
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Mucinous tumor of transverse colon presenting with colo-colic
intussusception in a 24-year old female: Aggressive tumor with
a rare presentation in a young female
Wafa Alqahtani1*; Ammar Ashraf1; Haseeb Khokhar2; Mohamed Tahar Yacoubi3
1Department of Medical Imaging, King Abdulaziz National Guard Hospital, Al-Ahsa, KSA.
2Department of General/Colorectal Surgery, King Abdulaziz National Guard Hospital, Al-Ahsa, KSA.
3Department of Anatomical Pathology, King Abdulaziz National Guard Hospital, Al-Ahsa, KSA.
*Corresponding Author : Wafa Alqahtani
Department of Medical Imaging, King Abdulaziz National Guard Hospital, Al-Ahsa, KSA.
Email: wafaalqahtani96@gmail.com
Received : Oct 03, 2022
Accepted : Oct 25, 2022
Published : Nov 01, 2022
Archived : www.jcimcr.org
Copyright : © Alqahtani W (2022).
Abstract
Background: Intussusception is the most common cause of bowel obstruction in the children. However, it is rare in the adults, accounting for only 5% of all cases of bowel obstruction. In Adult Intussusception (AI), an underlying pathology can be demonstrated in majority of the cases. Malignancy is the most common cause of colonic intussusception. We present a case of colonic intussusception due to an underlying primary malignancy in a young female.
Case presentation: A 24-year-old single female with no previous family history of Colorectal Cancer (CRC) presented to the emergency department with severe colicky pain in the right hypochondrium and right lumbar region. The pain was associated with nausea, vomiting, diarrhea, anorexia and weight loss. An intussusception was discovered on abdominal Ultrasound (US) examination which was later confirmed to be colonic in origin and associated with an underlying mass lesion on Computed Tomography (CT) scan of the abdomen and pelvis. The patent underwent colonoscopy and biopsy followed by the extended right hemicolectomy and the histopathology confirmed mucinous adenocarcinoma. The postoperative period was uneventful and later on, the patient was referred to the medical oncologist for further management.
Conclusion: Colonic intussusception is rare in adults and usually secondary to a malignant lesion in patients >50 years of age. We describe a rare case of transverse colon malignancy in a young female presenting as an intussusception. The surgeons and the radiologists must be mindful of underlying malignancy irrespective of the age in any adult patient presenting with a colo-colic intussusception.
Keywords: Intussusception; Adult intussusception (AI); Mucinous; colo-colic; Colorectal cancer (CRC).
Abbreviations: AI: Adult Intussusceptions; CT: Computed Tomography; US: Ultrasound; CRC: Colorectal Cancer.
Citation: Alqahtani W, Ashraf A, Khokhar H, Yacoubi MT, et al. Mucinous tumor of transverse colon presenting with colo-colic intussusception in a 24-year old female: Aggressive tumor with a rare presentation in a young female. J Clin Images Med Case Rep. 2022; 3(11): 2131.
Introduction
Intussusception is the most common cause of bowel obstruction in the pediatric population [1-5]. Intussusception is rare in adults with an estimated incidence of 2 cases/1,000,000 population/year, accounting for only 5% of all intussusceptions, 1% of all bowel obstructions, and 0.003-0.02% of all hospital admissions [2-9]. Amongst the Adult Intussusceptions (AI), 38–44% occur in the colon and 52–55% in the small intestine [4,6]. AI has various clinical presentations when compared to the pediatric form [8,10]. The classic triad of pain, hematochezia and a palpable mass is most often absent in the adults and the patients can present acutely, sub acutely or with a chronic history, most often with nonspecific obstructive type symptoms [5,8]. Due to this variable presentation, AI is difficult to diagnose, despite the evolution of imaging procedures and often remains unrecognized or misdiagnosed prior to surgery [2,5,10]. Abdominal Ultrasound (US) and Computed Tomography (CT) scan have high sensitivity for the diagnosis of AI but limited value in discriminating whether a lead point is malignant, benign, or idiopathic [3,10].
