
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
The impact of the intensive immunosuppressive treatment, a case report of ROHHAD syndrome in two siblings
Abolfazl Amjadipour1; Lobat Shahkar2*; Ali Ahani Azari3
1Student Research Committee, Medicine Faculty, Golestan University of Medical Sciences, Gorgan, Iran.
2Neonatal and Children’s Health Research Centre, School of Medicine, Golestan University of Medical Sciences, Gorgan, Iran.
3Anaesthesiologist, Mousavi Hospital, Gorgan, Iran.
*Corresponding Author : Lobat Shahkar
Taleghani Hospital, Gorgan, Iran.
Email: lobatshahkar@yahoo.com
Received : Oct 17, 2022
Accepted : Nov 02, 2022
Published : Nov 09, 2022
Archived : www.jcimcr.org
Copyright : © Shahkar L (2022).
Abstract
Introduction: ROHHAD is an acronym for rapid-onset obesity with hypoventilation, hypothalamic, and autonomic dysregulation. It is a rare disorder that presents with rapidly onset obesity with multiorgan disorders during early childhood. There are less than 100 cases reported. In this paper, we aimed to present a case of ROHHAD syndrome with rare neurologic symptoms. We also discuss our treatment regimen for this specific patient.
Case presentation: Our patient was first admitted to our department at the age of 6 years and 8 months old. Her symptoms started to show 7 month ago, at the age of 6. During a period of six month she has gained 9 kilograms as well as her previous obesity. The first child of these parents has also been diagnosed with the ROHHAD syndrome. We also have reported his symptoms and how his disease was diagnosed in another paper which has been published. She is suffering from somnolence and sleep apnea. She recently has been suffering from ataxia and imbalance with multiple falling accidents. She could not continue her school because of her violent acts and self-harming behaviours. She did not have any signs of central precocious puberty, only started to grow some pubic hair with no other sign of puberty.
Conclusion: Our case indicates that genetics might be a risk factor for ROHHAD syndrome. In this paper we reported a family with two children suffering from this rare disease, which raises the importance of more in depth genetic experiments about this syndrome. Our observations during her treatment process and the impact of IVIG might shed more light on the immunologic aspect of this syndrome. We believe that this regime should be more in consideration of other patients.
Keywords: Rapid-onset obesity with hypoventilation; Hypothalamic dysfunction; Obesity.
Citation: Amjadipour A, Shahkar L, Azari AA. The impact of the intensive immunosuppressive treatment, a case report of ROHHAD syndrome in two siblings. J Clin Images Med Case Rep. 2022; 3(11): 2149.
Introduction
ROHHAD is an acronym for rapid-onset obesity with hypoventilation, hypothalamic, and autonomic dysregulation. It is a rare disorder that presents with rapidly onset obesity with multiorgan disorders during early childhood with fewer than 100 cases reported. The diagnostic criteria for this syndrome and the ROHHAD term were first described by Ize-Ludlow et al [1]. The important aspects of this syndrome include significant weight gain over a period of six to twelve months in the first 10 years of life, followed by dysregulation of the autonomic nervous system, alveolar hypoventilation, and hypothalamic dysfunction.
Congenital Central Hypoventilation Syndrome (CCHS) which is presented with paired-like homeobox 2B (PHOX2B) mutation is a different entity, although sharing a lot of similarities in symptoms and signs with ROHHAD [2]. The rapid-onset weight gain (often 14 kilograms in 6-12 months) is typically the herald of the disease and the harbinger of the later features of the ROHHAD phenotype. ROHHAD can be seen by a variety of signs and symptoms. Till now there is not any single confirmatory diagnostic test. On the other hand, late diagnosis of this syndrome leads to late intervention and eventually high morbidity and mortality. It is of great value to have a very sensitive eye for symptoms of this syndrome especially in children over 2 years old with rapid onset obesity [1,3].
