
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Recurrent vulval angiomyofibroblastoma; An unusual benign
mesenchymal tumour, misdiagnosed
Hasina Sadiq1*; Irum Sohail2; Marium Riaz3; Shafaq Fatima3; Mahrukh Fatima Zaidi3
1Senior Registrar, Obstetrics and Gynecology Department, Shifa College of medicine, Islamabad, Pakistan.
2Professor of Obstetrics & Gynaecology, KRL Hospital, Islamabad, Pakistan.
3Post graduate trainees, Obstetrics and Gynecology Department, KRL Hospital, Islamabad, Pakistan.
*Corresponding Author : Dr Hasina Sadiq
Senior Registrar, Obstetrics and Gynecology Department, Shifa College of medicine, Islamabad, Pakistan.
Email: humbleschlr3@gmail.com
Received : Oct 03, 2022
Accepted : Oct 26, 2022
Published : Nov 02, 2022
Archived : www.jcimcr.org
Copyright : © Sadiq H (2022).
Abstract
We present a case report of a middle aged post menopausal female with a huge pelvic mass for last 15 years that was previously misdiagnosed as chronic dermatitis. Based on its uncanny appearance, it was decided to do complete excision of the vulval mass to rule out any soft tissue tumour. The histopathology came out to be a rare benign lesion i.e, angiomyofibroblastoma with the immunohistochemistry report favouring the diagnosis. The patient after complete excision is under routine follow up and survelliance and is recurrence free to date.
Keywords: Angiomyofibroblastoma; Vulva neoplasm; Mesenchymal tumour.
Citation: Sadiq H, Sohail I, Riaz M, Fatima S, Zaidi MF, et al. Recurrent vulval angiomyofibroblastoma; An unusual benign mesenchymal tumour, misdiagnosed. J Clin Images Med Case Rep. 2022; 3(11): 2134.
Introduction
Mesenchymal tumours of the vulva are a rare entity characterized by two main types i.e, benign angiomyofibroblastoma, and aggressive angiomyxoma. Both of them are difficult to diagnose and differentiate due to the rarity and overlapping gross morphological characteristics, histopathology, and immunohistochemistry features [1,2]. Angiomyofibroblastoma is the benign variant characterized by myofibroblastic cells and stromal cell differentiation and proliferation [3]. The tumor can occur in both males and females. Although, the tumour is rare in males the predominance site is the inguinoscrotal region, while the perineal region and vulva are common sites in females. The least common site in females is the uterine cervix being reported in 5 case reports to date, fallopian tube, and rarely urethra [3,4].
Due to its uncommon presentation, other benign conditions considered in the differential diagnosis are leiomyoma, fibroma, lipoma, and myxoma. While vulval and vaginal cyst and abscesses like bartholin cyst, gartner duct cyst, and nuck duct cyst also cannot be ignored [5]. It is prudent to differentiate and correctly diagnose the angiomyofibroblastoma from its aggressive varivariant. The former one is well-circumscribed masses with regular borders with high vascularity and cellularity. But the malignant variant is invasive and infiltrates into the deeper tissues [5]. The treatment of the benign variant is wide local excision with lower recurrence rates after complete resection. But the angiomyxoma required deeper resection followed by radiotherapy, depending upon the depth of involvement [1].
In this article, we reported a patient presented in March 2022 at the gynecological outpatient department of KRL hospital Islamabad with a vulvar mass diagnosed later on as angiomyofibroblastoma on histopathological examination.
Case presentation
A 57-year-old female presented to the outpatient department of KRL Hospital with the presenting complaint of a large pedunculated vulval mass. She has been married for 40 years in a consanguineous marriage with early teen marriage at 17 years. Regarding her parity, she is para 6+0 with all spontaneous vaginal deliveries and last childbirth 32 years back. She was diagnosed case of hepatitis C since last 15 years followed by a complete treatment and PCR negative for the last 5 years. Apart from this, patient was a known case of type II Diabetes mellitus and was on injectable insulin. Furthermore, she was recently diagnosed with essential hypertension and was compliant with the oral antihypertensive drug. Her surgical history was significant for a total abdominal hysterectomy that was done 25 years back due to chronic PID resulting in a surgical menopause.
