
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Delayed presentation of hypertrophic olivary degeneration
following pontine hemorrhage: Two case reports
highlighting clinical presentation, diagnostics
and multidisciplinary treatment
Shu Cheng1ⴕ; Xuan Li1ⴕ; Wei Zhang1; Lei Lei2; Mo Xian Chen3; Laakso E-Liisa4*; Jin Wen Sun1*
1Department of Rehabilitation Medicine, Wuhan University of Science and Technology affiliated Wuhan Resources & Wisco General Hospital, Wuhan, China.
2Department of Orthopaedics and Traumatology, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China.
3School of Rehabilitation, Kunming Medical University, Kunming, China.
4Mater Research, South Brisbane, Australia.
ⴕShared first author position.
*Corresponding Author : Laakso E-Liisa
Mater Research, South Brisbane, Australia.
Email: liisa.laakso@mater.uq.edu.au
Jin Wen Sun
Department of Rehabilitation Medicine, Wuhan University of Science and Technology affiliated Wuhan Resources & Wisco General Hospital, Wuhan, China.
Email: Sjwsally2005@163.com
Received : Oct 04, 2022
Accepted : Oct 26, 2022
Published : Nov 02, 2022
Archived : www.jcimcr.org
Copyright : © Laakso E-L, Jin WS (2022).
Abstract
Hypertrophic Olivary Degeneration (HOD) is a rare degenerative disease that causes hypertrophy rather than atrophy. The classical presentation of HOD is palatal myoclonus but HOD may also present with tremor, and stiffness in the extremities. In this paper, case report 1 was a man aged 46 years with HOD and Holmes tremor spreading to the head, trunk and bilateral upper and lower extremities after pontine hemorrhage. In case report 2, a 50-year-old man with HOD displayed a sense of stiffness in his left upper and lower extremities after pontine hemorrhage. Although pontine hemorrhage may cause tremor and stiffness in the late period, the development of focused imaging promotes and improves HOD diagnosis. HOD related symptoms can be partially ameliorated by the described medication and rehabilitation regimen.
Keywords: Hypertrophic olivary degeneration; Hemorrhage; Presentation; Diagnostics; Treatment.
Citation: Cheng S, Li X, Zhang W, Laakso E-L, Sun JW, et al. Delayed presentation of hypertrophic olivary degeneration following pontine hemorrhage: two casereports highlighting clinicalpresentation, diagnostics and multidisciplinary treatment. J Clin Images Med Case Rep. 2022; 3(11): 2133.
Introduction
Hypertrophic inferior Olivary Degeneration (HOD) is a trans-synaptic degenerative disorder secondary to dentate nucleus - red nucleus - inferior olivary loop (Guillain-Mollaret Triangle) lesions, mostly secondary to hemorrhage, infarction, and/or trauma of the midbrain, pons, or cerebellum [1,2]. The classical presentation of HOD is palatal myoclonus and the clinical features include dizziness, diplopia, nystagmus and ataxia. HOD may also present with Holmes Tremor (HT), mainly unilateral in the upper extremity. Tremor in the head, extremities and trunk is infrequent. Stiffness in the extremities secondary to HOD is also rarely reported. Magnetic Resonance Imaging (MRI) shows increased T2 signalling confined to the inferior olivary nucleus after stabilization of the primary lesion [3]. Due to lack of knowledge of the condition, a high rate of misdiagnosis, and ineffective treatment is presumed. The treatment of HOD to date has been mainly pharmaceutical. Rehabilitation is important, especially for patients with limb dysfunction although only one report was located regarding the rehabilitation treatment of HOD, caused by a traumatic brain injury [4]. In this paper, the clinical and imaging data of two HOD cases was analyzed and is discussed regarding clinical characteristics and rehabilitation treatment.
Case reports
Case report 1
man aged 46 years was admitted to the emergency department with sudden headache, dizziness, nausea and vomiting, followed by disturbance of consciousness for 2 hours. Non enhanced computed tomography performed on admission depicted hemorrhage on the left side of the pons, with minor involvement of the right side. The patient had a history of hypertension, type 2 diabetes mellitus, hyperlipidemia, cerebral infarction, and a long history of smoking and alcohol ingestion but denied any history of drug or food allergy.
