
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Image-guided radiotherapy using 4D cone-beam
computed tomography
AB Mohamed Yoosuf 1,2; Mamdouh Alqathami1,2,3*; Salem AlShehri1,3; Abdulrahman Alhadab1
1Department of Radiation Oncology, Ministry of National Guard – Health Affairs, Riyadh, Saudi Arabia.
2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia.
3King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia.
*Corresponding Author : Mamdouh Alqathami
Chief Medical Physicist, Department of Radiation Oncology, King Abdullah Specialist Children Hospital, King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia.
Email: alqathamima@gmail.com
Received : Oct 14, 2022
Accepted : Nov 03, 2022
Published : Nov 10, 2022
Archived : www.jcimcr.org
Copyright : © Alqathami M (2022).
Abstract
Purpose: A standard CBCT image lacks localization accuracy in the complex registration of a moving target. The 4D Cone Beam Computed Tomography (4D CBCT) is a useful tool for treating moveable tumors because it allows us to precisely pinpoint the location of the tumors during treatment and provide a guide during adaptive treatment strategy. This study evaluates the accuracy of 4D CBCT over a wide range of target motion scenarios.
Materials and methods: A CIRS dynamic thorax phantom with tumor insert of diameter 1 cm was used to acquire 4D images with induced respiratory motion (1D, 2D and 3D) along with varying amplitude and cycle time. Each scenario was imaged using device-less 4D CT with a slice thickness of 1.25 mm. The internal target volume was contoured on all 10 phases of images using MIP. VMAT plan with a single arc was created and compared to respective pre-treatment 4D CBCT in terms of translational and rotational accuracy. Each scenario was repeated three times for consistency.
Results: The mean shift between the planned and 4D CBCT-based images in lateral, longitudinal and vertical directions for all motion was 0.4 cm (± 0.1), 0.3 cm (± 0.2) and 0.7 cm (± 0.3) respectively. Similarly, the mean rotational shift between planned and 4D CBCT images were within 2˚ in all directions. The movements of the tumor during 4D CBCT were well within the ITV in all scenarios.
Conclusion : It has been determined that 4D CBCT is a useful tool for the care of mobile malignancies. The results demonstrate that when a moving tumor is the focus of radiation treatment, 4D CBCT registration can improve the localization accuracy and is consistent with those of 4D CT images.
Citation:Yoosuf ABM, Alqathami M, AlShehri S, Alhadab A, et al. Image-guided radiotherapy using 4D cone-beam Computed Tomography. J Clin Images Med Case Rep. 2022; 3(11): 2150.
Background
For treatment planning, treatment verification, and adaptive radiation in many malignancies, accurate Computed Tomography (CT) studies in the presence of respiratory motion are required [1]. The use of radiotherapy for lung cancer is growing, with Stereotactic Ablative Radiotherapy (SABR) currently being recommended as the first-line therapy for patients with Stage I NSCLC who are medically inoperable and require non-invasive treatment options [2]. To achieve the maximum therapeutic ratio, the underlying concept of administering a high and preferentially tumoricidal dosage to a target location while administering a low dose to nearby essential structures must still be followed [3]. The presence of positional uncertainty is a significant constraining factor in accurately modulating radiation to three-dimensional objects; this can be influenced by several factors, one of which is respiratory motion [4]. The normal lung parenchyma is frequently the dose-limiting constraint for curative radiation, and failing to account for lung tumor mobility related to respiration can result in both tumor underdosing and failure of local control.
Motion control may use many strategies, including breath-holding for respiratory control, abdominal compression plates, and radiation delivery strategies including gating and tracking [5]. Without taking respiratory motion into account, the image acquired can produce considerable aberrations that can affect target volume delineation as well as positional and volumetric data [6]. Standard CT slices can cause step artefacts, incomplete projection, and image blurring and take less time to acquire than the average breathing cycle (~5 sec) [7]. This may cause the original tumor’s size, shape, and location to be misrepresented.
Motion control may use many strategies, including breath-holding for respiratory control, abdominal compression plates, and radiation delivery strategies including gating and tracking [5]. Without taking respiratory motion into account, the image acquired can produce considerable aberrations that can affect target volume delineation as well as positional and volumetric data [6]. Standard CT slices can cause step artefacts, incomplete projection, and image blurring and take less time to acquire than the average breathing cycle (~5 sec) [7]. This may cause the original tumor’s size, shape, and location to be misrepresented.
