
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Removal of a pellet from the left ventricle
trabeculae: A case report
Abdolhamid Bagheri; Mohamad Khani; Tooba Akbari*
Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Tooba Akbari
Postal address: Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Tel: +98 21 22083106;
Email: Tbaakbari@gmail.com
Received : Oct 06, 2022
Accepted : Oct 26, 2022
Published : Nov 02, 2022
Archived : www.jcimcr.org
Copyright : © Akbari T (2022).
Abstract
Cardiac gunshot wounds, despite being rare, have a high mortality rate, and their proper management and prompt decision-making are critical.Here we present a case of cardiac gunshot woundin a young male who was shot at close range in the left shoulder from behind. The patient admitted at hospital with stable vital signs, but after a while, shortness of breath was begun and pneumothorax was diagnosed. Due to the instability of the pellet which localized in the LV using echocardiography, surgical excision of the pellet was planned. Patient was discharged two week the pellet removal with no complications.
Keywords: Cardiac wounds; Pellet; Gunshot management; Surgical procedures; Left ventricle.
Citation: Bagheri A, Khani M, Akbari T. Removal of apellet from the left ventricle trabeculae: A case report. J Clin Images Med Case Rep. 2022; 3(11): 2135.
Introduction
Cardiac wounds due to gunshots are usually rare and mostly lethal. Management of such wounds is very difficult, and there is a short period of time to keep patients alive [1]. Although it is difficult to calculate the survival rate of patients, but different studies estimate the survival rate between 3% to 84% [2]. The gold standard procedure for managing such patients globally is surgical, which of course depends on the patient’s clinical condition and hemodynamic stability of the bullet [3]. The mechanism of trauma, clinical conditions in hospitalization and the presence of lesions in multiple heart chambers are the most important variables for determining the outcome in these patients [2,4]. It is crucial to assess the cardiac injury extent, bullet trajectory, localizing and extraction of bullet immediately, which routinely performed using Computed tomography, transthoracic echocardiography, and transesophageal echocardiography [5].
We present the case of a young male who was shot at close range in the left shoulder from behind. In this case report, we pointed out the successful extraction of a pellet at the left ventricle trabeculae.
Case report
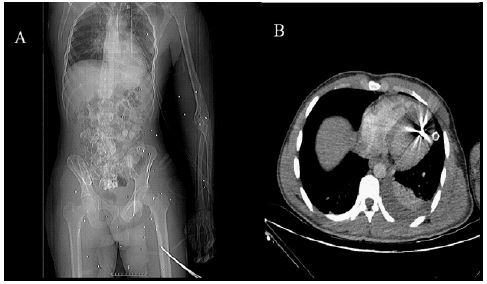
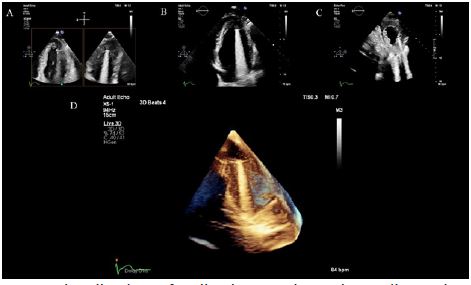
An 18-year-old man with multiple pellet injuries in the back who was hit with a hunting weapon from a distance of 5 meters, came to the hospital. The patient had no initial symptoms and was admitted to the hospital with stable vital signs, and without chest pain and shortness of breath. The patient was conscious at arrival with a Glasgow Coma Score of 15, a blood pressure of 120/70 mmHg, a body temperature of 36.8oC, respiratory rate of 20/minute, an oxygen saturation of 99% on room air,and a heart rate of 90 beats per minute. Upon arrival, Electrocardiogram (ECG), chest X-ray and Computed Tomography (CT) were performed. The patient’s ECG was normal and a pellet was observed in the CT examination (Figure 1). After 1 hour, symptoms of shortness of breath and pneumothorax appeared. Echocardiography was immediately performed on the patient and the pellet was observed in the Left Ventricular (LV) trabeculae (Figure 2). Echocardiography evaluation showed that the pellet entered the heart, but it was unstable and it was possible to fall inside the heart. Despite the expectation, the patient did not have Pulmonary Embolism (PE), but had a history of PSVT and PVC.
