disorder and comorbid substance use disorders. Behav Res Ther. 2017; 91: 43-50.
- Baig MR, et al. Enhancing Access to Psychiatric Care for Posttraumatic Stress Disorder in Veterans with Mild Traumatic Brain Injury through Integrated Services. Psychiatr Q. 2019; 90: 815-827.
- Jeffreys MD, et al. Evaluating treatment of posttraumatic stress disorder with cognitive processing therapy and prolonged exposure therapy in a VHA specialty clinic. J Anxiety Disord, 2014; 28:108-114.
- Imel ZE, et al. Meta-analysis of dropout in treatments for posttraumatic stress disorder. J Consult Clin Psychol. 2013; 81: 394-404.
- Krystal JH, et al. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: A randomized trial. Jama. 2011; 306: 493-502.
- Davis LL, et al. Divalproex in the treatment of posttraumatic stress disorder: A randomized, double-blind, placebo-controlled trial in a veteran population. J Clin Psychopharmacol. 2008; 28: 84-88.
- Villarreal G, et al. Efficacy of Quetiapine Monotherapy in Posttraumatic Stress Disorder: A Randomized, Placebo-Controlled Trial. Am J Psychiatry. 2016; 173: 1205-1212.
- Horacek J, et al. Mechanism of action of atypical antipsychotic drugs and the neurobiology of schizophrenia. CNS Drugs. 2006; 20: 389-409.
- Robert S, et al. Quetiapine improves sleep disturbances in combat veterans with PTSD: Sleep data from a prospective, open-label study. J Clin Psychopharmacol. 2005; 25: 387-388.
- Galovski TE, et al. Augmenting cognitive processing therapy to improve sleep impairment in PTSD: A randomized controlled trial. J Consult Clin Psychol. 2016; 84: 167-177.
- Gedge L, et al. Effects of quetiapine on sleep architecture in patients with unipolar or bipolar depression. Neuropsychiatr Dis Treat. 2010; 6: 501-508.
- Ma L, et al. Quetiapine attenuates cognitive impairment and decreases seizure susceptibility possibly through promoting myelin development in a rat model of malformations of cortical development. Brain Res. 2015; 1622: 443-451.
- Matsumoto Y, et al. Vorinostat ameliorates impaired fear extinction possibly via the hippocampal NMDA-CaMKII pathway in an animal model of posttraumatic stress disorder. Psychopharmacology (Berl). 2013; 229: 51-62.
- Acheson D, et al. The effect of intranasal oxytocin treatment on conditioned fear extinction and recall in a healthy human sample. Psychopharmacology (Berl). 2013; 229: 199-208.
- Popiel A, et al. Prolonged exposure, paroxetine and the combination in the treatment of PTSD following a motor vehicle accident. A randomized clinical trial - The “TRAKT” study. J Behav Ther Exp Psychiatry. 2015; 48: 17-26.
- Schneier FR, et al. Combined prolonged exposure therapy and paroxetine for PTSD related to the World Trade Center attack: A randomized controlled trial. Am J Psychiatry. 2012; 169: 80-88.
- Simon NM, et al. Paroxetine CR augmentation for posttraumatic stress disorder refractory to prolonged exposure therapy. J Clin Psychiatry. 2008; 69: 400-405.
- Echiverri-Cohen A, et al. Changes in temporal attention inhibition following prolonged exposure and sertraline in the treatment of PTSD. J Consult Clin Psychol. 2016; 84: 415-426.
- Jun JJ, Zoellner LA, Feeny NC. Sudden gains in prolonged exposure and sertraline for chronic PTSD. Depress Anxiety. 2013; 30: 607-613.
- Jerud AB, et al. The effects of prolonged exposure and sertraline on emotion regulation in individuals with posttraumatic stress disorder. Behav Res Ther. 2016; 77: 62-67.
- Flanagan JC, et al. Augmenting Prolonged Exposure therapy for PTSD with intranasal oxytocin: A randomized, placebo-controlled pilot trial. J Psychiatr Res. 2017; 98: 64-69.
- Baig MR, et al. Enhancing Completion of Cognitive Processing Therapy for Posttraumatic Stress Disorder with Quetiapine in Veterans with Mild Traumatic Brain Injury: A Case Series. Psychiatr Q. 2019; 90: 431-445.
- Spitzer RL, et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006; 166: 1092-1097.
- CM M. Insomnia: Psychological assessment and management. 1993; Guilford Press.: New York, NY.
- Kaufmann CN, et al. Psychometric Characteristics of the Insomnia Severity Index in Veterans With History of Traumatic Brain Injury. Behav Sleep Med. 2019; 17: 12-18.
- Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001; 2: 297-307.
- Mollayeva T, et al. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med Rev. 2016; 25: 52-73.
- Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP, et al. National Center for PTSD, The PTSD Checklist for DSM-5 (PCL-5) – [Measurement instrument]. 2013.
- Murphy D, et al. Exploring optimum cut-off scores to screen for probable posttraumatic stress disorder within a sample of UK treatment-seeking veterans. Eur J Psychotraumatol. 2017; 8: 1398001.
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998; 28: 551-558.
- Schumm JA, et al. Examination of the World Health Organization Disability Assessment System as a Measure of Disability Severity Among Veterans Receiving Cognitive Processing Therapy. J Trauma Stress. 2017; 30: 704-709.
- Weathers FW, Blake DD, Schnurr P. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) - Past Month [Measurement Instrument]. 2015.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001; 16: 606-613.
- Tedeschi RG, Calhoun LG. The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. J Trauma Stress. 1996; 9: 455-471.
- Saunders JB, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction. 1993; 88: 791-804.
- Berman AH, et al. Evaluation of the Drug Use Disorders Identification Test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. Eur Addict Res. 2005; 11: 22-31.
- Bharmal M, et al. Validation of an abbreviated Treatment Satisfaction Questionnaire for Medication (TSQM-9) among patients on antihypertensive medications. Health Qual Life Outcomes. 2009; 7: 36.
- Sharpe L, et al. Testing for the integrity of blinding in clinical trials: How valid are forced choice paradigms? Psychother Psychosom. 2003; 72: 128-131.
- Kraemer HC, et al. Caution regarding the use of pilot studies to guide power calculations for study proposals. Arch Gen Psychiatry. 2006; 63: 484-489.
- Leon AC, Davis LL, Kraemer HC. The role and interpretation of pilot studies in clinical research. J Psychiatr Res. 2011; 45: 626-629.
- Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008; 31: 180-191.
- Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale, New Jersey: Erlbaum Associates. 1988.
- Hayes AF. The PROCESS macro for SPSS, SAS, and R. 2020; Available from: https://processmacro.org/index.html.
- Rauch SA, et al. Imagery vividness and perceived anxious arousal in prolonged exposure treatment for PTSD. J Trauma Stress. 2004; 17: 461-465.
- Deacon B, et al. Maximizing the efficacy of interoceptive exposure by optimizing inhibitory learning: A randomized controlled trial. Behav Res Ther. 2013; 51: 588-596.
- Lund BC, et al. Declining benzodiazepine use in veterans with posttraumatic stress disorder. J Clin Psychiatry. 2012; 73: 292-296.
- Viola J, et al. Pharmacological management of post-traumatic stress disorder: Clinical summary of a five-year retrospective study, 1990-1995. Mil Med. 1997; 162: 616-619.
- Rothbaum BO, et al. A randomized, double-blind evaluation of D-cycloserine or alprazolam combined with virtual reality exposure therapy for posttraumatic stress disorder in Iraq and Afghanistan War veterans. Am J Psychiatry. 2014; 171: 640-648.