Case presentation
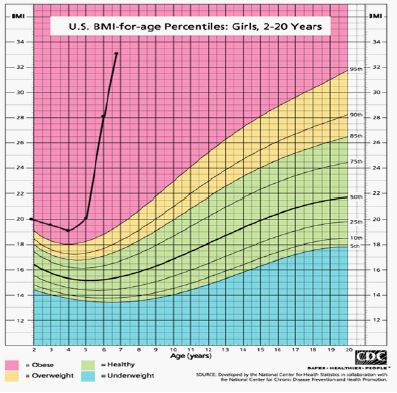
Our patient was first admitted to our department at the age of 6 years and 8 months old. The first child of these parents has also been diagnosed with the ROHHAD syndrome. We also have reported his symptoms and how his disease was diagnosed in another paper which has been published [4]. Her symptoms started to show 7 month ago, at the age of 6 when she was 31 kilograms. But only over a course of 8 months, she gained 9 kilograms and is now 40 kilograms. Unlike her brother she did not have any hyperphagia and even is experiencing dysphagia. Her height is 110 centimetre and with 40 kg weight, she has a BMI of 33 which is +8 SD for her age. Her BMI progression is shown in figure 1, based on a chart from National Center for Health Statistics [5].
The patient was born at term, from a 28 years old mother. Her mother had experienced no complications during pregnancy and the infant was delivered via caesarean section because of the previous caesarean section. There is no consanguinity between her parents. She was born with a normal-range weight of 3700 g and birth height of 48 cm. The child had a normal neonatal period and had normal growth and psychomotor development.
She is very sleepy during the day and she used to wake up during her sleep from apnea one to two times every night. She also complains of excessive night sweats and thermal dysregulation. Like her brother, she is also having ataxia and poor balance in gait. She is suffering from urinary incontinence and enuresis. She also had gastrointestinal dysmotility and constipation from the past year and she has a chronic anal fissure which causes two episodes of hemmorrhage after defection every month. She started preschool at the age of 6. She could not continue her school because of her violent acts and self-harming behaviours. Her mother stated that she has punched her head multiple times. Sometimes she has hit her head against the wall without any reason.
Her physical examinations revealed tachycardia with heart rate of 120 bpm, normal blood pressure of 105/60 mmHg and tachypnea with respiratory rate of 30. She is an obese girl with BMI of 33. She has a moonlike face, marked rapid weight gain with central obesity and buffalo hump, adipomastia and supraclavicular fat pad. She did not have any signs of central precocious puberty, only started to grow some pubic hair with no other sign of puberty. Her extremities were not cold and there was not any sign of purple striae, plethora, acne, acanthosis nigricans or hyperpigmentation. She had no alteration in pain perception nor sign of pulmonary hypertension: JVP, hepatomegaly, pedal edema. Her complete lab data is shown in Table 1. She had increased levels of Prolactin with twice the normal upper limit
Because of this increased prolactin and the association of ROHHAD syndrome with neural tumour Syndrome we asked for a whole body Positron Emission Tomography with Computerised-Tomography scan (FDG-PET/CT). Her FDG-PET/CT revealed multiple enlarged lymph nodes in the neck and intraperitoneal abdominopelvic regions without significant uptake caused by a previous inflammatory process. The patient was further investigated using Metaiodobenzylguanidine scan (MIBG scan) which showed no abnormal radiotracer uptake throughout the body.
Discussion
ROHHAD is an extremely complex syndrome which requires a high level of suspicion for diagnosis and must be managed by a multidisciplinary team including endocrinologists, psychiatrists, surgeons, pneumologists, oncologists, neuro-paediatricians, and cardiologists, among other specialists. Even in conservative management, it is vitally important to have early management in order to improve the prognosis.
This syndrome is currently known as ROHHAD-NET because around 40% of ROHHAD syndrome also present with neural crest origin tumours of e.g. ganglioneuroma, ganglioneuroblastoma; on some occasions, these tumours may even appear several years after first symptom onset [5]. The underlying pathogen esis of ROHHAD is unclear, but a combination of genetic predisposition and paraneoplastic or immunological factors have been suggested. However, no genetic alterations or epigenetic changes specific to this syndrome have been identified, yet.
Table 1: Laboratory findings.
