
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Benckiser’s hemorrhage following a vasa previa rupture:
An uncommon case report
Mariam Mahtate1*; Aziz Slaoui²; Soukaina Cherradi1; Najia Zeraidi1; Brahim Rhrab1; Amina Lakhdar1; Aziz Baydada1
1Gynecology-Obstetrics and Endoscopy Department, Maternity Souissi, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco.
2Gynecology-Obstetrics and Endocrinology Department, Maternity Souissi, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco.
*Corresponding Author : Mariam Mahtate
Gynecology-Obstetrics and Endoscopy Department, Maternity Souissi, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco.
Tel: 0021-262-566-7820;
Email: mariam.mahtate@gmail.com
Received : Oct 07, 2022
Accepted : Oct 27, 2022
Published : Nov 03, 2022
Archived : www.jcimcr.org
Copyright : © Marinova (2022).
Abstract
Background: Vasa praevia is an uncommon but very serious condition that is characterized by the presence of vessels belonging to the fetal circulation in the amniotic membranes surrounding the internal cervical os below the fetal presenting part. These vessels are at risk of rupture in active labor, or when the membranes spontaneously or artificially rupture, which can result in an acute fetal exsanguination and death. The prenatal diagnosis is thus of paramount importance, allowing a prophylactic cesarean section and therefore avoids severe Benckiser’s hemorrhage responsible for very high neonatal mortality.
Case report: We hereby report an uncommon case of 36-year-old patient who presented to the emergency department for spontaneous rupture of the membranes and painless vaginal bleeding at a gestational age of 35 weeks. The transvaginal ultrasonography in combination with color Doppler revealed membranous fetal blood vessels crossing the internal cervical os which was indicative of vasa previa. The patient underwent an emergency cesarean section, giving birth to an anemic female newborn that required immediate resuscitation, including intubation and blood transfusions.
Conclusion: Even if vasa previa is considered to be a rather rare condition observed in obstetric practice, it seriously threatens the life of the fetus and requires prompt management.
Keywords: Vasa praevia; Pregnancy; Bleeding; Neonatal mortality; Benckiser’s hemorrhage.
Abbreviations: VP: Vasa Previa; TA-USG: Trans-abdominal ultrasonography; TV-USG : Trans-vaginal ultrasonography; NICU: Neonatal intensive care unit; IVF: In-vitro fertilization.
Citation: Mahtate M, Slaoui A, Cherradi S, Zeraidi N, Rhrab B, et al. Benckiser’s hemorrhage following a vasa previa rupture: An uncommon case report. J Clin Images Med Case Rep. 2022; 3(11): 2137.
Background
Vasa previa is an uncommon condition in which the vessels belonging to the fetal circulation in the amniotic membranes cross or run in close proximity to the internal cervical os underneath the presenting part [1]. They can either lead from the placenta to a velamentous cord insertion (Type 1) or connect the main placental plate to a succenturiate lobe (Type 2) [1,2]. Unsupported by the umbilical cord or placental tissue, these vessels can tear causing an uncontrollable hemorrhage, called Benckiser’s hemorrhage [2]; putting the fetus in distress and leading to rapid fetal death, sometimes within minutes, through exsanguination in utero [2,3]. This hemorrhage of fetal origin happens most often when the membranes rupture, whether spontaneously or artificially. Sometimes the rupture of the membranes spares these vessels [3]. However, the risk of hemorrhage remains present, since it can occur by dilaceration of the vessels during the progression of the fetal presentation in the pelvis [2-4].
The presenting fetal part may also exert direct pressure on the unprotected vessels resulting in fetal distress due to hypoxia [3].
This is why prenatal identification of VP via ultrasound can only be beneficial and make it possible to schedule a prophylactic cesarean section before the onset of fetal death as well as other adverse perinatal outcomes [3-5]. By this case report, we aim to shed light on vasa previa and their risk factors in order to contribute to their antenatal diagnosis and proper management. For this purpose, we present a case of ruptured vasa previa incidentally diagnosed by transvaginal ultrasonography combined with color Doppler in a patient with spontaneous rupture of the membranes and painless vaginal bleeding. She then underwent an emergency cesarean section, giving birth to an anemic female newborn that required immediate resuscitation, including intubation and blood transfusions.
