
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Medium and large-sized arteries thrombosis in patients with COVID-19
Alia Fazaa; Yosr El Mabrouk*; Saoussen Miladi; Hiba Bousaa; Leila Souabni; Yasmine Makhlouf; Selma Chekili; Selma Kassab; Kaouther Ben Abdelghani; Ahmed Laatar
Rheumatology Department, Faculty of Medicine of Tunis, Tunis El Manar University, Mongi Slim Hospital, La Marsa, Tunisia.
*Corresponding Author : Yosr El Mabrouk
Rheumatology Department, Faculty of Medicine of Tunis, Tunis El Manar University, Mongi Slim Hospital, La Marsa, Tunisia.
Email: yosr.elmabrouk@gmail.com
Received : Oct 18, 2022
Accepted : Nov 07, 2022
Published : Nov 14, 2022
Archived : www.jcimcr.org
Copyright : © Mabrouk YE (2022).
Abstract
Recent epidemiological studies have reported that hypercoagulopathy is a well-documented symptom of SARS-CoV-2 infection, particularly in more severe cases requiring admission to the critical care unit. We report here the clinical and imaging features of three patients with SARS-CoV-2 infection who developed acute thrombosis of the abdominal aorta, the superior mesenteric artery and cerebral arteries, respectively. The extensive manage of thrombo inflammation is necessary to enhance the outcome of this disease. It would be suitable to retain anticoagulant remedy after discharge, mainly in sufferers with severe disease and a poor prognosis.
Keywords: Thrombosis; Covid; Arteries; Infection; Hypercoagulopathy.
Citation: Fazaa A, Mabrouk YE, Miladi S, Bousaa H, Souabni L, et al. Medium and large-sized arteries thrombosis in patients with COVID-19. J Clin Images Med Case Rep. 2022; 3(11): 2155.
Introduction
COVID-19 is a viral contamination, like wise described as intense acute breathing syndrome [1]. It has been suggested that hypercoagulopathy has an essential vicinity with inside the excessive mortality rate. It is a well-documented symptom of SARS-CoV-2 infection, particularly in more severe cases requiring admission to the critical care unit [2]. The etiopathogenic processes are still being unraveled, despite the fact that it has been linked to endothelial dysfunction, excess thrombin and fibrinolysis inhibition [1]. The pulmonary embolism is one of the most common thrombotic consequences as well as myocardial infarction [2].
Management of acute thrombosis with in the placing of this pandemic disorder poses particular challenges, along with the want to hold incredible care with restricted resources, whilst on the identical time stopping contamination unfold to patients and physicians [2].
Here, we report 3 cases of arterial thrombosis in COVID-19 infected patients.
Case 1
A 55-year-old man with a history of asthma, was admitted with cough, fever, asthenia evolving for twelve days, complicated by dyspnea ten days later. The rapid covid screening test was positive. Oxygen saturation at hospital arrival was 97% with 4 liters of oxygen therapy. Vital signs were stable.
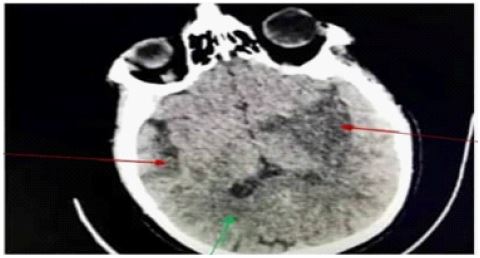
Neurological examination was normal. A blood analysis showed lymphocytopaenia (520/ mm³), a CRP of 100 mg/l, D-dimers of 1126 μg/L, hepatic cytolysis (AST/ALT of 52/53 UI/l). The patient received 40 mg x 2/day subcutaneous low molecular weight heparin and 6 mg/day dexamethasone. Six days following admission, the patient complained of neuralgia-like pain and an altered state of consciousness. On physical examination, he was aphasic, he had right hemiplegia and deviation of labial commissures. A brain scan revealed no signs of a recent ischemic or hemorrhagic stroke. Repeat CT angiography after 3 hours showed left middle cerebral artery thrombosis. Then, we started treatment with 60 mg x 2/day subcutaneous low molecular weight heparin and 100 mg/day acetylsalicylic acid. On day 11 of hospitalisation, a control brain scan showed an ischemic stroke constituted in the territories of the right and left sylvian arteries (Figure 1).
