
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
A hair loss pandemic: 19 cases of COVID-19
induced telogen effluvium
Jazmine Nesvik¹*; Colin Smith²; Jonathan Cleaver³; David Cleaver³; Lloyd Cleaver³
1Northeast Regional Medical Center, 315 S Osteopathy, Kirksville, MO, 63501, USA.
2A.T. Still University, 800 W Jefferson St, Kirksville, MO, 63501, USA.
3Cleaver Dermatology, 1316 Country Club Drive, Kirksville, MO, 63501, USA.
*Corresponding Author : Jazmine Nesvik
Northeast Regional Medical Center, 315 S Osteopathy, Kirksville, MO, 63501, USA.
Ph: (320) 491-0988, Fax: (660) 956-7097;
Email: jazminenesvik@atsu.edu
Received : Oct 19, 2022
Accepted : Nov 04, 2022
Published : Nov 11, 2022
Archived : www.jcimcr.org
Copyright : © Nesvik J (2022).
Abstract
As the COVID-19 pandemic continues, the number of patients presenting to dermatology clinics with hair loss is increasing. Little is known about the specifics of telogen effluvium affecting this patient population. We aimed to discover patterns in patient characteristics and clinical course in those with telogen effluvium secondary to COVID-19 infection. We accomplished this by collecting patient history, physical exam, and images on patients presenting to our rural Missouri dermatology clinic with COVID-induced telogen effluvium from July 2020 through March 2021. Of the 19 patients identified, 95% were female, mean age was 56 years, mean onset of hair loss following COVID-19 diagnosis was 2.73 months with a range of 2 weeks to 6 months, and 32% of the patients had been hospitalized from COVID. Furthermore we explore possible pathogenesis behind and special considerations regarding counseling for COVID-induced telogen effluvium. We have concluded that telogen effluvium can occur following both severe and mild COVID-19 infections, may present earlier than TE associated with other causes, and requires unique patient counseling and follow-up given the psychological impact of both COVID-19 and telogen effluvium. Clinicians should be familiar with the unique characteristics of COVID-induced telogen effluvium and how to appropriately manage these patients.
Keywords: Telogen effluvium; Hair loss; Alopecia; COVID-19; SARS-CoV-2; Cytokine storm.
Abbreviations: M: Male; F: Female; HPT: Hair Pull Test; Hair Prep: Trichoscopic evaluation.
Citation: Nesvik J, Smith C, Cleaver J, Cleaver D, Cleaver L, et al. A hair loss pandemic: 19 cases of COVID-19 induced telogen effluvium. J Clin Images Med Case Rep. 2022; 3(11): 2152.
Introduction
Telogen Effluvium (TE) is typically a self-limited diffuse non-scarring alopecia occurring three to four months after the premature transition of hairs from anagen to telogen phase [1]. Apart from the distressing amount of hair loss which can have significant psychosocial implications for patients, TE sufferers are generally asymptomatic and experience resumption of normal hair growth within 6 months. Known triggers for the transition from anagen to telogen include periods of intense physiologic or emotional stress, medications, infections, and ultraviolet light [1]. However, one-third of TE cases lack a definitive cause. A TE trigger with increasing incidence gaining public awareness is COVID-19 infection [2,3]. COVID-19 is caused by a novel RNA virus, SARS-CoV-2, that rapidly spread to pandemic proportions in early 2020. It is the source of a great amount of physiologic and emotional stress that could explain the increasing incidence of telogen effluvium among this patient population [4].
Case series
Beginning in July 2020, our physicians noticed an increase in the number of patients presenting to our rural Northeast Missouri dermatology clinic with the complaint of hair loss. A thorough history and physical examination on each patient led to the diagnosis of telogen effluvium secondary to COVID-19 infection as the cause. We have documented nineteen such patients whose history and physical exam findings will be discussed here and can be referenced in table 1.