The patient received treatment consisting of diuresis, anti-infection, hemostasis, acid inhibition, brain protection, electrolyte balance adjustment, and blood pressure control. The condition was stabilized and the patient discharged after 2 weeks of hospitalization, with right-sided hemiparesis and paraesthesia, ophthalmoplegia, and dysarthria. After discharge, the man continued to receive comprehensive rehabilitation therapy including physical and occupational therapy, acupuncture and electrical stimulation on the right extremities. The patient’s right limb activity and numbness were improved at three months assessment. He could sit and stand independently and walk several steps with minimal assistance.
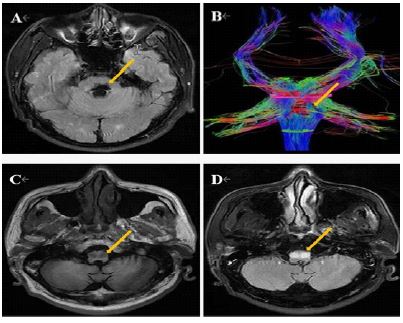
Nearly six months after the insult, he presented with involuntary tremor of the head, trunk, and bilateral upper and lower extremities exacerbated by posture and activity. Tremor was more pronounced at the upper extremities, accompanied by vertical nystagmus of both eyes and ataxia. Tremor was absent during sleep. On cranial Magnetic Resonance Imaging and Diffusion Tensor Imaging (MRI and DTI), there was prominent enlargement and T2 hyperintensity observed for both Inferior Olivary Nuclei (ION), and the left corticopontine tract was locally interrupted and sparse (Figure 1). A diagnosis of HOD was made based on clinical manifestations and the results of imaging examinations.
On admission to rehabilitation, clonazepam (0.5 g tid) was added to suppress tremors, antihypertensive (nifedipine sustained-release tablet 20 mg qd), lipid-lowering (atorvastatin calcium tablets 20 mg qd), and glucose-lowering therapies (acarbose capsules 100 mg tid). A 3 hours/day, 5 days/week rehabilitation programme was designed for one month, including mobility training, upper extremity fine motor skills training, strengthening exercises, and exercises for dysarthria, coordination and balance training. After one month of regular medication and rehabilitation, the tremor of the patient’s head, extremities and trunk was significantly reduced, and only slight nystagmus was noted. The patient showed good sitting balance (BOBATH balance from level 0 to level 1), standing with minimal assist (BOBATH balance from level 0 to nearly level 1) and improvement of Fugl-Meyer upper extremity motor score from 20 to 42 points and BADL score from 28 to 40 points between start and end of rehabilitation program. Dysarthria was also improved from 13a to 19a (Frenchay Dysarthria Assessment).
Case report 2
A 50-year-old man presented to the emergency department with sudden left hemiparesis, right facial paralysis, hypoesthesia, ataxia, ophthalmoplegia and slurred speech. The patient had a history of hypertension and hyperlipidemia, but denied any drug or food allergy history. Non enhanced computed tomography performed on admission revealed hemorrhage on the right side of the pons. After conservative treatment, the patient was discharged with severe hypoesthesia and ataxia. With continued post-discharge rehabilitation, the movement of left extremities, hypoesthesia, dysarthria, balance and ataxia were improved.
Nearly seven months after initial presentation, the patient re-presented complaining of stiffness in his left upper and lower extremities, more obvious and persistent in the upper limb, persistent and aggravated by activity. MRI and DTI examination showed enlarged and remarkable T2 hyperintensity in bilateral ION, and the right corticopontine tract was locally interrupted and sparse (Figure 2). Combined with the MRI findings and symptoms, a diagnosis of HOD was made.