Internal Target Volume (ITV) created using 4DCT is the most common method for motion management. ITV is calculated through examination of the Four-Dimensional Computed Tomography (4DCT) images in the case of tumors moving with respiration, such as lung cancer [8]. The radiotherapy plans are typically created using ITV along with setup margins [1,5,8,9]. Comparing the Cone Beam CT (CBCT) acquired prior to treatment with estimated target position and motion to the primary planning CT scan acquired during the simulation is a standard method for doing radiotherapy image-guided verification [10]. Beyond the crucial function of verification imaging in patient setup, variations in CT volumes have been modeled to extract radiobiological characteristics and employed as indicators for adaptive re-planning [1]. However, the target motion brought on by the patient’s breathing during CBCT acquisition could result in motion artefacts. Additionally, it reduces the target localization’s precision. This might make target localization less accurate [10]. Therefore, by using 4D CBCT to reduce ITV inconsistencies between treatment and plan steps, these issues can be minimized. Inter-observer variability of target localization for 4DCBCT and 3DCBCT imaging was compared using patient data by Sweeney et al [10]. They discovered that 4DCBCT had much less variability. The CBCT systems that permit the respiratory correlation have recently been presented by commercial vendors. Furthermore, the adaptive IGRT and volumetric modulated arc treatment, two of the most advanced radiotherapy systems, have examined the use of 4D CBCT for the estimation of Planning Target Volume (PTV) Margins (VMAT) [11-13]. This study evaluates the accuracy of 4D CBCT over a wide range of target motion scenarios.
Table 1: The dynamic thorax phantom target movement scenarios during 4DCT and preset shifts in all directions for each scenario.
| Superior / Inferior | Anterior / Posterior | Lateral | Amplitude | Cycle Time | |
|---|---|---|---|---|---|
| Scenario #1 | 10 mm | 0 | 0 | 5 mm | 5 sec |
| Scenario #2 | 10 mm | 5 mm | 0 | 5 mm | 5 sec |
| Scenario #3 | 10 mm | 5 mm | 5 mm | 5 mm | 5 sec |
| Scenario #4 | 10 mm | 0 | 0 | 5 mm | 2.5 sec |
| Scenario #5 | 10 mm | 5 mm | 0 | 5 mm | 2.5 sec |
| Scenario #6 | 10 mm | 5 mm | 5 mm | 5 mm | 2.5 sec |
Materials and methods
4D moving lung phantom
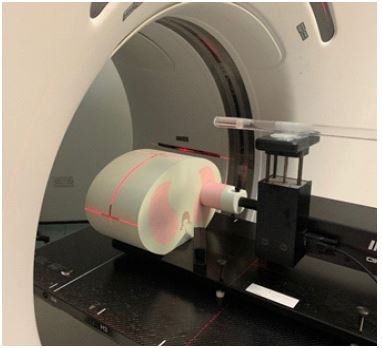
For simulating respiratory motion, a dynamic thorax phantom (CIRS Inc., Norfolk, VA) was used. This phantom features a sphere tumor target in synthetic lung material and mimics the contours of human chests. This sphere (1 cm dia) tumor target is movable in three dimensions. This sphere target was calibrated for this study to move up to 5 mm in anterior-posterior, 5 mm in lateral, and 10 mm in superior-inferior directions as shown in Table 1. The dynamic thorax phantom’s motion range used in this investigationwas selected to resemble random patients’ respiratory movements with varying amplitude and cycle time. Figure 1 depicts the experimental setup for the acquisition of 4DCT images of the moving lung phantom using device less 4D techniques.
Imaging and pre-treatment imaging modalities
The GE Discovery CT 590 RT CT scanner (GE Healthcare) was used for the treatment planning. Prior to the CT simulation, deviceless 4D determines the patient’s breathing cycle length, automatically sorts 4D CT pictures into the required respiratory bins, and prepares intensity projection datasets (like MIP) that are then made available for virtual simulation [14]. The obtained CT scans are divided into ten separate phases, from full inhalation (0%), to full exhalation (50%) and back to full inhalation. The 1.25 mm CT images with the thickest slices are taken. The Monaco treatment planning system (Elekta Oncology Systems, Crawley, UK) version 5.11 was used to contour the acquired 4DCT images. VMAT plan with 1 Arc was created from the Monaco treatment planning system once the virtual target had been contoured. The XVI SymmetryTM technique was then used to confirm the phantom’s motion.