Case 2
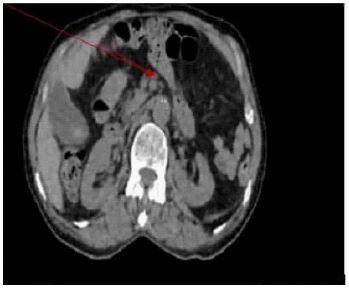
A 84-year-old woman with a history of hypertension and atrial fibrillation, was admitted with six days of dry cough, vomiting and abdominal pain. Oxygen saturation at hospital arrival was 87% and improved to 96% with 5 liters of oxygen therapy. She had a tachycardia at 100 beat per minute. Blood pressure was normal. She was apyretic. Neurological examination was normal. The rapid covid screening test was positive. A chest scan revealed multiple bilateral lung opacities compatible with covid-19 infection with widespread involvement (50%), blood analysis showed a CRP of 200 mg/l, lymphocytopaenia (920 per mm³), hepatic cytolysis (AST/ALT of 82/70 UI/l) and creatinine clearance of 42 ml/mn. The patient received 1 g x 3/ day of cefotaxime, 500 mg x 2/ day of levofloxacin, 40 mg x 2/day of subcutaneous low molecular weight heparin and 6 mg/day of dexamethasone. On day 3 of hospitalisation, the patient developed increasing diffuse abdominal pain with local heat. She was febrile at 39°C. The abdomen was tympanitic, sensitive and painful. An abdominal scan showed severe stenosis of the Superior Mesenteric Artery (SMA) at 70% (Figure 2). She received 100 mg/ day acetylsalicylic acid, 40 mg/day of atrovastatin, 400 mg x 2/ day of pentoxifylline and 200 mg x 3/day of naftidrofuryl with good progress.
Case 3
A 61-year-old man, with no past medical history, attended the emergency department due to progressive dyspnea and fever evolving for a week. He was tested positive for COVID-19, based on the Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) test performed via nasopharyngeal swab. The patient reported no other symptoms. Oxygen saturation at hospital arrival was 83% and improved to 94% with high-flow oxygen therapy (10 liters). Vital signs were stable. Neurological examination was normal. A chest scan revealed bilateral interstitial pneumonia with 80% parenchymal involvement. A blood analysis showed lymphocytopaenia (780 per mm³), a C-Reactive Protein (CRP) of 165 mg/l and Hepatic Cytolysis (AST/ALT of 86/54 UI/L). Concerning therapeutic management, the patient received 2 × 40 mg/day subcutaneous low molecular weight heparin, 4 mg/day dexamethasone and 2 × 1 g/day intravenous ceftriaxone. On day 6 of hospitalisation, the patient reported a severe acute pain in the lower limbs. On examination, both limbs were cold. Femoral pulses were abolished. An emergency Computed Tomography (CT) angiography of the lower limbs showed total stenosis of the abdominal aorta in its terminal portion extended over approximately 30 mm to the internal and external common iliac arteries. Total popliteal artery stenosis was also observed (Figure 3).
Treatment with unfractionated heparin at a dose of 180 mg was started, associated to 250 mg acetylsalicylic acid. Ten hours later the patient was found to have pulseless electrical activity and he passed away after a 10-minute of cardiopulmonary resuscitation.
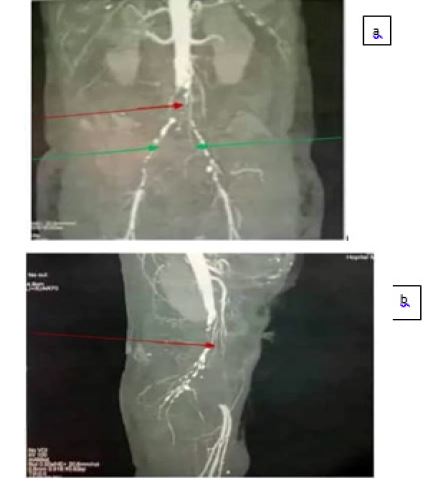
b: Total popliteal artery stenosis (red arrow).