| Parameters - unit | Results | Normal range |
|---|---|---|
| blood biochemical | ||
| WBC /μL | 8500 | 4500 - 13500 |
| Neutrophil | 45% | |
| Lymphocyte | 53% | |
| Hb g/dL | 12 | 11.2 - 14.1 |
| MCV FL | 79.7 | 68 - 75 |
| MCH pg | 26.0 | 25 - 33 |
| MCHC g/dL | 32.6 | 31 - 37 |
| Platelet /μL | 248000 | 140000 - 400000 |
| Fasting Blood sugar mg/dL | 80 | 70 - 115 |
| BUN mg/dL | 11.6 | 5 - 23 |
| Creatinine mg/dL | 0.60 | 0.7 - 1.4 |
| Triglyceride mg/dL | 0.61 | < 200 |
| Cholesterol mg/dL | 124 | < 200 |
| HDL mg/dL | 39 | 45-65 |
| LDL mg/dL | 67 | < 130 |
| Hormone | 180 -2 00 | |
| T4 μg/dL | 7.62 | 5.4-11.2 |
| TSH mU/L | 4.05 | 0.58-4.1 |
| Prolactine ng/mL | 68.4 | 5.0-35.0 |
| cortisol 8 A.M mcg/dL | 8.92 | 4.8-19.2 |
| ACTH pg/mL | 11.5 | < 46 |
| Urine Biochemistry | ||
| Volume mL/24 hour | 400 | 650-1000 |
| Urine Protein mg/24 hour | 32 | < 150 |
| Urine free cortisol mcg/ 24 hour | 2.3 | 1.5-63 |
| Urine Creatinine mg/24 hour | 660 | 600-1800 |
| Vinyl mandolin acid mg/24 hour | 2.27 | < 13.6 |
The presence of oligoclonal bands and anti hypothalamus and anti pituitary antibodies in cerebrospinal fluid analysis of several cases of ROHHAD has suggested the immune-mediated pathogenesis [14,15]. Association with celiac disease, may suggest further evidence for immune-mediated etiology [16]. Encephalitis characterised by perivascular lymphocytic infiltrate in autopsy findings of six children with ROHHAD syndrome is also in favour of the immune mediated pathogenesis [17].
Another reason suggesting immune-mediated pathogenesis in ROHHAD has been shown by the good outcomes of the intensive immunosuppressive treatment for the neuropsychological function. These treatments included cyclophosphamide, rituximab, immunoglobulin and corticoids [18,19]. In another 15-old-year patient with ROHHAD syndrome the intensive immunosuppressive treatment including corticosteroids, immunoglobulins and long term mycophenolate mofetil had improving outcomes for the neuropsychological function and autonomic aspects of this syndrome [20].
In our case, we started the IVIG regime and after three doses of IVIG, the patient is having less difficulties in sleep with significant improvements in her balance. The effects started to show after the third dose and still have not been reversible. We believe that this therapeutic regime should be more in the spotlight and by bringing the focus of the studies on this topic, we can grasp better on the pathophysiology and as a result, better treatment outcomes in ROHHAD patients.
Hypothalamic dysfunction is variable. If present, a strict fluid intake regimen and specific hormone replacement should be considered in the management. It is shown that hypoventilation responds very well to artificial ventilation during sleep in the first years of evolution with progressive need for continuous ventilatory support. These procedures, available at home, may improve the quality of life and prevent sudden death. As mentioned before, early detection of breathing and sleep disorders and therapeutic interventions have a significant role in morbidity and mortality in ROHHAD syndrome. We have started non-invasive ventilation for our patient which has improved her quality of sleep and decreased her somnolence during the day.
Conclusion
Our case indicates that genetics might be a risk factor for ROHHAD syndrome. In this paper we reported a family with two children suffering from this rare disease, which raises the importance of more in depth genetic experiments about this syndrome. Our observations during her treatment process and the impact of IVIG might shed more light on the immunologic aspect of this syndrome. We believe that this regime should be more in consideration of other patients.
Declarations
Authors contribution: Drafting of the manuscript and critical revision of the manuscript for important intellectual content: A. A.; Acquisition and analysis and interpretation of data: A. A., and A. Ah.; Study concept and design and Study supervision: L. S.
Conflict of interests: The authors declare that we have no known competing financial interests or personal relationships.
Funding/support: This study did not receive any grant.
Informed consent: The authors obtained informed consent from the patient’s parents in Persian.
References
- Ize Ludlow D, Gray JA, Sperling MA, Berry Kravis EM, Milunsky JM, Farooqi IS, et al. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation presenting in childhood. Pediatrics. 2007; 120: e179-188.
- Katz ES, McGrath S, Marcus CL. Late-onset central hypoventilation with hypothalamic dysfunction: A distinct clinical syndrome. Pediatric pulmonology. 2000; 29: 62-68.
- Rand CM, Patwari PP, Rodikova EA, Zhou L, Berry-Kravis EM, Wilson RJ, et al. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation: Analysis of hypothalamic and autonomic candidate genes. Pediatric research. 2011; 70: 375-378.