Due to the instability of the pellet in the LV and the risk of systemic embolization, the decision was made for surgical exploration. The patient was admitted to the cardiac surgery ward for extraction of the pellet. Since, the entry wound was found in posterior of LV, pellet was removed from trabeculae and then the wound was repaired (Figure 3).
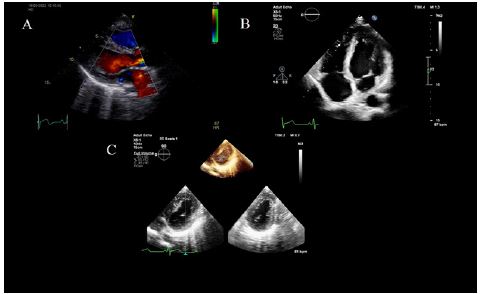
The patient had complete recovery from surgery and didn’t need ventilatory or dynamic support during its course. Echocardiography performed after recovery showed normal LV function was and there was no PE (Figure 4). Finally, the patient was discharged 2 weeks after surgery with a normal mitral valve, cardiac function and muscle structure, and a good general condition. Echocardiography after surgery also showed the proper function and structure of the heart.

Discussion
Hemodynamic compromise of the patient determines the decision for management of cardiac gunshot wounds. If the patient faced hemorrhagic shock due to blood loss or in the presence of pericardial tamponade, surgical intervention is obligatory. But patients with stable hemodynamic must be evaluated carefully. In such conditions, a comprehensive physical examination, chest X-ray, and chest CT must be performed to monitor patient’s vital signs and to evaluate the possible damage of the vital organs and bullet localization. Despite this, the management of gunshot wounds remains controversial [6-8].
We presented the case of a stable young male, who was shot at close range from behind. He arrived at hospital with stable vital signs. Shortly after admission symptoms of shortness of breath and pneumothorax appeared and a pellet was localized in the LV.
Bullets or pellets may be found free in different heat chambers, in the pericardial space, or penetrated in the myocardium.It had been reported that combined use of 2D-echocardiography and contrast-enhanced CT is the suitable approach to localize the bullet, and to evaluate the extent of injury [9]. Besides, Hashimi and colleagues stated the superiority of transesophageal echocardiography compared to transthoracic echocardiography for the localization and characterization of intracardiac pellets [10]. Choosing the right imaging system and localization of the pellet is crucial in such cases since surgeon had a short period of time to made a decision [11].
The early clinical feature of cardiac gunshots include tamponade, hemorrhage, valvular dysfunction, and intracardiac shunts. Also, there are several late features including pulmonary arteries embolism, endocarditis, dysrhythmia, pericarditis, stroke, erosion into coronary vessels, lead toxicity, and cardiac neurosis [12].
Several indications had been established for surgical excision of bullet. Proximity to a vital structure, entry into heart after contamination, unstable bullet on imaging, dysrhythmia, intracardiac shunt, and hemodynamic valvular compromise are hard indications. Besides several soft indications had been mentioned in literatures [13].
Stable and asymptomatic patients with intramyocardial or pericardial gunshots preferred to be managed non-operatively. On the other hand, bullets found in heart chambers, bullets with valvular wounds or those partially embedded in the myocardium should be excised surgically. To making decision for surgical intervention in symptomatic patients with cardiac gunshot injuries, careful observation and imaging by different methodologies must be considered. To prevent cardiac tamponade in cases that the patient has pericardial effusion, there may be a need for pericardiocentesis and/or cardiac surgery [14,15].
The majority of the cardiac gunshot wounds were removed surgically [16]. Generally, bullets retained the chambers had a potential for embolization should be removed through surgical exploration [17].