The underlying etiology and management also differ greatly in the adult population when compared to children [8]. 90% of the AI patients harbor a pathological lead point which is in contrast to the intussusception in the pediatric age group, where approximately 90% of the cases are idiopathic, often influenced by anatomic or infection related factors [1,2,4,5,8,10,11]. In the pediatric population, non-surgical management such as pneumatic or hydrostatic reduction is sufficient in 80% of the patients whereas surgery, often with bowel resection, is the recommended treatment for majority of the patients with AI, although the optimal surgery remains controversial [1,5,6,8,10,11]. In AI, the early and correct diagnosis of the etiology and timely treatment are very important; however, most patients are diagnosed late as a result of a poor index of suspicion and misdiagnosis [2,3].
Here, we present a case of colo-colic intussusception due to an underlying mucinous adenocarcinoma in a young female. To the best of our knowledge, we are not aware of a case of colo-colic intussusception due to mucinous tumor in such a young patient with no family history of bowel carcinoma.
Case presentation
A 24-year-old single female presented to the emergency department with severe colicky pain in the right hypochondrium and right lumbar region. She reported multiple episodes of similar pain in the last 4 months, with worsening of the pain in the last 7 days. The pain was associated with nausea, vomiting and diarrhea. No history of radiation of the pain or any associated aggravating or relieving factors. There was also history of anorexia and 30 kilograms weight loss in the last 4 months. No history of bleeding per rectum, melena, hematemesis, fever or sweating. No respiratory, urinary and gynecological symptoms. Her personal medical history was unremarkable. She had no family history of bowel cancer but her mother had gallbladder cancer.
On physical examination, the patient was in pain with a pain score of 10/10 and mildly dehydrated. Except mild tenderness in the right hypochondrium, abdomen was soft and non-distended with normal bowel sounds. She had a temperature of 36.6oC, pulse of 105 beats/minute, blood pressure of 138/80 mmHg, respiratory rate of 20 breaths/ minute, and oxygen saturation of 100% on room air. Her weight was 64.35 kg, height 158 cm with a BMI of 25.78 Kg/m2. Except low hemoglobin {89 g/L (120-160 g/L)}, all laboratory tests were within normal limits.
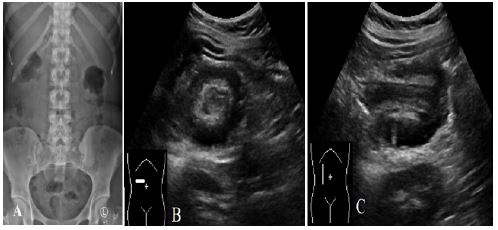
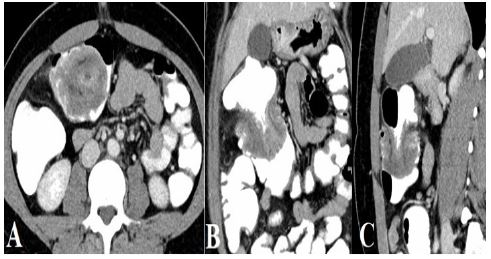
Plain abdominal radiograph was negative for any acute abdominal finding. A provisional clinical diagnosis of cholelithiasis / cholecystitis was made by the emergency department physician and an abdominal US examination was requested. US was negative for any gallbladder disease but it showed a bowel-related persistent lesion in the right hypochondriumwith swirled pattern of alternating hyper and hypo-echogenicities, resembling a target sign on axial images, suggestive of intussusception. However, its exact origin (enteric or colonic) was not clear. The patient was referred to the general surgery and a contrast enhanced CT scan of the abdomen and pelvis was performed which showed circumferential irregular mural thickening of the proximal transverse colon with colo-colic intussusception associated with a few small sub centimeter loco-regional lymph nodes. No bowel obstruction, pneumoperitoneum or other significant finding was noted. CT chest was organized as part of staging which was found to be normal. All tumor markers including Carcinoembryonic Antigen (CEA) and Lactate Dehydrogenase (LDH) were normal.