All but one patient complained of new diffuse scalp hair thinning (Figures 1 and 2). Patient 4, however, complained of localized thinning along her right frontal scalp, and patient 10 had thinning of his eyebrows in addition to his scalp hair. A thorough history was performed to exclude other causes of hair loss and to identify the likely cause of the telogen effluvium. The patients were screened for concurrent nutritional deficiencies, thyroid disorders, autoimmune conditions, new medications, and sources of emotional and physiologic distress such as recent illness or surgery. All patients included in this case series were found to have had a positive COVID test 2 weeks to 6 months preceding first signs of hair loss. A Hair Pull Test (HPT) was performed on each patient by applying slow traction to approximately 60 hairs on the scalp. Removal of 6 or more hairs constituted a positive HPT. Though not routinely necessary for diagnosis, trichoscopic evaluation was performed on two patients to determine the growth phase of the removed hairs.


Results
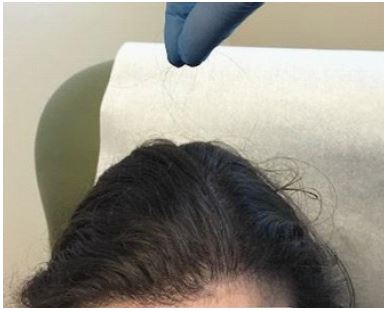
Our patients were 95% female with a mean age of 56 years. The mean time between COVID-19 infection and clinically noticeable hair loss was 2.73 months with a range of 2 weeks to 6 months. 32% of the patients were hospitalized secondary to COVID-19, and 21% stated they were “very sick,” but able to be treated outpatient. Of note, patient 9, who had a history of chronic alopecia areata, presented with diffuse hair thinning in addition to a preexisting hairless patch on her vertex scalp (Figure 4). Patient 11 had preexisting frontotemporal hair loss in addition to new diffuse hair thinning. Patient 4 had localized right frontal scalp thinning only. In terms of diagnostic tests, a positive HPT, pictured in Figure 3, was seen in all but one patient. This patient had already experienced resolution of her telogen effluvium at the time of presentation and had noticeable regrowth. Trichoscopic evaluation performed on two patients revealed clubbed hair roots indicative of telogen hairs.

In addition to reassurance, minoxidil and biotin were offered to all patients as treatment. However, most patients were satisfied with the conservative route of clinic follow-up after being educated on the typical progression of TE and, therefore, did not pursue further treatment. At the time of this article’s submission, all patients have experienced cessation of hair loss, and the majority have observed noticeable regrowth.
Table 1: Patient characteristics and details of telogen effluvium and COVID-19 infection.
| ID | Age, years | Sex | TE latency (months) | Tests | Severity of illness | Hair loss pattern | Relevant comorbidities and medications |
|---|---|---|---|---|---|---|---|
| 1 | 54 | F | 5 | +HPT | Unknown | Diffuse scalp thinning | None |
| 2 | 55 | F | 3 | +HPT, +Hair Prep | High fever, symptomatic; outpatient treatment | Diffuse scalp thinning | History of kidney transplant |
| 3 | 45 | F | 2 | +HPT | Unknown | Diffuse scalp thinning | Hyperthyroidism |
| 4 | 48 | F | 0.5 | +HPT | Severe; 14 days hospitalization | Right frontal scalp thinning | Systemic lupus erythematosus; carvedilol |
| 5 | 66 | F | 1.5 | -HPT | Unknown | Diffuse scalp thinning with regrowth | Lisinopril; note: hair loss lasted 1.5 months |
| 6 | 31 | F | 6 | +HPT, +Hair Prep | Severe; 5 days hospitalization | Diffuse scalp thinning | Hypothyroidism |
| 7 | 68 | F | 3 | +HPT | Moderate symptoms for several weeks; outpatient treatment | Diffuse scalp thinning | None |
| 8 | 43 | F | 2 | +HPT | Severe; hospitalized unknown duration | Diffuse scalp thinning | None |
| 9 | 60 | F | 2 | +HPT | Unknown | Diffuse scalp thinning with one hairless patch on vertex scalp | Alopecia areata, seborrheic dermatitis |
| 10 | 78 | M | 1 | +HPT | Unknown | Diffuse scalp and eyebrow thinning | None |
| 11 | 69 | F | 1 | +HPT | Unknown | Diffuse scalp thinning with existing frontotemporal hair loss | Hypothyroidism, female pattern alopecia |