She presented with a complaint of recurrent vulvar growth, which initially appeared 15 years back with the complaints of chronic vulvar itching. The vulvar growth was painless. She was given multiple topical ointments by a dermatologist and gynecologist including topical steroid cream, fusidic cream, and bacitracin cream. The vulvar growth biopsies were done 5 times according to the patient and the latest report done in 2014 was consistent with chronic dermatitis, negative for malignancy and acid-fast bacilli. She was reassured and topical ointments were given. But she had persistent complaints of chronic itching over the mons pubis and on labia majora with a large vulvar re-growth. This was now affecting her quality of life up to the extent that the mass was associated with hindrance during movement and also her sexual life. Later on, the mass became tender due to its huge size so she visited the outpatient department. Her history was negative for any history of genital or skin warts, chronic skin lesion anywhere on the body or vaginal dischargeand drug allergies.She was morbidly obese with a BMI of 41 kg/m2, vitally stable, and cooperative during the examination. Abdominal examination was significant for a large paraumbilical hernia. While the rest of the examination was unremarkable. On local examination, there was a large, well-circumscribed, non-tender, firm mass hanging down from the mons pubis and extending up to the left labia majora. The size of the mass was 10 x 8 cm. The surface of the mass was uneven with dark brown patches and polypoid growths over the surface mimicking the small wart-like lesions (Figure 1). Vaginal examination, digital rectal examination followed by proctoscopy was unremarkable. Differential diagnoses based on appearance were lipoma, condylomata and vulval intraepithelial neoplasia.

Dermatologist was also taken on board before planning to do the complete excision of the mass. During the surgery the findings were excision of the gross cauliflower-like growth, yellow color serous fluid oozed out while excising lesion. The size of the mass was 8 x 8 x 2 cm. The cut surface was tan white and yellow homogenously with small spaces filled with yellow serous fluid.The surgical margins were clear. Post-operative recovery of the patient was smooth.
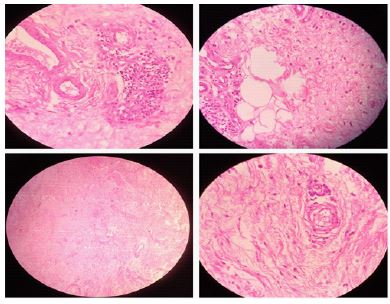
Microscopically, the tissue was lined by the stratified squamous epithelium. Subepithelial tissue shows a mesenchymal tumour composed of fascicles of spindle cells that have abundant eosinophilic cytoplasm and elongated nuclei with no atypia. This tumour is showing hypo and hypercellular areas. Stroma is edematous and myxoid with scattered cells are seen. Tumour is reaching up to the deep margin. The features were in the favour of the angiomyofibroblastoma. Immunohistochemistry revealed that the tumour is positive for desmin, vimentin, faint positive for estrogen and progesterone while negative for smooth muscle actin. Histopathology features are shown in Figure 2.
She was called for follow-up, and the wound was healthy. Considering complete surgical excision, it was decided to call her on regular follow-up visits and a telephonic contact number was taken from the patient. Counseling and debriefing of the attendants were done. Up till now no recurrence was noted.
Discussion
This tumour was first described in the literature by Fletcher CD, et al. in 1992 as a painless and slowly growing mass with no recurrence. This was a case series of 10 patients with angiomyofibroblastoma [6]. The average age of females with angiomyofibroblastoma is between 30 to 50 years [1,3]. The age of our patient was 57 years. However, it can occur in young females as well reported in the literature by Angraenni TD, et al. in which a young female of 22 years, nulliparous presented with a painless vulvar mass slowly growing over a period of 10 years that was treated by wide excision [1]. The patient was followed over a period of 2 years and no recurrence was noted.
The size of the tumour is variable ranging from less than 5 cm for vulvar angiomyofibroblastoma to more than 6 cm for cervical tumours and up to 37 cm in some studies [1,3,4]. Macroscopically the tumour has been described as a myxoid homogenous mass with well-circumscribed borders and margins in the majority of studies and histologically by areas of hypercellularity and hypocellularity with internal vascularity. These features were present in our patient as well [5]. The treatment of such vulvar lesions is total excision with no recurrence noted. This surgical treatment has been suggested in a majority of literature.