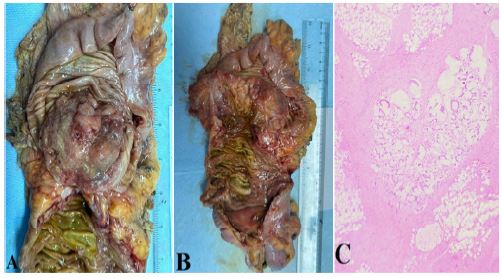
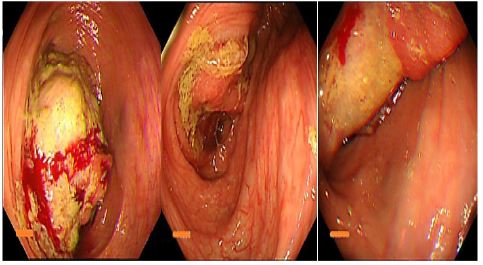
Based on these imaging findings, the patent underwent colonoscopy the next day which showed an irreducible colonic intussusception at the hepatic flexure with congested friable mucosa and multiple biopsies were taken which came positive for mucinous carcinoma. The next day, the patient underwent laparoscopic extended right hemicolectomy and the histopathology showed grade II moderately differentiated mucinous adenocarcinoma, measuring 7 x 5 x 2.5 cm with tumor invading the muscularis propria into the pericolonic fat. One out of 24 (1/24) lymph node was positive for metastasis. As per pTNM, AJCC 8th edition, the tumor stage was pT3, pN1a, pM0. Microsatellite Stability Index (MSI) was 0/7. Later on, the patient was referred to the medical oncologist for adjuvant chemotherapy.
Discussion
Intussusception is defined as telescoping of a proximal bowel loop (known as the intussusceptum) into an immediately adjacent distal bowel loop (known as the intussuscipiens) [1,3-6,8,10-12]. It is an uncommon type of bowel obstruction which usually results from a disturbance in the normal peristalsis secondary to pathology in the wall of the intestine [1,5,8,11]. Intussusception commonly affects the junctions between the freely mobile and fixed bowel segments; e.g. mobile intraperitoneal ileum intussuscepting into the fixed, retroperitoneal cecum and it rarely affects the proximal gastrointestinal tract structures like esophagus, stomach and duodenum due to their immobility and anatomical fixation [8].
It is usually considered a disease of infants and young children and is uncommon in the adults with a child to adult ratio of nearly 20:1 [1,5]. AI can affect any part of the bowel; however, it is more common in the small bowel and affects the colon in only 20-25% [2,7,8,11-13]. In adults, the colonic intussusception is commonly seen in the sigmoid colon, transverse colon, and the cecum [6]. Approximately 90% of the cases of intussusception in the pediatric population are idiopathic; however, 90% cases of Adult Intussusception (AI) are secondary to a well-known pathological lead point and only 5% of the large bowel and 16% of the small bowel intussusceptions are idiopathic [1,2,4,5,11]. 65-70% of cases of large bowel intussusception and 30-35% of cases of small bowel intussusception are secondary to the malignancy [1,2,6]. 30% of the enteric and 66% of the colonic intussusceptions in the adults are due to adenocarcinoma [4]. Most of the large bowel intussusceptions are due to adenocarcinoma of the colon whereas most of the small bowel intussusceptions are secondary to the metastasis [5].
The nomenclature of the intussusception describes its location and the underlying etiology. Depending on the location, intussusception is usually categorized in to entero-enteric (limited to the small bowel), colo-colic (limited to the colon), ileo-colic (terminal ileum prolapsing into the ascending colon), and ileo-cecal (ileo-cecal valve acting as the lead point) [1,4,5,11]. Depending on the underlying etiology, it can also be classified in to primary (or idiopathic) and secondary (malignant and benign) intussusception [4,6].
In approximately 20% cases of AI, no clear underlying cause is found and these cases are labelled as primary or idiopathic intussusceptions and such intussusceptions are more commonly seen in the small intestine [1].