Case report
We hereby report an uncommon case of a primiparous 36-year-old woman, with no particular pathological history apart from placenta previa diagnosed at 26 weeks of gestation, who presented to the gynecological emergency department at our institution complaining of spontaneous rupture of the membranes and painless vaginal bleeding at a gestational age of 35 weeks.
Upon admission, Blood pressure was 118/69 mmHg, Heart rate was 80 beats per minute and normal uterine tone.
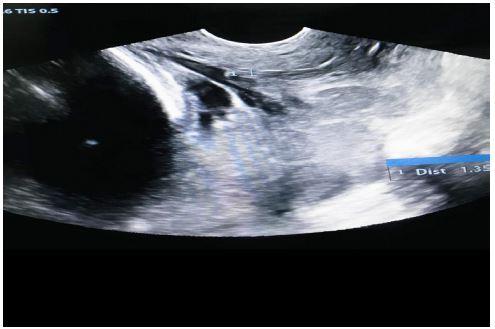
TA-USG showed fetal growth appropriate for the gestational age and the placenta attached to posterior uterine wall. TV-USG revealed placental location at 1.35 cm from the internal cervical os (Figure 1). Furthermore, membranous fetal vessels were observed to pass across the cervical internal os using real-time color Doppler ultrasonography (Figure 2). Therefore, a diagnosis of low-lying placenta complicated by vasa previa was made.
The fetal heart rate in the cardiotocographic recording showed a sinusoidal pattern.

An emergency caesarean section was then immediately performed for suspected ruptured vasa praevia, allowing the birth of a pale female newborn weighing 2580 g, with Apgar scores 3 and 6 at 1 and 5 min respectively, requiring immediate resuscitation and admission in neonatal intensive care unit for blood transfusions.
Placental examination after delivery was consistent with our diagnosis of a velamentous cord insertion with rupture of one of the vessels running along the membranes.
Postpartum period was uneventful and the patient was discharged on the fourth day after delivery. The baby was discharged from NICU in a healthy condition after 2 weeks of admission with hemoglobin at 14.5 g/dl.
Discussion
Vasa praevia is an uncommon but serious condition, with an estimated incidence ranging from 1 in 2000 to 1 in 6000 pregnancies [4,6]. However, its true incidence has been underreported as it may be mistaken for placental abruption or placenta previa [6].
Whereas the exact cause of VP is unclear, several risk factors have been reported, which include velamentous cord insertion, bilobed or succenturiate placenta and second-trimester low-lying placenta or placenta praevia. Pregnancies conceived via IVF, multiple gestations, and prior uterine surgeries may also increase the risk of vasa previa [7-10].
Our patient had history of second trimester complete placenta previa; its upward migration and resolution resulted in velamentous cord insertion.
Several case reports have demonstrated the ability of ultrasonography and color Doppler to diagnose vasa praevia prenatally in high risk pregnancies, preventing then the onset of complications related to their rupture [9-12]. Unfortunately, detailed prenatal ultrasonography screening for vasa previa was not performed in our case. Oyelese et al. [12] compared women who received prenatal diagnosis to those who did not and reported neonatal survival rates of 97% and 44% respectively, and blood transfusion rates of 3.4% and 58.5% respectively.
The classic clinical presentation of VP rupture is painless vaginal bleeding (also known as Benckiser’s hemorrhage) at time of spontaneous rupture of membranes, amniotomy or cervical dilatation; accompanied by fetal heart rate irregularities [10,13]. In our case, transvaginal ultrasonography combined with color Doppler incidentally showed fetal blood vessels coursing over the internal cervical os; the occurrence of vaginal bleeding and a sinusoidal heart-rate pattern reflecting fetal anemia were consistent with the diagnosis of ruptured vasa previa. Spontaneous rupture of membranes was the reason behind this rupture.
The bleeding that occurs, even if it is sparse, usually results in hypovolemic shock of the newborn; as the total blood volume of the fetus at term is approximately 80–100 ml/kg [9]. Only rapid extraction associated with resuscitation and neonatal transfusions reduce mortality and neonatal morbidity [9,12]. This is why antenatal screening of vasa previa can only be beneficial and make it possible to schedule a prophylactic cesarean section before the onset of these complications [9]. Our patient underwent an emergency cesarean section, giving birth to an anemic female newborn, which required immediate resuscitation, including intubation and blood transfusions; the neonate outcome has then improved and was discharged from NICU with hemoglobin at 14.5 g/dl.