Discussion
We report here the clinical and imaging features of three patients with SARS-CoV-2 infection who developed acute thrombosis of the cerebral arteries, the superiormesenteric artery and the abdominal aorta, respectively. Two of them had severe SARS-CoV-2 infection with the exception of case 1.
As known, the SARS-CoV-2 infection causes systemic Inflammation and promotes a hypercoagulable state especially in more severe cases in which patients are admitted to the intensive care units [1].
Most publications have highlighted the frequency of venous thrombosis and pulmonary embolism complicating COVID-19. Arterial thromboembolic complications are less common [3,4].
The exact mechanism for thrombosis in COVID-19 is unknown. Hypoxia, inflammatory mediators, thrombocythemia, immobilization and liver injury secondary to angiotensin-converting enzyme 2 receptor expression are the proposed mechanisms [1]. Moreover, recent studies have shown that the virus targets endothelial cells which results in endothelial dysfunction [5]. In our cohort, the most likely etiopathogenic processes are hypoxia, inflammation (increased CRP), hepatic cytolysis and immobilization. The relationship between acute infection and stroke is complex and it was demonstrated for many types of bacterial and viral infections. An increased risk of stroke was documented after respiratory infections, including influenza, and the risk was highest within the first week [6]. Infection with COVID-19 can also accelerate the progression of acute stroke [7]. A study reported that 16 days after onset of SARS-CoV-2 infection, a 64-year-old man with acute respiratory distress syndrome and a history of atherosclerotic disease developed an ischemic stroke with symptoms of hemiparesis [8]. This was the case of our first patient who developed hemiplegia 18 days after the onset of the infection. In the study of Li and al, the median duration from first symptoms of Covid-19 to cerebrovascular disease were 12 days in eleven patients with severe forms. They were more likely to have cardiovascular risk factors, including hypertension, diabetes and increased inflammatory response [7]. In the cases reported by Tunc and al, the mean time from Covid-19 symptom onset to the diagnosis of stroke was 2 days [9]. Therefore, we must retain the diagnosis of COVID-19 infection as soon as possible to initiate preventive anticoagulant treatment. However, the thrombotic risk remains elevated even with standard anticoagulation therapy, particularly in patients admitted to intensive care units, due to cytokin storm, raising the question of optimal doses of agents for anticoagulation [10,11].
There are only a few case reports of COVID-19-related SMA thrombosis [1]. Several studies reported that D-dimer tends to rise early in mesenteric ischemia and has a sensitivity of 95% in diagnosing intestinal ischemia [1,12]. In COVID-19, a high CRP level is associated with the disease severity [13]. This was the case of our second patient who had an elevated CRP. CT angiography is the best diagnostic modality and has a sensitivity and specificity of 89.4% and 99.5%, respectively, in diagnosing acute mesenteric ischemia [14].
The case of an acute thrombosis on aortic graft represents an extreme complication. This pathology has more severe circulatory consequences. A retrospective study of 12630 patients with COVID-19 identified 49 patients with arterial thromboembolism, including 35 with lower extremity ischemia (aortoiliac, femoral above knee and popliteal below knee) [15]. Although hypertension and other comorbidities are reported as present in aortic thrombosis cases, our patient did not have known cardiovascular disease or a history of thrombosis. COVID-19 disease itself creates a hypercoagulant state, independently of concomitant diseases or predisposing conditions for the formation of large-vessel thrombosis [16].
Although a thrombosis at the aortic level is rare, it would be appropriate to continue anticoagulant therapy after discharge, especially in patients with severe disease and poor prognosis criteria (such as high D-dimer or high fibrinogen) [4].
Finally, management of COVID-19 patients should include regular monitoring of a coagulation panel, as well as platelet counts and D-dimer levels, as these parameters can be helpful in determining prognosis and titering dosages of anticoagulation agents in these patients [17].