| 12 | 65 | F | 3 | +HPT | Severe; hospitalized 8 days | Diffuse scalp thinning | None |
| 13 | 71 | F | 1 | +HPT | Moderate symptoms; outpatient treatment | Diffuse scalp thinning | Lisinopril |
| 14 | 69 | F | 4 | +HPT | Unknown | Diffuse scalp thinning | Seborrheic dermatitis |
| 15 | 23 | F | 4 | +HPT | Unknown | Diffuse scalp thinning | None |
| 16 | 70 | F | 6 | +HPT | Severe; hospitalized 7 days | Diffuse scalp thinning | Hypothyroidism |
| 17 | 76 | F | 4 | +HPT | Unknown | Diffuse scalp thinning | None |
| 18 | 57 | F | 1 | +HPT | Moderate symptoms; outpatient | Diffuse scalp thinning | None |
| 19 | 25 | F | 2 | +HPT | Severe; hospitalized 5 days | Diffuse scalp thinning | None |
M: Male; F: Female; HPT: Hair Pull Test; Hair Prep: Trichoscopic evaluation.
Discussion
The incidence of TE has greatly increased over the course of the COVID-19 pandemic to three- to five-fold over pre-pandemic numbers [3,5]. There are a variety of emotional or physiologic factors associated with COVID that could result in TE. It may occur secondary to the inflammatory cytokines released during infection, the febrile state during disease, medications used in treatment, or psychological stress surrounding COVID-19. Di Landro et al. proposed that the most likely explanation is the systemic hyperinflammatory syndrome leading to release of pro-inflammatory cytokines such as IL-6, TNF-alpha, IL-1B, and IFN-gamma, all of which promote catagen development in murine and/or human hair follicles [6].
Alternatively, Rivetti and Barruscotti presented a group of patients with real or perceived worsening in their preexisting telogen effluvium secondary to psychological causes [7]. The stress of contracting COVID-19 and its consequences along with the loneliness of isolation led to new or worsening anxiety and depression for many individuals. Rivetti and Barruscotti highlighted the importance of regular follow-up and psychological support for this subset of patients.
Our case series demonstrates the benefit of educating patients on the pathophysiology of the disease and its self-limited nature along with scheduling regular follow-up and providing psychological support. The majority of our patients were satisfied with this approach and did not pursue further treatment options. As suggested by Rivetti and Barruscotti, frequent follow-ups using telehealth could be incorporated into our patient management.
The majority of TE cases in this series were seen in patients who had not been hospitalized for their infection (68%) [2,5]. This indicates that even mild COVID-19 infection can trigger the development of TE. Alternatively, this could mean that psychological stressors are playing a larger role than the physiological burden of the disease. Based on our study, it is not apparent whether severity of illness led to a faster onset of telogen effluvium, but this could be explored in future studies.
Our study confirms findings seen in prior COVID-19 induced TE studies and adds valuable information to current literature. The average age of our patients is similar to that seen in other studies: 56 years here versus 55 in Mieczkowska et al.’s study [8]. COVID-induced TE is also seen more commonly in females: 95% in our study compared to 100% and 90% in other studies [8,9]. Furthermore, our study had the benefit of all patients having confirmed positive COVID tests and all were seen in-person versus via telemedicine compared with the studies by Cline et al. and Mieczkowska et al., respectively [8,10].
Limitations of our study include potential confounding variables such as preexisting hair loss disorders in addition to comorbid conditions and medications (such as angiotensin-converting enzyme inhibitors and beta-blockers) associated with telogen effluvium (Table 1) [1]. However, none of these causative medications were initiated within 6 months prior to the start of TE, and the comorbid conditions were chronic. Thus, these are unlikely to explain the acute onset of TE seen in our patients.