The patient was prescribed oral antihypertensive (fosinopril tablets 10 mg qd), lipid-lowering drug (atorvastatin calcium tablets 20 mg qd), and relief of the sense of stiffness (Gabapentin 0.3 g tid, dopamine 0.25 g tid, clonazepam 0.5 g tid, baclofen 10 mg tid). A 3 hours/day, 5 days/week rehabilitation plan was scheduled for one month, including stretching of the left upper and lower extremities, scapula and pelvis stability training, sit-to-stand transfer activity, knee control and walking training, upper extremity fine motor skills training, coordination training, and Mendelssohn technique. Acupuncture treatment in left extremities and right face and scalp was used for dredging the meridians and circulation. After one month of regular medication and rehabilitation, the patient had no improvement in the feeling of stiffness of his left extremities, but improvement of Fugl-Meyer upper extremity motor score from 40 to 50 points and BADL score from 70 to 75 points between start and end of rehabilitation program. He could sit independently (BOBATH balance from level 1 to nearly level 2), and stand for a short time (BOBATH balance from level 0 to nearly level 1), and his speech function was improved from 19a to 24a (Frenchay Dysarthria Assessment).
Discussion
HOD is a transsynaptic degeneration of neurons caused by changes in the connections among neurons in the cerebellar dentate nucleus, midbrain red nucleus and inferior olivary nucleus of medulla oblongata. Nerve fibers from the dentate nucleus pass through the superior foot of the cerebellum to the contralateral red nucleus and interact with the cerebellar arm along the pathway. Nerve fibers from the red nucleus descend through the central tegmental tract to the inferior olivary nucleus, and nerve fibers from the inferior olivary nucleus pass through the inferior foot of the cerebellum to the contra lateral dentate nucleus. The loop was first described in 1931 by Guillain and Mollaret, also known as the Guillain-Mollaret anatomical Triangle (GMT) [5]. When the lesion is located in the red nucleus or central tegmental tract, it often results in ipsilateral hypertrophy of the olivary nucleus. In contrast, if the dentate nucleus or the superior foot of the cerebellum is insulted, degeneration would happen in the contralateral ION. Bilateral hypertrophic inferior olivary degeneration is usually caused by simultaneous damage to the red nucleus or central tegmental tract, as well as to the dentate nucleus or the superior foot of cerebellum. Destruction of the inferior olivary efferent fibers will not cause HOD [6]. In case one, the hemorrhagic lesion involved the bilateral tegmental tract of the pons, and in case two, the lesion involved the ipsilateral tegmental tract of the pons and the upper cerebellar foot. MRI of both patients showed bilateral hypertrophic inferior olivary degeneration.
The pathological evolution of HOD can be divided into 6 periods [7,8]: stage 1: At the early stage of the disease, there is no abnormality in the ION; stage 2: Degeneration of the ION, pathological hypertrophy with no glial proliferation under microscopy after approximately 3 weeks; stage 3: Hypertrophy of the ION due to neuronal and astrocyte proliferation after approximately 6 months; stage 4: Significant hypertrophy and enlargement of the ION; stage 5: Pseudohypertrophy of the ION (disintegration of neurons and astrocytes), remaining for 3–4 years; and stage 6: ION atrophy due to neuronal loss after a few years.
The clinical manifestations of HOD mainly include palatal myoclonus, nystagmus, ataxia, limb clonus or severe tremor, among which palatal muscle tremor is the characteristic manifestation of the disease [9,10] however, not all patients with HOD show palatal myoclonus. Two patients reported by Terao et al [11] presented with limb clonus and nystagmus, but no palatal myoclonus. In addition to the primary disease, the clinical manifestations of case one mainly included tremor in the Head, Trunk and Extremities (HT) and nystagmus, without palatal myoclonus. The presentation of HOD with HT spreading to the lower extremities and trunk is very rare [12,13]. HT is characterized by tremor that is induced by posture and intention and disappears during sleep [14]. It generally appears in one upper extremity [15]. The mechanism of tremor may be related to damage of the GMT when the cerebellum amplifies low-frequency oscillations [16,17]. The mechanism of ataxia is related to the effect of ION degeneration on cerebellar function. The inferior olivary degeneration leads to the reduction of crawling fibers, progressive degeneration of purkinje cells, and the gradual release of inhibition of deep cerebellar nucleus cells, resulting in ataxia [18,19].