Secondary AI have a lead point and majority of these lead points in the small bowel are benign. Benign causes of AI include intestinal lipomas, leiomyomas, inflammatory polyps, fibromas, hamartomas, Meckel’s diverticulum, cystic fibrosis, scleroderma, foreign bodies, appendicitis and post-operative adhesions [1,4-6].
Malignant causes of AI include adenocarcinoma, carcinoids, lymphoma, GIST, malignant polyps, leiomyosarcomas, and metastatic tumors [1,2,4,6,11,12]. Patient with celiac disease and Crohn’s disease are famous to present with transient small bowel intussusception without any lead point [1,5].
Our patient had colo-colic intussusception in the proximal transverse colon secondary to the underlying primary mucinous adenocarcinoma of the colon.
Clinical features
The clinical presentation of AI is non-specific and variable [4,5]. Patients may present with acute (enteric intussusception), subacute or chronic symptoms (colonic intussusception) of bowel obstruction and most of the patients predominantly present with abdominal symptoms of chronic partial bowel obstruction [1,4,5,8]. Abdominal pain is the commonest symptom. Other symptoms can be nausea, vomiting, constipation, gastrointestinal bleeding, altered bowel habits, bloating and abdominal distention [3-5,12]. These symptoms are non-specific and can simulate with other more common abdominal pathologies like bowel obstruction, gastroenteritis and inflammatory bowel disease, thus making the clinical diagnosis of intussusception difficult [4]. In case of late presentation with delayed diagnosis, the patient can present with complications of intussusception like bowel ischemia, bowel perforation, peritonitis and shock [12]. Clinical examination may show abdominal tenderness, abdominal distension and rarely a palpable mass; however, most of the time, no significant positive finding is seen [4,8,12]. Due to low incidence and variable clinical presentation, diagnosis of AI needs a high clinical suspicion and further evaluation with imaging, particularly CT scan [4,8]. Chronic abdominal pain and weight loss were the predominant complaints in our patient.
Imaging work up
In adults, the preoperative diagnosis of intussusception is usually laborious [2]. Intussusception in adults can be evaluated with different imaging modalities including plain abdominal radiograph, ultrasound, barium enema, cross sectional imaging like CT scan of the abdomen and colonoscopy [1,2,6]. The plain abdominal radiograph is usually nonspecific and non-diagnostic in intussusception but can show air-fluid levels if it is complicated with bowel obstruction [5,6]. Bowel enema and CT can recognize the etiology of intussusception [2]. Barium enema is helpful in colo-colic or ileo-colic intussusceptions and shows the classical “meniscus and coiled spring signs” [2,6]. It is used as a first-line therapeutic procedure for intussusception in children but has no role in adults [6]. Once used as a classical examination method in the diagnosis of intussusception in the past, has now been replaced by abdominal US and CT [3].
The abdominal US is a useful imaging modality in the diagnosis of intussusception and has a reported accuracy of 60-83.3% [1,2,4-6,11,14]. A typical intussusception has well-recognized classical sonographic features which are “target, doughnut or bull’s eye sign” on the transverse view (concentric alternating hypo- and hyper-echoic bands) and “pseudokidney or hayfork sign” on the longitudinal view (hyperechoic mesenteric fat within the intussusception surrounded by the bowel wall) [1,2,4-6,11,14]. US is fast, cheap, non-invasive, readily available, easy to perform and carries no radiation risks [1,2,6]. It can be used in the follow up of transient, self-limiting intussusceptions seen in inflammatory bowel disease and celiac disease [1]. Beware of diseases associated with bowel wall thickening which may simulate intussusception [2]. Also remember that this imaging modality is operator dependent which is a major limitation [1,2,6]. Obesity and bowel gases are other limitations of this modality [1].