- Amjadipour A, Shahkar L, Hanafi F. A Case Report of ROHHAD Syndrome in an 8-year-old Iranian Boy. Int J Endocrinol Metab. 2021; 19: e111571.
- Statistics NCfH. Centers for Disease Control and Prevention Growth charts: Centers for Disease Control and Prevention; 2020 [Available from: https://www.cdc.gov/growthcharts/cdc_charts.htm.
- Bougnères P, Pantalone L, Linglart As, Rothenbühler A, Le Stunff C. Endocrine Manifestations of the Rapid-Onset Obesity with Hypoventilation, Hypothalamic, Autonomic Dysregulation, and Neural Tumor Syndrome in Childhood. The Journal of Clinical Endocrinology & Metabolism. 2008; 93: 3971-3980.
- Ouvrier R, Nunn K, Sprague T, McLean C, Arbuckle S, Hopkins I, et al. Idiopathic hypothalamic dysfunction: A paraneoplastic syndrome? The Lancet. 1995; 346: 1298.
- Abaci A, Catli G, Bayram E, Koroglu T, Olgun HN, Mutafoglu K, et al. A case of rapid-onset obesity with hypothalamic dysfunction, hypoventilation, autonomic dysregulation, and neural crest tumor: ROHHADNET syndrome. Endocrine practice: Official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2013; 19: e12-16.
- Huppke P, Heise A, Rostasy K, Huppke B, Gärtner J, et al. Immunoglobulin Therapy in Idiopathic Hypothalamic Dysfunction. Pediatric Neurology. 2009; 41: 232-234.
- Patwari PP, Rand CM, Berry Kravis EM, Ize-Ludlow D, Weese Mayer DE, et al. Monozygotic twins discordant for ROHHAD phenotype. Pediatrics. 2011; 128: e711-e715.
- Lee JM, Shin J, Kim S, Gee HY, Lee JS, Cha DH, et al. Rapid-Onset Obesity with Hypoventilation, Hypothalamic, Autonomic Dysregulation, and Neuroendocrine Tumors (ROHHADNET) Syndrome: A Systematic Review. Biomed Res Int. 2018; 2018: 1250721
- Ibáñez-Micó S, Marcos Oltra AM, de Murcia Lemauviel S, Ruiz Pruneda R, Martínez Ferrández C, et al. Rapid-onset obesity with hypothalamic dysregulation, hypoventilation, and autonomic dysregulation (ROHHAD syndrome): A case report and literature review. Neurologia (Barcelona, Spain). 2017; 32: 616-622.
- Carroll MS, Patwari PP, Kenny AS, Brogadir CD, Stewart TM, Weese-Mayer DE. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation (ROHHAD): Response to ventilatory challenges. Pediatric pulmonology. 2015; 50: 1336-1345.
- Sartori S, Priante E, Pettenazzo A, et al. Intrathecal synthesis of oligoclonal bands in rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation syndrome: New evidence supporting immunological pathogenesis. J Child Neurol. 2014; 29: 421–425.
- Giacomozzi C, Guaraldi F, Cambiaso P, et al. Anti-Hypothalamus and Anti-Pituitary Auto-antibodies in ROHHAD Syndrome: Additional Evidence Supporting an Autoimmune Etiopathogenesis. Horm Res Paediatr. 2019; 92: 124–132.
- Cemeroglu AP, Eng DS, Most LA, Stalsonburg C, Kleis L, et al. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation syndrome and celiac disease in a 13-year-old girl: Further evidence for autoimmunity? J Pediatr Endocrinol Metab. 2016; 29: 97–101.
- Gharial J, Ganesh A, Curtis C, et al. Neuroimaging and Pathology Findings Associated With Rapid Onset Obesity, Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation (ROHHAD) Syndrome. J Pediatr Hematol Oncol. 2020; 11.
- Paz Priel I, Cooke D, Chen A. Cyclophosphamide for Rapid-Onset Obesity, Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation Syndrome. J Pediatr. 2011; 158: 337–339.
- Jacobson L, Rane S, McReynolds L, Steppan D, Chen A, Paz-Priel I, et al. Improved Behavior and Neuropsychological Function in Children With ROHHAD After High-Dose Cyclophosphamide. Pediatrics. 2016; 138: e20151080.
- Chow C, Fortier MV, Das L, et al. Rapid-Onset Obesity With Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation (ROHHAD) Syndrome May Have a Hypothalamus–Periaqueductal Gray Localization. Pediatr Neurol. 2015; 52: 521–525.