Conclusion
Cardiac gunshot wounds are rare, but their proper management is essential. Each patient must be evaluated individually and there is no universal protocol of management. Correct use of imaging and assessment of the patient’s condition as soon as possible are critical. Here we report a case of cardiac gunshot, in which the pellet was removed from the patient’s LV with a timely decision based on the patient’s condition and imaging.
Conflict of interest: Authors had no conflict of interest.
References
- Kaya A, Caliskan E, Tatlisu MA, Hayiroglu MI, Tekessin AI, Cakilli Y, et al. A Retained Bullet in Pericardial Sac: Penetrating Gunshot Injury of the Heart. Case Rep Cardiol. 2016; 2016: 2427681.
- Kang N, Hsee L, Rizoli S, Alison P. Penetrating cardiac injury: overcoming the limits set by Nature. Injury. 2009; 40: 919-927.
- Daskalaki D, Hakmi H, Stright A, Mitzman B, Mair ER, Joseph DK, et al. Bullet embolization to the heart: A rare and confounding penetrating cardiac injury case report. Int J Surg Case Rep. 2020; 73: 35-38.
- Volpe MA, Paredes JEM, Redigolo LC, Sanchez ISM, Lanichek F, et al. Heart Injury with Projectile Lodged Inside the Heart. Braz J Cardiovasc Surg. 2018; 33: 303-305.
- Brathwaite CE, Weiss RL, Baldino WA, Hoganson N, Ross SE, et al. Multichamber gunshot wounds of the heart. The utility of transesophageal echocardiography. Chest. 1992; 101: 287-288.
- Hassett A, Moran J, Sabiston DC, Kisslo J. Utility of echocardiography in the management of patients with penetrating missile wounds of the heart. J Am Coll Cardiol. 1986; 7: 1151-1156.
- Robison RJ, Brown JW, Caldwell R, Stone KS, King H, et al. Management of asymptomatic intracardiac missiles using echocardiography. The Journal of trauma. 1988; 28: 1402-1403.
- Symbas PN, Vlasis Hale SE, Picone AL, Hatcher CR, Jr. Missiles in the heart. Ann Thorac Surg. 1989; 48: 192-194.
- Alakhfash AA, Alqwaee A, Almesned A. Percutaneous removal of air-bullet gunshot: Case report and literature review. Egypt Heart J. 2020; 72: 21.
- Kaljusto ML, Skaga NO, Pillgram Larsen J, Tonnessen T. Survival predictor for penetrating cardiac injury; a 10-year consecutive cohort from a scandinavian trauma center. Scand J Trauma Resusc Emerg Med. 2015; 23: 41.
- Restrepo CS, Gutierrez FR, Marmol-Velez JA, Ocazionez D, Martinez-Jimenez S. Imaging patients with cardiac trauma. Radiographics. 2012; 32: 633-649.
- Symbas PN, Picone AL, Hatcher CR, Vlasis Hale SE. Cardiac missiles. A review of the literature and personal experience. Ann Surg. 1990; 211: 639-647.
- Lundy JB, Johnson EK, Seery JM, Pham T, Frizzi JD, Chasen AB, et al. Conservative management of retained cardiac missiles: Case report and literature review. J Surg Educ. 2009; 66: 228-235.
- Gandhi SK, Marts BC, Mistry BM, Brown JW, Durham RM, Mazuski JE, et al. Selective management of embolized intracardiac missiles. Ann Thorac Surg. 1996; 62: 290-292.
- Klein JA, Nowak JE, Sutherell JS, Wheeler DS. Nonsurgical management of cardiac missiles. Pediatr Emerg Care. 2010; 26: 36-38.
- Nakamura DS, McNamara JJ, Sanderson L, Harada R. Thoracic air gun injuries in children. Am J Surg. 1983; 146: 39-42.
- Greenlees G, Govewalla P, Haqzad Y, Sharkey A, Cartwright N. Penetration of the Heart by an Airgun Pellet: A Case Without Significant Effusion or Valvular Injury. Ann Thorac Surg. 2019; 108: e9-e10.