The medical linear accelerator InfinityTM (Elekta Oncology Systems, Crawley, UK) was utilized in this investigation. 4D CBCT images were acquired using XVI SymmetryTM 4.5.4.x (Elekta Oncology Systems, Crawley, UK). The image acquisition parameters were 120 kVp, 4m. As, and 1320 slice frames. The kilo-Voltage (kV) CBCT system is attached to the gantry on both sides, along with a kV X-ray tube and a flat panel. The flat-panel detector’s active area is 410 mm2 by 410 mm2, and the image acquisition matrix’s pixels are 512 x 512. The detector is symmetrically positioned in the FOV’s centerin the small mode of 4D CBCT scanning. 270 x 260 mm2 was the FOV. Additionally, the overall gantry angle from 180 to 20 degrees was used [15,16].
Results and discussion
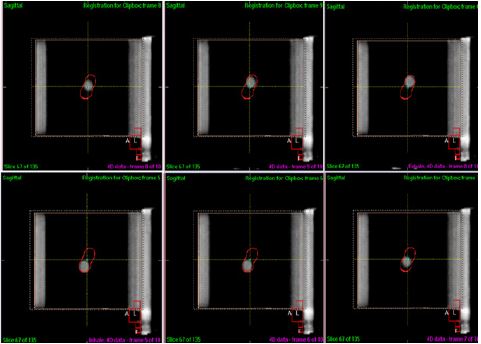
Figure 2 displays an example of 4DCBCT images acquired at different respiratory phases. Table 2 lists the table shift while registering 4DCT and 4DCBCT images. Further, the movement of the sphere within the CIRS dynamic thorax phantom was verified to ensure the target is moving within the ITV as illustrated in Figure 2. Both 4DCT and 4D CBCT cases’ sphere target movements were examined while the 4D moving lung phantom was in use.
From SymmetryTM registration, the effectiveness of the 4D CBCT system for tumors moving with respiration was assessed using the 4D moving lung phantom. The mean table translational shift difference between the 4D CT images acquired pre-set movements and motion assessed using 4D CBCT was determined to be < 0.6 mm in the superior-inferior direction, < 0.5 mm in the lateral direction, and < 10 mm in the anterior-posterior direction as shown in Table 2. Similarly, the table rotational shift between the two image sets were within 5˚ in all direction.
The CIRS 4D moving lung phantom was moved in accordance with the parameters we established for this study. In both the 4DCT and 4D CBCT examples, the measurement error absolute values were within 10 mm in all directions. For example, the greatest measurement error on a 4DCT scan was 0.9 mm in the anterior-posterior direction. This is due to the fact that the 4D moving lung phantom’s pre-set motion range in the anterior-posterior direction was moving in three dimensions as compared to other directions. The relative measurement error was minimal if the motion range of the sphere within the dynamicthorax phantom in 1D and 2D respectively. The 4D moving lung phantom’s continual movement caused an identical measurement inaccuracy in both positive and negative directions.
Table 2: Positional error accuracy during delivery in linear accelerator.