Contrast enhanced CT scan of the abdomen and pelvis is the imaging modality of choice in the evaluation of intussusception [1,2,5,6,8,12]. CT can identify the underlying cause of intussusception and is considered the most sensitive preoperative imaging modality when compared with ultrasound, fluoroscopy and colonoscopy [2,3,10,15]. CT has a diagnostic accuracy of 58-100% in diagnosing an intussusception [8,11,14]. CT scan is more precise in AI and has shown a diagnostic accuracy of nearly 100% in one study [4,11]. Identification of a bowel within bowel configuration with or without mesenteric vessels and fat is pathognomonic for intussusceptions [1]. Intussusception is seen as a target mass (axial plane) and sausage shaped mass (longitudinal plane) [1,2,4-6]. CT scans also provides other important information such as location and type of intussusception, length and diameter of the intussusception, possible lead point, mesenteric vasculature, possibility of strangulation, bowel obstruction and adjacent viscera [1,2,12]. Intussusception measuring less than 4 cm in length is likely transient and can be managed conservatively as compared to the intussusceptions measuring 9.6 cm in length [1]. Similarly, intussusception measuring less than 3.2 cm in diameter is likely transient whereas intussusceptions measuring more than 4.8 cm in diameter is likely pathological [1]. 50% of the intussusceptions with a lead point and intestinal obstruction are likely pathological intussusceptions [1].
Abdominal CT scan can discriminate primary (idiopathic) and secondary intussusceptions, depict complications of the intussusception and differentiate the intussusception from other abdominal emergencies and these CT scan findings play a key role in the management decision and can prevent unnecessary surgeries [2,10,12].
Neoplasms act as a leading pointin 70% of cases of colonic intussusception and approximately 70% of these neoplasms are malignant [2,8]. With this high prevalence of underlying malignancy in the colonic intussusception, CT also provides excellent additional preoperative information of such malignancy regarding its locoregional extension as well as the distant metastasis [2,8].
Colonoscopy is valuable in colo-colic, ileo-colic and ileo-cecal adult intussusceptions [1,4,6]. Colonoscopy not only confirms the presence and location of intussusception but also helps in the recognition of an underlying lead point which can be biopsied to clinch a diagnosis which is crucial in further treatment planning [1,4,6]. Colonoscopy and biopsy should be averted in patients with complicated intussusception with suspicion of ischemia or perforation [6,4,11].
In our case, the abdominal radiograph was unremarkable. The intussusception was detected on the abdominal US although it was limited in determining its exact location and the underlying etiology, and these shortcomings were addressed by the CT scan and colonoscopy. On CT scan, the intussusception was measuring 6 cm in diameter and 6.5 cm in length. Furthermore, the CT scan and colonoscopy findings were highly suggestive of a malignant pathological lead point which was later affirmed by the histopathology.
Treatment
There is no universal consensus on the optimal management of the AI [2,4,12]. The management decision depends on the location of the intussusception and age of the patient [1,3,6,8,10]. In children, the enteric intussusceptions usually reduce spontaneously whereas the ileo-colic intussusceptions are managed with hydrostatic or pneumatic reduction; however, such therapeutic reduction is not recommended in the adults [4,5,8]. Surgery (laparoscopy or exploratory laparotomy) is the treatment of choice in AI depending on the location and nature of the underlying etiology; however, reduction of the intussusceptum before bowel resection is still debatable [3-5,9,10]. Surgery is indicated in patients presenting with intestinal obstruction, bowel related mass on imaging, systemic symptoms of malignancy (e.g. fever, anorexia, weight loss etc.) and colo-colic and ileo-colic intussusceptions due to increased risk of underlying malignancy [4].
When surgery is indicated in the intussusception, intussusception is surgically resected in the adults whereas it is surgically reduced in the pediatrics [4,12]. In case of any suspicion of underlying malignancy, oncologically adequate en bloc removal of the affected bowel segment along with the associated mesentery should be considered and, in such cases, preoperative colonoscopy with tissue diagnosis of the underlying cause is helpful in surgical treatment planning [4,12]. Bowel ischemia, severe bowel edema, strangulation and leukocytosis are other indications of surgery due to high risk of bowel perforation [1,10,12].