The diagnosis of HOD depends mainly on head MRI and DTI. On MRI, the ION show increased volume, localized high-signal nodules on T2‑weighted images, and equal or low signal on T1WI, with no enhanced signal. The lesion can be seen as early as 1 month after onset on T2WI, most clearly at 8 months, still visible at 18 months, and disintegrated 3-4 years later [20,21]. DTI, as a new functional MRI technology, has been preliminarily applied in clinical work of central nervous system diseases such as stroke, brain tumor, neurodegenerative disease, demyelinating disease and mental disease by three-dimensional reconstruction of white matter fiber tracts and analysis of their integrity to assess the severity of disease [22]. HOD is distinguished primarily from T2 hyperintensity on MRI of the ION. Infarction, tumor, demyelination, infection, or inflammatory disease of the medulla oblongata may also present. However, most of these can be identified by clinical and supplementary examination. The secondary T2WI hyperintensity of distant sites, is different from other disease manifestations. However, imaging examination has a lag and is not suitable for early diagnosis of disease. Mutations in POLG and SURF1 genes cause mitochondrial production and metabolism disorders, which significantly increase the risk of HOD [23]. Therefore, genetic testing of patients after brain stem and cerebellar injury can help predict HOD.
HOD is a self-limiting disease in which the olivary nucleus gradually atrophies and the symptoms are gradually relieved without any targeted treatment. The drugs used to treat tremor include clonazepam, carbamazepine, levodopa, artane, tiapride and propranolol. Most drugs relieve but may not completely control tremor. Severe tremor may also be amenable to deep brain stimulation [24]. In case one, after oral administration of clonazepam during hospitalization, nystagmus almost resolved, trunk and extremity tremor was significantly reduced and independent sitting and standing position were restored. To our knowledge, there has been no literature reporting the treatment of secondary extremity stiffness. Case 2 received oral gabapentin, levodopa, clonazepam and baclofen successively, but the treatment effect was suboptimal. Since clinical manifestations of HOD often overlap with primary manifestations, sensory input, core trunk control, balance and ataxia training are mostly performed in rehabilitation for common clinical manifestations [21]. Sensory disorders, balance disorders and ataxia were the root causes of motor control disorders in the two described cases, and also created difficulties in rehabilitation.
Sensory disorders can be divided into superficial sensory disturbance, proprioceptive and complex sensory disorders. Clinically, mecobalamin, nerve growth factor, gabapentin, pregabalin, duloxetine and amitriptyline are often prescribed. Superficial sensory rehabilitation training is carried out through physical therapy and occupational therapy such as Rood therapy, needle-tip stimulation, alternating hot and cold stimulation, rapid brush and other methods, following the principle of eye closing - eye opening - eye closing while stimulating the skin. In proprioceptive sensory disorders, joint position and motion influence motor function rehabilitation. In the early stage in our cases, we mainly carried out good limb position, joint compression and proprioceptive neuromuscular facilitation to promote sensory input to central and peripheral nervous systems. Subsequently, proprioception can be enhanced through balance training and visual biofeedback training [25]. Motion control training is used to improve posture disorders caused by proprioception and muscle tone abnormalities [26]. In addition, traditional Chinese medicine and acupuncture also have an effect on the rehabilitation of sensory disorders [27,28] and include flavored astragalus cassia twig decoction, angelica nourishing blood decoction, and acupuncture (mainly in the heart meridian, pericardium meridian, and surface projection of posterior central gyrus). The two cases had obvious sensory disturbance and proprioceptive hypoaesthesia which were improved after combined rehabilitation and drug treatment.
As well as proprioceptive dysfunction in the two cases, impaired visual and vestibular input contributed to balance dysfunction. Due to its importance in daily life, balance and coordination re-training (to correct procedural sensory information) was a critical part of rehabilitation following the sequence of motor development from sitting, to standing to walking training, rather than simple muscle strength training and reflex activity [29,30], which was considered vital in optimizing outcomes. Through staged training, balance, coordination functions and the ability of daily living activities was significantly improved.