COVID-19 is also considered to infrequently cause thyroid dyscrasia [11]. As a well-studied trigger of TE, the infection-related thyroid disturbance may have exacerbated the TE in the four patients with underlying thyroid disorders. It could have also elicited new onset hyper- or hypothyroidism in those without previous thyroid dysfunction. Additionally, the increase in hair loss complaints could be explained by the increased publicity on hair loss as a delayed effect of COVID-19. Lastly, this series is limited by its single-center design and small case number.
Conclusion
Knowing that TE is a potential result of COVID-19 infection, physicians should incorporate screening for a history of COVID-19 when interviewing a TE-patient. Patients with a history of COVID-19, particularly females, should be counseled about this potential post-infectious manifestation and informed that TE can present weeks to months following infection. This is potentially earlier than telogen effluvium attributable to other causes. Given the profound psychological impacts of both telogen effluvium and COVID-19, it is imperative that COVID-induced TE patients be reassured that hair loss will cease and regrowth will ensue. Clinicians should schedule patients for regular follow-up, including via telehealth, to reduce the stress of coming to clinic and provide psychological support to these patients. Consideration could also be given to checking thyroid labs because of rare COVID-induced thyroid dyscrasias.
Future studies could expand upon the findings of this case series. The pathogenesis behind COVID-induced TE could be further elucidated. The association between TE and treatments used for COVID-19 should be explored. Finally, learning more about the relationship between severity of COVID-19 symptoms and time to TE onset as well as the time to resumption of hair growth could improve patient counseling.
References
- Asghar F, Shamim N, Farooque U, Sheikh H, Aqeel R, et al. Telogen Effluvium: A Review of the Literature. Cureus. 2020; 12: e8320.
- Rizzetto G, Diotallevi F, Campanati A, Radi G, Bianchelli T, Molinelli E, et al. Telogen effluvium related to post severe Sars-Cov-2 infection: Clinical aspects and our management experience. Dermatol Ther. 2021; 34: e14547.
- Kutlu Ö, Metin A. Relative changes in the pattern of diseases presenting in dermatology outpatient clinic in the era of the COVID-19 pandemic. Dermatol Ther. 2020; 33: e14096.
- Listings of WHO’s Response To COVID-19. World Health Organization, World Health Organization. 29 Jan. 2021, www.who.int/news/item/29-06-2020-covidtimeline.
- Domínguez Santás M, Haya Martínez L, Fernández Nieto D, Jiménez Cauhé J, Suárez Valle A, Díaz Guimaraens B, et al. Acute telogen effluvium associated with SARS-CoV-2 infection. Aust J Gen Pract. 2020; 49: 10.31128/AJGP-COVID-32.
- Di Landro A, Naldi L, Glaser E, Paus R, Tosti A, et al. Pathobiology questions raised by telogen effluvium and trichodynia in COVID-19 patients. Exp Dermatol. 2021; 30: 999-1000.
- Rivetti N, Barruscotti S. Management of telogen effluvium during the COVID-19 emergency: Psychological implications. Dermatol Ther. 2020; 33: e13648.
- Mieczkowska K, Deutsch A, Borok J, Guzman A, Fruchter R, Patel P, et al. Telogen effluvium: A sequela of COVID-19. Int J Dermatol. 2021; 60: 122-124.
- Olds H, Liu J, Luk K, Lim HW, Ozog D, Rambhatla PV, et al. Telogen effluvium associated with COVID-19 infection. Dermatol Ther. 2021; 34: e14761.
- Cline A, Kazemi A, Moy J, Safai B, Marmon S, et al. A surge in the incidence of telogen effluvium in minority predominant communities heavily impacted by COVID-19. J Am Acad Dermatol. 2021; 84: 773-775.
- Speer G, Somogyi P. Thyroid complications of SARS and coronavirus disease 2019 (COVID-19). Endocr J. 2021; 68: 129-136.