| Translational shift | Rotational Shift | |||||
|---|---|---|---|---|---|---|
| Scenario | Lateral (cm) | Longitudinal (cm) | Vertical (cm) | X (deg) | Y (deg) | Z (deg) |
| #1 | 0.5 ± 0.1 | 0.4 ± 0.2 | 0.9 ± 0.2 | 0.8 ± 0.1 | 0.5 ± 0.2 | 0.0 ± 0.1 |
| #2 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.6 ± 0.2 | 0.0 ± 0.1 | 359.8 ± .02 | 0.0 ± 0.1 |
| #3 | 0.5 ± 0.1 | 0.6 ± 0.1 | 0.4 ± 0.1 | 0.0 ± 0.1 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| #4 | 0.4 ± 0.1 | 0.3 ± 0.1 | 0.8 ± 0.2 | 0.2 ± 0.1 | 359.2 ± 0.1 | 0.0 ± 0.0 |
| #5 | 0.2 ± 0.1 | 0.1 ± 0.0 | 0.8 ± 0.2 | 0.0 ± 0.0 | 0.0± 0.1 | 0.0 ± 0.0 |
| #6 | 0.5 ± 0.1 | 0.1 ± 0.1 | 0.9 ± 0.1 | 0.4 ± 0.1 | 359.5 ± 0.1 | 0.1 ± 0.1 |
Conclusion
Motion-correlated CT, often known as 4DCT, is an effective technique for monitoring internal organ motion. Multiple 3D images representing distinct bins or portions of the respiratory cycle are part of a 4DCT dataset. In radiotherapy, the 4DCT images of the organs that move in response to breathing are frequently employed for image registration. This is a result of the ability to take into account the temporal changes in tumor location during treatment. Our results suggest that 4D CBCT images can also be employed as an effective tool for ensuring accurate image registration prior to treatment and thus reduce measurement error considerably. A more precise evaluation of the effectiveness of 4D CBCT can be demonstrated if additional targets that vary in size, range of movement, shapes, and respiratory motion patterns were included, which is a goal of future studies. Additionally, more precise target localization using 4D CBCT images may be required to increase the efficiency and efficacy of radiotherapy treatment, particularly in cases where tumors move in response to respiration.
References
- Lee TC, et al. Accuracy Comparison of 4D Computed Tomography (4DCT) and 4D Cone Beam Computed Tomography (4DCBCT). 2017; 6: 323-335.
- Ahmed N, et al. Does Motion Assessment with 4-Dimensional Computed Tomographic Imaging for Non-Small Cell Lung Cancer Radiotherapy Improve Target Volume Coverage? Clinical Medicine Insights. Oncology. 2017; 11: 1179554917698461-1179554917698461.
- Cole AJ, et al. Motion management for radical radiotherapy in non-small cell lung cancer. Clin Oncol (R Coll Radiol). 2014; 26: 67-80.
- Yoganathan SA, et al. Magnitude, Impact, and Management of Respiration-induced Target Motion in Radiotherapy Treatment: A Comprehensive Review. Journal of medical physics. 2017; 42: 101-115.
- Keall PJ, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys. 2006; 33: 3874-900.
- Keall P, et al. Potential radiotherapy improvements with respiratory gating. 2002; 25: 1-6.
- Balter JM, et al. Uncertainties in CT-based radiation therapy treatment planning associated with patient breathing. 1996; 36: 167-174.
- Shin HJ, et al. Evaluation of the Elekta Symmetry™ 4D IGRT system by using a moving lung phantom. Journal of the Korean Physical Society. 2015; 67: 260-263.
- Doi Y, et al. Target volume and motion position evaluation of four-dimensional cone-beam CT: comparison with 4D-CT using dynamic thorax phantom. Biomedical Physics & Engineering Express. 2019; 5: 035016.
- Sweeney RA, et al. Accuracy and inter-observer variability of 3D versus 4D cone-beam CT based image-guidance in SBRT for lung tumors. 2012; 7: 1-8.
- Sonke JJ, et al. Respiratory correlated cone beam CT. 2005; 32: 1176-1186.
- Jia X, et al. Four-dimensional cone beam CT reconstruction and enhancement using a temporal nonlocal means method. Medical Physics. 2012; 39: 5592-5602.
- Yan H, et al. Extracting respiratory signals from thoracic cone beam CT projections. Physics in medicine and biology. 2013; 58: 1447-1464.
- Holla R, et al. Investigation of Internal Target Volumes Using Device and Deviceless Four-dimensional Respiratory Monitoring Systems for Moving Targets in Four-dimensional Computed Tomography Acquisition. Journal of medical physics. 2019; 44: 77-83.
- Li J, et al. Evaluation of Elekta 4D cone beam CT-based automatic image registration for radiation treatment of lung cancer. 2015; 88: 20140620.
- Lee S, et al. Impact of scanning parameters and breathing patterns on image quality and accuracy of tumor motion reconstruction in 4D CBCT: A phantom study. Journal of Applied Clinical Medical Physics. 2015; 16: 195-212.