Other pathological entities to consider before reaching the final diagnosis are other vulval lesions like bartholin gland cyst, vulvar abscess, lipoma, sarcoma, myxoma, vulvar hypertrophy with lymphedema and hemangioma. But the important thing is to differentiate this benign mesenchymal lesion from the aggressive variant; angiomyxoma. Angiomyxomas are deeper infiltrating lesions of larger sizes in a majority of cases. They are aggressive due to their tendency to metastasize locally adjacent paravaginal and pararectal tissues. They require extensive surgical approaches with postoperative radiotherapy or hormonal therapy due to a greater risk of local recurrences up to 72% [7]. Previously the immunohistochemistry markers were used to distinguish between the two entities and it was believed that mainly desmin, vimentin, estrogens and progesterone receptors are affirmative for the angiomyofibroblastomaonly. But this was refuted later on as they were found to be positive in some of the cases with angiomyxoma [8].
In literature other benign variants have also been mentioned. Kunnath NP, et al. described a case of cellular angiofibroma of vulva in a post menopausal female of 52 years. This variant appeared as asymptomatic multiple polypoidal masses in the vulval region. Histologically, spindle cells were seen with a differentiating feature of hyalinized thick walled vasculature. Treatment and immunohistochemistry staining characteristics were same in both of the lesions [9].
In one of the case report from Sudan, there was a finding of moderate anemia but considered a coincidental finding in the patient as this was not found in other case reports. Anemia is common in Africa in various forms such as iron deficiency anemia, sickle cell anemia, and variants of thalassemia. Similarly, in that patient history of female genital mutilation type II was present. But no correlation was confirmed [5]. No such factors were found in our patient.
Conclusion
Vulva neoplasms either benign or malignant are rare. But the patients with a suspicious looking vulval mass should undergo complete excision followed by histopathology and immunohistochemistry testing to confirm the diagnosis. Benign lesions have lower recurrence rate but the malignant lesions will need further adjuvant therapies. Hence, the exact diagnosis will lead to better treatment of the patient.
References
- Anggraeni TD, Nuranna L, Luthfiyanto M, Siregar NC, Hellyanti T, Siregar TP, et al. Rare case of huge vulvar angiomyofibroblastoma in a young female. Gynecologic oncology reports. 2021; 36: 100751.
- Kulkarni AR, Tinmaswala MA, Shetkar SV, Kondekar S. Angiomyofibroblastoma: Imaging and histopathology of a rare benign mesenchymal tumor. Tropical Journal of Obstetrics and Gynaecology. 2019; 36: 308-311.
- Büyüktalanci DÖ, Yiğit S, Altindağ SD, Aydoğmuş H, Gençdal S, et al. Angiomyofibroblastoma of the uterine cervix in a patient with triple negative breast cancer: A case report. Anatolian Current Medical Journal. 3: 181-184.
- Buitrago SM, Caicedo CM, Puentes LO. 609 Angiomyofibroblastoma vulvar: Case report and literature review. International Journal of Gynecologic Cancer. 2020; 30.
- Birge O, Merdin A, Ozbey EG, Arslan D. Large pedunculated angiomyofibroblastoma of the vulva with concomitant anemia: A case report and mini review of the literature. Clinical and Experimental Obstetrics & Gynecology. 2021; 43: 914-916.
- Fletcher CD, Tsang WY, Fisher C, Lee KC CJ. Angiomyofibroblastoma of the vulva. A benign neoplasm distinct from aggressive angiomyxoma. Am J Surg Pathol. 1992; 16: 373–382.
- Goyal LD, Garg P, Badyal R, Bhalla S. Aggressive (deep) angiomyxoma of the vulva: A case report. Journal of Medical Case Reports. 2022; 16: 1-4.
- Qiu P, Wang Z, Li Y, Cui G. Giant pelvic angiomyofibroblastoma: Case report and literature review. Diagnostic Pathology. 2014; 9: 1-5.
- Kunnath NP, Nanda S, Mohapatra J. Multiple Angiofibromas of the Vulva in Postmenopause. Indian Journal of Gynecologic Oncology. 2022; 20: 1-3.