
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Severely symptomatic proximal DVT following cancer, successfully treated by rheolytic thrombectomy
Azin Alizadehasl1; Seyed Amir Hossein Emami2; Kamran Roudini2; Alia Bahramnejad1*; Amir Dousti3; Rezvaneh Shourmeij1
1Cardio-Oncology Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
2Cancer Institute, Imam Khomeini Hospital, Tehran University of Medical sciences, Tehran, Iran.
3Interventional Cardiology research center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Alia Bahramnejad Rajaie
Cardiovascular Medical and Research Center, Niayesh highway, Tehran, Iran.
Ph: +98-9121-570-518;
Email: Aaly_brnj@yahoo.
Received : Sep 10, 2022
Accepted : Oct 28, 2022
Published : Nov 04, 2022
Archived : www.jcimcr.org
Copyright : © Rajaie AB (2022).
Abstract
Cancer associated thrombosis is well known in patients with cancer. Following proximal DVT, post thrombotic syndrome is prevalent. Our patient with history of colon cancer presented with proximal DVT with extreme swelling of the leg and treated successfully with Angio Jet Zelante DVT catheter, a procedure which is safe and effective.
Keywords: Cancer; Thrombosis; Secondary prevention.
Abbreviations: VTE: Venous Thromboembolism; CAT: Cancer Associated Thrombosis; DVT: Deep Vein Thrombosis; PTS: Post Thrombotic Syndrome; DOACS: Direct Acting Oral Anticoagulant Drugs; CDT: Catheter Directed Thrombolysis; ECG: Electrocardiogram; LVH: Left Ventricle Hypertrophy; TTE: Trans Thoracic Echocardiography; LVEF: Left Ventricle Ejection Fraction; GLS: Global Longitudinal Strain; RV: Right Ventricle; CXR: Chest Radiograph; BMI: Body Mass Index; IV: Intravenous; FV: Femoral Vein; CFV: Common Femoral Vein; EIV: External Iliac Vein; CIV: Common Iliac Vein; IVC: Inferior Vena Cava.
Citation: Alizadehasl A, Hossein Emami SA, Roudini K, Bahramnejad A, Dousti A, et al. Severely symptomatic proximal DVT following cancer, successfully treated by rheolytic Thrombectomy. J Clin Images Med Case Rep. 2022; 3(11): 2143.
Introduction
Since 1865 when Armand Trousseau described relationship between cancer and Venous Thromboembolism (VTE), our knowledge about Cancer Associated Thrombosis (CAT), its diagnosis, prevention, and management has had many advances [1]. VTE is the third most common cause of cardiovascular death, and is the second cause of mortality in patients with cancer [2]. Treatment of VTE is aimed to reduction of mortality and morbidity, furthermore improving quality of life is an overriding task. One of conditions following Deep Vein Thrombosis (DVT) of illiofemoral veins (proximal veins of lower limbs) is Post Thrombotic Syndrome (PTS) which may highly influence the quality of life of patients. There is numerous ways to prevent PTS including oral anticoagulant therapy especially with Direct Acting Oral Anticoagulant Drugs (DOACs), Elastic Compression Stocking (ECS), and invasive endovascular interventions like Catheter Directed Thrombolysis (CDT) and pharmacomechanical (rheolytic) thrombolysis [3]. Here we aimed to describe a case of proximal iliofemoral DVT which treated by Angio Jet Zelante DVT catheter.
Case presentation
A 63 year old gentleman, presented to hospital with swelling of left lower limb. His past medical history was significant for hypertension and diabetes mellitus and colon cancer. The colon adenocarcinoma was diagnosed six months ago. He has had total colectomy and was on Folfox chemotherapy. He was smoker with 20 packed/year smoking, and had no history of recent travel. On admission the patient had pulse rate of 74 beats per minute and blood pressure was 130/75 mmHg and Respiratory rate was 14 cycles per minute. Pulse oxymeter showed blood oxygen saturation 96% in room air, lungs were clear in auscultation and heart had a regular rhythm without murmur. The patient’s abdomen was soft without palpable mass. His Body Mass Index (BMI) was 25 Kg/m2. Limb examination showed swelling of left limb with pain and tenderness with changes in colour and temperature.
Cellular blood count was unremarkable, 12 leads Electrocardiogram (ECG) showed normal sinus rhythm with normal axis and voltage criteria for Left Ventricle Hypertrophy (LVH) was remarkable.
Trans Thoracic Echocardiography (TTE) was performed and showed left Ventricle Ejection Fraction (LVEF): 50%, no regional wall motion abnormality, mild LVH, grade I diastolic dysfunction, no hemodynamic significant valve disease, Global Longitudinal Strain (GLS): -17, and normal size and function of Right Ventricle (RV). Chest Radiograph (CXR) was normal.
Colour and pulse Doppler study of left lower limb showed hyper echo material in left iliac, femoral, and popliteal veins in favour of acute or sub acute extensive DVT without revascularization.
With diagnosis of DVT, Intravenous (IV) heparin started as baseline of treatment then further investigation was done by CT venography which showed dilatation and intra luminal filling defects in popliteal vein, Femoral Vein (FV), Common Femoral Vein (CFV), External Iliac Vein (EIV), Common Iliac Vein (CIV), and most proximal (lower end) of Inferior Vena Cava (IVC) in favour of acute DVT.