Conclusion
The reported cases show neurological deterioration secondary to pons hemorrhage with interval development of bilateral HOD during recovery. Comprehensive rehabilitation along with drug therapy relieved tremor and ataxia and improved daily living ability. The effectiveness of sensory, balance and coordination rehabilitation in HOD patients needs to be considered by clinicians in complex presentations such as the ones described here. However, many mechanisms of the disease remain unresolved thus a gold standard of treatment remains unsolved. Greater research effort is required to understand HOD and develop effective therapies.
Declarations
Ethics approval and consent to participate: This study was approved by the Ethics Committee of China Resources & WISCO General Hospital. Written informed consent for anonymous publication of case details and pictures was obtained from each patient.
Acknowledgments: Thanks to all the reviewers and editors for their opinions and suggestions. This work was supported by Hubei Provincial Health Commission Joint Fund Project (number WJ2019H199).
Conflicts of interest: The authors report no conflicts of interest in this work.
References
- Wein S, Yan B, Gaillard F. Hypertrophic olivary degeneration secondary to pontine haemorrhage. J Clin Neurosci. 2015; 22: 1213-1214.
- Konno T, Broderick DF, Tacik P, Caviness JN, Wszolek ZK, et al. Hypertrophic olivary degeneration: A clinico-radiologic study. Parkinsonism & related disorders. 2016; 28: 36-40.
- Wang YL, Gao Y, He PP, Yin JN, Dong RF, et al. A meta-analysis of case studies and clinical characteristics of hypertrophic olivary degeneration secondary to brainstem infarction. Journal of integrative neuroscience. 2020; 19: 507-511.
- Zhou J, Liu Y, Ali Shah SZ. Hypertrophic olivary degeneration following cerebral trauma managed with rehabilitation - A case report. J Pak Med Assoc. 2021; 71: 1252-1254.
- Kitajima M, Korogi Y, Shimomura O, Sakamoto Y, Hirai T, et al. Hypertrophic olivary degeneration: MR imaging and pathologic findings. Radiology. 1994; 192: 539-543.
- Gatlin JL, Wineman R, Schlakman B, Buciuc R, Khan M, et al. Hypertrophic olivary degeneration after resection of a pontine cavernous malformation: A case report. Journal of radiology case reports. 2011; 5: 24-29.
- Pandey P, Westbroek EM, Gooderham PA, Steinberg GK. Cavernous malformation of brainstem, thalamus, and basal ganglia: A series of 176 patients. Neurosurgery. 2013; 72: 573-589; discussion 88-89.
- Shinohara Y, Kinoshita T, Kinoshita F, Kaminou T, Watanabe T, et al. Hypertrophic olivary degeneration after surgical resection of brain tumors. Acta radiologica (Stockholm, Sweden: 1987). 2013; 54: 462-466.
- Lim CC, Lim SA. Images in clinical medicine. Pendular nystagmus and palatomyoclonus from hypertrophic olivary degeneration. The New England journal of medicine. 2009; 360: e12.
- Bruno MK, Wooten GF. Hypertrophic olivary degeneration. Archives of neurology. 2012; 69: 274-275.
- Terao S, Sobue G, Takahashi M, Osano Y, Shimada N, et al. [Chronological changes in MR imaging of inferior olivary pseudohypertrophy-report of two cases]. No to shinkei = Brain and nerve. 1994; 46: 1184-1189.
- Kim JS, Park JW, Kim YI, Han SJ, Kim HT, et al. Tremors associated with an inferior olivary lesion that developed after a pontine hemorrhage. Movement disorders: Official journal of the Movement Disorder Society. 2006; 21: 1539-1540.
- Menéndez DF, Cury RG, Barbosa ER, Teixeira MJ, Fonoff ET, et al. Hypertrophic olivary degeneration and holmes’ tremor secondary to bleeding of cavernous malformation in the midbrain. Tremor and other hyperkinetic movements (New York, NY). 2014; 4: 264.
