
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Left ventricular pseudoaneurysm and the utility of
non-contrast coronary artery calcium scan in
differentiating acute versus chronic bleed
Lucia P Schroeder*; Venkat S Manubolu; Jairo Aldana Bitar; Matthew J Budoff
Cardiology Division, The Lundquist Institute at Harbor-UCLA Medical Center, Torrance, CA, USA.
*Corresponding Author : Lucia P Schroeder
Cardiology Division, The Lundquist Institute at Harbor-UCLA Medical Center, Torrance, CA, USA.
Tel: 208-867-4732;
Email: lucipschroeder@gmail.com
Received : Sep 27, 2022
Accepted : Oct 25, 2022
Published : Nov 01, 2022
Archived : www.jcimcr.org
Copyright : © Schroeder LP (2022).
Citation: Schroeder LP, Manubolu VS, Bitar JA, Budoff MJ, et al. Left ventricular pseudoaneurysm and the utility of non-contrast coronary artery calcium scan in differentiating acute verse chronic bleed. J Clin Images Med Case Rep. 2022; 3(11): 2132.
Introduction
A Left Ventricular Pseudoaneurysm (LVP) forms when cardiac rupture is contained by pericardium or scar tissue [1]. Ventricular pseudoaneurysms differ from true aneurysms since they do not contain the endocardium or myocardium. LVPs can result from myocardial infarction, cardiac surgery, infection, or trauma [1]. The clinical presentation for ventricular pseudoaneurysms varies. Most notable presentations are chest pain, dyspnea, sudden cardiac arrest, congestive cardiac failure, tamponade, embolism, and syncope.
.LVP could be a potentially fatal structural condition due to its significant risk of rupture. The estimated risk of rupture for ventricular pseudoaneurysm is approximately 30-45% [2]. Due to this increased risk, the need for urgent management is crucial.
The standard imaging test used to confirm LVP when echocardiography is not diagnostic is cardiac Computed Tomography (CTA). However, this case highlights the importance of using contrast CTA in conjunction with a non-contrast study, such as a Coronary Artery Calcium (CAC) scan, where it is necessary to differentiate an acute versus chronic bleed in an LVP, which can be challenging with contrast CT alone. Differential diagnosis includes cardiac tumor and pericardial mass.
Case report
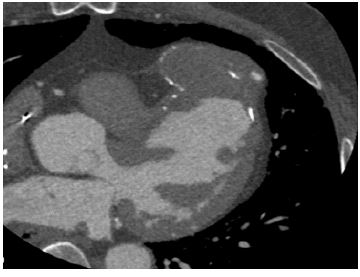
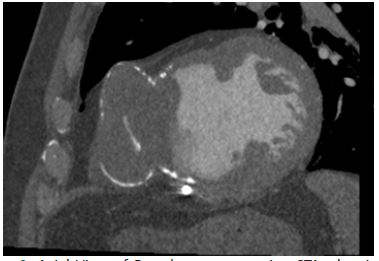
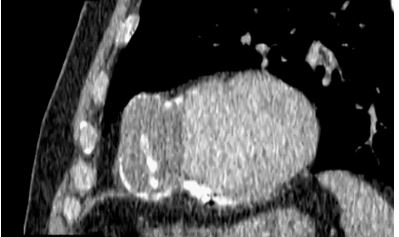
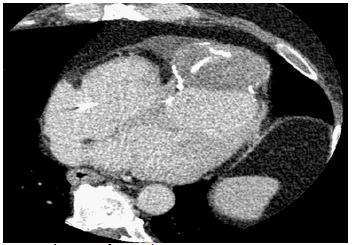
A 59-year-old male with past medical history of type 2 diabetes mellitus and coronary artery disease, on carvedilol, rosuvastatin, warfarin, and metformin, underwent CTA for evaluation of chest pain. CTA showed a pseudoaneurysm spanning 68.5 mm by 36.0 mm with several areas of High Attenuation (HU) in the aneurysm itself. This finding on CTA posed a clinical challenge: Are these high attenuation areas within the aneurysm contrast or old calcified lesions? The presence of contrast would suggest active leakage of blood into the aneurysm from the left ventricle, which may need urgent intervention in a symptomatic patient. (Figures 1-4, illustrates the pseudoaneurysm in sagittal and axial views with and without contrast).
Discussion
CTA is one of the best imaging modalities for the identification of ventricular pseudoaneurysms. However, in cases where contrast CT identifies aneurysms with high attenuation areas, it’s imperative for clinicians to know if these lesions correspond to iodinated CT contrast, an acute bleed, or chronic bleed with calcifications. Contrast CTAs can be challenging to differentiate such lesions since calcium and contrast HU overlap. Utilizing non-contrast CT along with CTA guides clinicians to differentiate such lesions. In this case, a non-contrast study (a coronary artery calcium scan) was obtained in conjunction with CTA as part of the imaging protocol. Upon evaluation of the CAC scan, there were several calcified lesions noted in the LVP indicating an old, calcified hematoma in the LVP and making the likelihood of active leakage of blood into LVP less likely. Non-contrast CAC scans are of high clinical significance in patients undergoing CTA as they can differentiate between acute bleeding or acute rupture versus calcified lesions such as old hematomas and influence further treatment plans. This particular case highlights the importance of non-contrast image calcium score in conjunction with coronary CTA in evaluation of patients with chest pain, therefore allowing the correct differentiation between an acute event vs a chronic event.
References
- Inayat F, Ghani AR, Riaz I, Ali NS, Sarwar U, Bonita R, Virk HUH, et al. Left Ventricular Pseudoaneurysm: An Overview of Diagnosis and Management. J Investig Med High Impact Case Rep. 2018; 6: 2324709618792025.
- Dachman AH, Spindola Franco H, Solomon N. Left ventricular pseudoaneurysm. Its recognition and significance. JAMA. 1981; 246: 1951-1953.