Conclusion
SARS-Cov2 infection can lead to serious illnesses with a risk of developing thrombotic complications associated with an increased risk of morbidity and mortality. The extensive manage of thromboinflammation is necessary to enhance the outcome of this disease. It would be suitable to retain anticoagulant remedy after discharge, mainly in sufferers with severe disease and a poor prognosis. However, the thrombotic risk remains high even with standard anticoagulation therapy, raising the question of optimal doses.
References
- Amaravathi U, Balamurugan N, Muthu Pillai V, Ayyan SM. Superior Mesenteric Arterial and Venous Thrombosis in COVID-19. J Emerg Med. 2021; 60: e103-e107.
- Klok FA, Kruip MJHA, van der Meer NJM. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020; 191: 145–147.
- Azouz E, Yang S, Monnier Cholley L, Arrivé L. Systemic arterial thrombosis and acute mesenteric ischemia in a patient with COVID-19. Intensive Care Med. 2020; 46: 1464-1465.
- Borulu F, Erkut B. Severe Aortic Thrombosis in the Early Period after COVID-19: Two Cases. Ann Vasc Surg. 2021; 73: 114-118.
- Deng H, Tang TX, Chen D, Tang LS, Yang XP, Tang ZH, et al. Endothelial Dysfunction and SARS-CoV-2 Infection: Association and Therapeutic Strategies. Pathogens. 2021; 10: 582.
- Morassi M, Bagatto D, Cobelli M, D’Agostini S, Gigli GL, Bnà C, et al. Stroke in patients with SARS-CoV-2 infection: case series. J Neurol. 2020; 267: 2185-2192.
- Li Y, Li M, Wang M, Zhou Y, Chang J, Xian Y, et al. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc Neurol. 2020; 5: 279-284.
- Goldberg MF, Goldberg MF, Cerejo R, et al. Cerebrovascular disease in COVID-19. AJNR Am J Neuroradiol 2020. 10.3174/ajnr.A6588. [Epub ahead of print: 14 May 2020]
- Tunç A, Ünlübaş Y, Alemdar M. Coexistence of COVID-19 and acute ischemic stroke report of four cases. J Clin Neurosci. 2020. 10.1016/j.jocn.2020.05.018.
- Patel SD, Kollar R, Troy P, Song X, Khaled M, Parra A, et al. Malignant Cerebral Ischemia in A COVID-19 Infected Patient: Case Review and Histopathological Findings. J Stroke Cerebrovasc Dis. 2020; 29: 105231.
- Edhem Unver and et al. Case report: Cerebral thromboembolism in an unconscious COVID-19 patient in intensive care. Pan Afr Med J. 2021; 38: 373.
- Montagnana M, Danese E, Lippi G. Biochemical markers of acute intestinal ischemia: Possibilities and limitations. Ann Transl Med. 2018; 6: 341.
- Gong J, Dong H, Xia QS, et al. Correlation analysis between disease severity and inflammation-related parameters in patients with COVID-19: A retrospective study. BMC Infect Dis. 2020; 20: 963.
- Henes FO, Pickhardt PJ, Herzyk A, et al. CT angiography in the setting of suspected acute mesenteric ischemia: prevalence of ischemic and alternative diagnoses. Abdom Radiol N Y. 2017; 42: 1152–1161.
- Etkin Y, Conway AM, Silpe J, Qato K, Carroccio A, Manvar-Singh P, et al. Acute arterial thromboembolism in patients with COVID-19 in the New York City area. Ann Vasc Surg. 2021; 70: 290-294.
- Yarımoglu R, Yarımoglu S, Tastan H, Erkengel HI, et al. Acute infrarenal abdominal aortic occlusion in a patient with COVID-19. Ann Saudi Med. 2021; 41: 392-395.
- Cheung S, Quiwa JC, Pillai A, Onwu C, Tharayil ZJ, Gupta R, et al. Superior Mesenteric Artery Thrombosis and Acute Intestinal Ischemia as a Consequence of COVID-19 Infection. Am J Case Rep. 2020; 21: e925753.