In cases with suspected bowel ischemia, en bloc removal of the affected bowel segment without reduction will minimize the contamination [10]. Also, in view of high risk of malignancy in colonic intussusception in the adults, en bloc surgical resection without reduction is advocated not only due to lack of discrimination between malignant & benign lesions pre or intra-operatively but alsoto avoid the probable risk of local or distant tumor dissemination [1,2,5,6,8,10,12]. Intraoperative reduction may avert unnecessary bowel removal, although it can escalate the hazard of tumor seeding [10]. However, some authors consider that these risks are hypothetical and mild traction should be applied in selected cases to minimize the irrelevant resection of normal bowel [5,8].
Radiologic decompression and endoscopic reduction have generally not been the recommended management options in adults and thus 70-90% of cases of AI are managed with definite surgery or laparoscopic reduction [9].
In intussusceptions with a long intussusceptum, intraoperative reduction can be tried which may obviate wide bowel resection [5,10]. In patients with suspicion of a benign polypoidal lesion, intussusception reduction followed by enterotomy and polypectomy can be tried [10]. In tropical areas, due to low incidence of malignancy and larger number of idiopathic intussusceptions when compared with the non-tropical areas, reduction may be a fair substitute for ileocolic and enteric intussusceptions [10]. The patient should be thoroughly investigated with all available imaging modalities preoperatively if there are no acute symptoms [10].
Laparoscopic surgery is safe, minimally invasive, and has speedy recovery, brief postoperative hospital stays and diminished overall complications [3].
In adults, the enteric intussusceptions smaller than 3.5 cm and without any bowel obstruction or suspicion of malignancy are usually self-limiting and can be managed non-surgically [1,2,4,9].
Our patient had significant weight loss (systemic symptom of malignancy), colonic mass with colo-colic intussusception on CT scan & colonoscopy and pathological evidence of malignancy on biopsy. She had no features of bowel ischemia, complete bowel obstruction, bowel perforation or peritonitis. The intussusception was irreducible during the colonoscopy as well as surgery. She underwent oncologically adequate en bloc removal of the affected bowel segment along with the associated mesentery (laparoscopic extended right hemicolectomy).
Conclusion
In conclusion, intussusception in adults is uncommon and its diagnosis is laborious due to its diverse clinical presentation and if not diagnosed and managed in time, may be associated with complications like bowel obstruction, ischemia, perforation and peritonitis with sepsis. AI, particularly the colonic intussusception, can be a presentation of underlying malignancy and its diagnosis needs high index of suspicion. Surgery without preoperative reduction is a decent treatment strategy for AI. Continuous research and awareness of this rare entity may allow the physicians and the radiologists to make a timely precise preoperative diagnosis.
Teaching points
• Intussusception is the most common cause of bowel obstruction in the children; however, it is rare in the adults, accounting for only 5% of all cases of the intussusceptions.
• Approximately 90% of the intussusceptions in the pepediatrics are idiopathic whereas 90% of the intussusceptions in the adults have a pathological lead point and only 5% of the large bowel and 16% of the small bowel intussusceptions in the adults are idiopathic. Non-surgical management is sufficient in 80% of the pediatric patients whereas surgery is the recommended treatment for the majority of the adult patients.
• 38–44% of the AI occurs in the colon and 52–55% occurs in the small intestine. In adults, colonic intussusception is commonly seen in the sigmoid colon, transverse colon, and the cecum.
• 65-70% of cases of large bowel intussusceptions and 30-35% of cases of small bowel intussusceptions are secondary to the malignancy. Most of the large bowel intussusceptions are due to adenocarcinoma of the colon whereas most of the smallbowelintussusceptions are secondary to the metastasis.
• Patient with celiac disease and Crohn’s disease are famous to present with transient small bowel intussusception without any lead point.
• Least but not the last and the take home message: Colonic intussusception in the young adults can be a presentation of an underlying malignancy.
References
- Shenoy S. Adult intussusception: A case series and review. World Journal of Gastrointestinal Endoscopy. 2017; 9: 220–227. https://doi.org/10.4253/wjge.v9.i5.220.