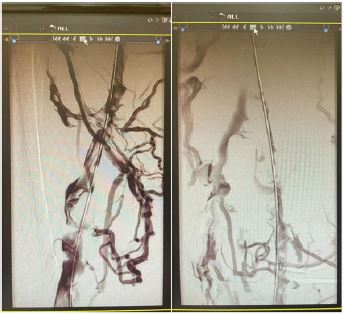
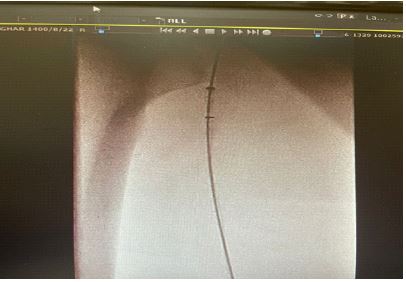
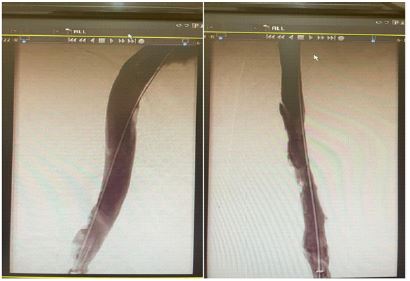
According to very disturbing severe swelling of patient’s left lower limb and high possibility of PTS, the patient was candidate for invasive venography and pharmaco-mechanical thrombolysis. Venography via left popliteal vein access showed fresh thrombosis in proximal veins of left lower limb with many collateral formation (Figure 1). Then via same access through a 8 Fr sheath, Angio Jet Zelante DVT catheter entered and alteplase spray in the whole path was done (Figure 2), 30 min break time took place in order to give an opportunity to the medication for making effect and then via same catheter thrombosuction was done. Finally another venography was done which showed fully patency of venous lumen and all of clots were resolved and all of collateral veins were disappeared as an excellent final result (Figure 3).
After the procedure popliteal sheath of access was took out and hemostasis was done the elastic bandage was done and IV heparin started which later changed to DOAC and patient discharged with relieved pain and swelling of his left lower limb. (Figure 4).

Discussion
DVT especially the proximal ones needs to treat promptly and rapidly or there would be high risk for development of Pulmonary Embolism (PE) and/or venous dysfunction resulting in PTS. Traditional treatment for DVT is anticoagulant mainly focused on stabilizing the clot in order to prevent PE but with traditional treatment including anticoagulant and ECS about half of patients with DVT will have venous insufficiency and PTS [4]. The PTS is chronic sequelae of DVT, and is a disabling condition that patients would frequently need medical support. Manifestations of PTS vary from mild to more severe manifestations such as chronic leg pain which disturbs patient’s activity, intractable edema, and leg ulcers. PTS decreases quality of life and productivity and is costly as measured by health resource utilization, and patient’s out of pocket [5]. CDT, balloon angioplasty, and stenting are some endovascular interventions which have showed promises to decrease PTS [6].
Suresh Vedantham et al. performed a phase III, multicenter, open label, assessor-blinded, randomized clinical trial in which they enrolled 692 patients with acute DVT into two groups, 336 patients in pharmaco-mechanical thrombolysis group and 355 patients assigned to control group, they found in patients with acute proximal DVT, a treatment strategy that included first-line Angio Jet catheter directed thrombolysis was reasonably safe and led to an improved symptom status and venous quality of life at 1 month and reduced PTS at 6 months compared with anticoagulation alone [7].
In conclusion using pharmaco-mechanical thrombolysis in patients with proximal DVT has a role in preventing PTS.
Disclosure: The authors have nothing to disclose.
Funding: There was no funding.
References
- Norbaini Binti Abdol Razak, Gabrielle Jones, Mayank Bhandari, Michael C. Berndt and Pat Metharom. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018; 10: 380.
- Caio J Fernandes, Luciana TK Morinaga, José L Alves Jr et al. Cancer-associated thrombosis: the when, how and why. Eur Respir Rev. 2019; 28: 180119. https://doi.org/10.1183/16000617.0119-2018
- Paolo Prandoni. New perspectives for prevention of the post-thrombotic syndrome. Bleeding, Thrombosis and Vascular Biology. 2022; 1: 20.
- Maofeng Gong, Guanqi Fu, Zhengli Liu et al. Rheolytic Thrombectomy Using Angio Jet Zelante DVT Catheter or Solent Omni Catheter fot Treatment of Patients with Proximal Vein Thrombosis. Research square 2021. https://doi.org/10.21203/rs.3.rs-1073588/v1
- Susan R. Kahn; The post-thrombotic syndrome. Hematology Am Soc Hematol Educ Program. 2016; 2016: 413–418.
- Giovanni Gautier, Frederic Douane, Arthur David et al. Pharmaco-mechanical catheter-directed thrombolysis versus recanalization and stenting for post thrombotic syndrome after lower limb deep vein thrombosis: A comparative study. Quantitative Imaging in Medicine and Surgery. 2022; 12: 1664-1673.| https://dx.doi.org/10.21037/qims-21-572
- Suresh Vedantham, Amber Salter, Samantha Lancia, Lawrence Lewis, Siddhant Thukral, et al. Clinical Outcomes of a Pharmacomechanical Catheter-Directed Venous Thrombolysis Strategy that Included Rheolytic Thrombectomy in a Multicenter Randomized Trial. J Vasc Interv Radiol 2021; 32: 1296–1309. https://doi.org/10.1016/j.jvir.2021.06.001