- Kim MK, Cho BM, Park SH, Yoon DY. Holmes’ tremor associated with bilateral hypertrophic olivary degeneration following brain stem hemorrhage: A case report. Journal of cerebrovascular and endovascular neurosurgery. 2014; 16: 299-302.
- Choi SM. Movement Disorders Following Cerebrovascular Lesions in Cerebellar Circuits. Journal of movement disorders. 2016; 9: 80-88.
- Zhang X, Santaniello S. Role of cerebellar GABAergic dysfunctions in the origins of essential tremor. Proceedings of the National Academy of Sciences of the United States of America. 2019; 116: 13592-13601.
- Wright GC, Brown R, Grayton H, Livingston JH, Park SM, et al. Clinical and radiological characterization of novel FIG4-related combined system disease with neuropathy. Clinical genetics. 2020; 98: 147-154.
- Nishie M, Yoshida Y, Hirata Y, Matsunaga M. Generation of symptomatic palatal tremor is not correlated with inferior olivary hypertrophy. Brain : a journal of neurology. 2002; 125: 1348-1357.
- Shaikh AG, Hong S, Liao K, Tian J, Solomon D, et al. Oculopalatal tremor explained by a model of inferior olivary hypertrophy and cerebellar plasticity. Brain: A journal of neurology. 2010; 133: 923-940.
- Goyal M, Versnick E, Tuite P, Cyr JS, Kucharczyk W, et al. Hypertrophic olivary degeneration: Metaanalysis of the temporal evolution of MR findings. AJNR American journal of neuroradiology. 2000; 21: 1073-1077.
- Blanco Ulla M, López Carballeira A, Pumar Cebreiro JM. Magnetic resonance imaging of hypertrophic olivary degeneration. Radiologia. 2015; 57: 505-511.
- Schaller-Paule MA, Steidl E, Shrestha M, Deichmann R, Steinmetz H, et al. Multicenter Prospective Analysis of Hypertrophic Olivary Degeneration Following Infratentorial Stroke (HOD-IS): Evaluation of Disease Epidemiology, Clinical Presentation, and MR-Imaging Aspects. Frontiers in neurology. 2021; 12: 675123.
- Kinghorn KJ, Kaliakatsos M, Blakely EL, Taylor RW, Rich P, Clarke A, et al. Hypertrophic olivary degeneration on magnetic resonance imaging in mitochondrial syndromes associated with POLG and SURF1 mutations. Journal of neurology. 2013; 260: 3-9.
- Sabat S, Mannering N, Agarwal A. Hypertrophic olivary degeneration: Case series and review of literature. Journal of the neurological sciences. 2016; 370: 180-186.
- Gorst T, Rogers A, Morrison SC, Cramp M, Paton J, Freeman J, et al. The prevalence, distribution, and functional importance of lower limb somatosensory impairments in chronic stroke survivors: A cross sectional observational study. Disability and rehabilitation. 2019; 41: 2443-2450.
- Hugues A, Di Marco J, Ribault S, Ardaillon H, Janiaud P, et al. Limited evidence of physical therapy on balance after stroke: A systematic review and meta-analysis. PloS one. 2019; 14: e0221700.
- Li L, Pan J, Chen C. [Electroacupuncture on the heart meridian and pericardium meridian acupoints for 29 cases of sensory disturbance after thalamic stroke]. Zhongguo zhen jiu = Chinese acupuncture & moxibustion. 2016; 36: 102.
- Donnelly SC. Traditional Chinese medicine treatment post-stroke and a significant reduction in presentation to healthcare providers. QJM: monthly journal of the Association of Physicians. 2019; 112: 397.
- Toosizadeh N, Mohler J, Armstrong DG, Talal TK, Najafi B, et al. The influence of diabetic peripheral neuropathy on local postural muscle and central sensory feedback balance control. PloS one. 2015; 10: e0135255.
- Schröder J, van Criekinge T, Embrechts E, Celis X, Van Schuppen J, et al. Combining the benefits of tele-rehabilitation and virtual reality-based balance training: A systematic review on feasibility and effectiveness. Disability and rehabilitation Assistive technology. 2019; 14: 2-11.