- Al-Radaideh AM, Omari HZ, Bani-Hani KE. Adult intussusception: A 14-year retrospective study of clinical assessment and computed tomography diagnosis. Acta Gastroenterol Belg. 2018; 81: 367-372.
- Su T, He L, Zhou T, Wu M, Guo Y, Wang Q, Jiang J, Cao X, et al. Most adult intussusceptions are caused by tumors: A single-centre analysis. Cancer Management and Research. 2020; 12: 10011–10015. https://doi.org/10.2147/cmar.s268921
- Hadid T, Elazzamy H, Kafri, Z. Bowel intussusception in adults: Think cancer! Case Reports in Gastroenterology. 2020; 14: 27–33. https://doi.org/10.1159/000505511
- Nkembe NM, Mbanga C, Agbor VN. Complicated Idiopathic Ileo-ileal Intussusception in a 45-year-old Male: A Case Report. Int J Case Rep; 2018; 2.
- Shimoyama H, Ueno K, Samizo M. Successful treatment of adult cecorectal intussusception caused by cecum cancer with mobile cecum: A case report. Surgical Case Reports. 2021; 7. https://doi.org/10.1186/s40792-021-01180-0
- de Mesquita G, Carvalho B, de Almeida Medeiros K, Nii F, Martines D, et al. Intussusception reveals mutyh-associated polyposis syndrome and colorectal cancer: A case report. BMC Cancer. 2019; 19. https://doi.org/10.1186/s12885-019-5505-8
- McQuade C, Waters PS, O’Brien C, Crowther S, Torreggiani W, Kavanagh DO, et al. Colorectal intussusception secondary to primary rectal melanoma: A novel case report. International Journal of Surgery Case Reports. 2018; 44: 78–81. https://doi.org/10.1016/j.ijscr.2018.02.015
- AlSamman MA, Ferreira JD, Moustafa A, Moveson J, Akerman P, et al. Successful endoscopic reduction of an ILEOCOLONIC intussusception in an adult with Peutz-JEGHERS syndrome. Gastroenterology Research. 2019; 12: 40–42. https://doi.org/10.14740/gr1130
- Hong KD, Kim J, Ji W, Wexner SD, et al. Adult intussusception: A systematic review and meta-analysis. Techniques in Coloproctology. 2019; 23: 315–324. https://doi.org/10.1007/s10151-019-01980-5
- Marsicovetere P, Ivatury S, White B, Holubar S. Intestinal intussusception: Etiology, diagnosis, and treatment. Clinics in Colon and Rectal Surgery. 2016; 30: 030–039. https://doi.org/10.1055/s-0036-1593429
- Gambardella D, Gambardella D, De Caridi A, Trapuzzano O, Loria G, Maschio V, et al. Adult intussusception secondary to colorectal cancer in a young woman: A case report. Global Surgery Case Reports. 2020; 1–4. https://doi.org/10.31487/j.gscr.2020.02.10
- Toyoda S, Horii K, Okumura S, et al. [Sigmoid colon cancer with intussusception prolapsing through the anus treated by elective laparoscopic radical surgery]. NihonShokakibyoGakkaiZasshi = The Japanese Journal of Gastroenterology. 2018;115(1):87-93. DOI: 10.11405/nisshoshi.115.87. PMID: 29353855.
- Kim JW, Lee BH, Park SG, Kim BC, Lee S, Lee SJ, et al. Factors predicting malignancy in adult intussusception: An experience in university-affiliated hospitals. Asian Journal of Surgery. 2018; 41: 92–97. https://doi.org/10.1016/j.asjsur.2016.11.010
- Knight AM, Haurani C, Hollenbeck A, Greene F, Mostafa G, et al. Intussusception in the adult population: A Challenge to surgeons. The American Surgeon. 2017; 83: 131–133. https://doi.org/10.1177/000313481708300410 (C7)
- Cha PI, Gurland B, Forrester JD. First reported case of intussusception caused byescherichia coliO157: H7 in an adult: Literature review and case report. Surgical Infections. 2019; 20: 95–99. https://doi.org/10.1089/sur.2018.137.