Thus, several authors emphasize that, in the presence of confirmed vasa previa, an elective caesarean section should be carried out prior to the onset of labor, most often around 34–36 weeks, avoiding rupture of membranes and fetal exsanguination, while taking into consideration the impact of iatrogenic prematurity [9-12].
As the aim of surgery is to prevent rupture of aberrant vessels, it is recommended to start the hysterotomy with a superficial transverse incision, allowing the visualization of the blood vessels oriented towards the cervix [13]. An amniotomy avoiding these vessels can then be carried out to allow delivery of the fetus [13].
Conclusion
Vasa praevia is an uncommon condition in which the most feared complication is Benckiser’s hemorrhage. Prenatal diagnosis is thus of paramount importance, allowing an elective caesarean section, and therefore prevents potential rupture of the low-lying vessel (s) and subsequent fetal demise or neonatal morbidity.
Declarations
Guarantor of submission: The corresponding author is the guarantor of submission.
Acknowledgements: None.
Funding: There are no funding sources to be declared.
Availability of data and materials: Supporting material is available if further analysis is needed.
Competing interests: The authors declare that they have no competing interests.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate: Ethics approval has been obtained to proceed with the current study. Written informed consent was obtained from the patient for participation in this publication.
References
- Melcer Y, Jauniaux E, Maymon S, et al. Impact of targeted scanning protocols on perinatal outcomes in pregnancies at risk of placenta accreta spectrum or vasa praevia. Am J Obstet Gynecol 2018; 218: 443.e1-443.e8.
- Rachel G Sinkey, Anthony O Odibo, MSCE. Diagnosis and management of vasa praevia, American Journal of Obstetrics & Gynecology. 2015; 213, ISSUE 5, P615-619.
- Sullivan Elizabeth A, Javid Nasrin; Duncombe Gregory, Li Zhuoyang, Safi Nadom, et al. Vasa praevia Diagnosis, Clinical Practice, and Outcomes in Australia; Obstetrics & Gynecology. 2017; 130: 591-598.
- Oyelese KO, Turner M, Lees C, Campbell S. Vasa praevia: An avoidable obstetric tragedy. Obstet Gynecol Surv 1999; 54: 138–45.
- Mulot S, Valentin L, Dreyfus M, Benoist G, et al. Vasa prævia : quand et comment rechercher les vasa prævia en échographie et quelle prise en charge proposer aux patientes en cas de découverte d’un vasa prævia ? À propos de quatre cas et revue de la littérature. Revue de Médecine Périnatale. 2017.
- Stafford I, Neumann E, Abnormal placental structure and vasa praevia. Journal of Ultrasound in Medicine. 2004; 23: 1521–1522.
- McQueen V, Speed M, Rutter S, Gray T, et al. Vasa praevia: Should we routinely screen high-risk women for this rare but serious condition? Ultrasound. 2018; 26: 127–131.
- Gagnon R, Morin L, Bly S, et al. Directive clinique sur la prise en charge du vasa praevia. J Obstet Gynecol Can. 2009; 31: 754–760.
- Carbonnel M, Tigaizin A, Carbillon L, et al. Vasa praevia: A propos d’un cas. Gynecol Obstet Fertil. 2007; 35: 327–329.
- Ruiter L, Kok N, Limpens J, Derks JB, de Graaf IM, Mol BW, et al. A systematic review on the diagnostic accuracy of ultrasound in the diagnosis of vasa praevia. Ultrasound Obstet Gynecol 2015; 45: 516–522.
- Andre F. Lijoi and Joanna Brady. Vasa praevia Diagnosis and Management. The Journal of the American Board of Family Practice November. 2003; 16: 543-548.
- Oyelese Y, Catanzarite V, Prefumo F, Lashley S, Schachter M, Tovbin Y, et al. Vasa praevia: The impact of prenatal diagnosis on outcomes », Obstet Gynecol. 2004; 103: 937–942.
- Tsakiridis I, Mamopoulos A, Athanasiadis A, Dagklis T, et al. Diagnosis and Management of Vasa praevia. Obstetrical & Gynecological Survey. 2019; 74: 436–442.