
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of mesonephric adenocarcinoma of the uterine corpus in a woman with postmenopausal bleeding
Seongeun Bak1*; Heekyoung Song2; Soo Young Hur1
1Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, the Catholic University of Korea, Seoul 06591, South Korea.
2Department of Obstetrics and Gynecology, Incheon St. Mary’s Hospital, College of Medicine, the Catholic University of Korea, Incheon 21431, South Korea.
*Corresponding Author : Seongeun Bak
Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222, Banpo-daero, Seocho-gu, Seoul 06591, Korea.
Email: newsseong@gmail.com
Received : Sep 22, 2022
Accepted : Nov 08, 2022
Published : Nov 15, 2022
Archived : www.jcimcr.org
Copyright : © Bak S (2022).
Abstract
Background: Mesonephric Adenocarcinoma (MNA) is a rare malignant tumor to arise from mesonephric remnants occurring in the uterine cervix and, less likely the corpus. Only about 30 cases of MNA arising from uterine corpus had been reported in the literature and its clinical symptoms, treatment method were not known very well. So we reported our case, MNA of uterine corpus, and reviewed clinical symptoms of it.
Case presentation: A 66-year-old woman (gravida 1, reaching menopause in her 55-year age) was admitted to our hospital for post-menopausal bleeding. Transvaginal Sonogram (TVS) demonstrated 5 cm sized with mixed echogenic mass and 3 cm sized calcified mass, probably uterine myoma, sere seen in intramural layer and endometrial thickness was measured about 0.3 cm. Endometrial and cervical cytology was also done, and the result of endometrial samples was proliferative endometrium with no other abnormal findings. After 1 year later, at her follow up visit, the size of intramural myoma was growing up to 10 cm by TVS. Pelvic magnetic resonance imaging revealed intramural myoma increased of its size with hemorrhage, and tumor marker was higher than the normal range (CA125: 1037.1 U/ml, CA 19-9: 159.21 U/ml). Total laparoscopic hysterectomy with bilateral salpingo-oophorectomy was done. The final pathology was MNA arising from uterine corpus with myometrial and uterine serosa invasion, and adjuvant chemotherapy, palliative radiotherapy for pain control. Was done. There was recurrent lesion 1 year after completion of adjuvant chemotherapy. The patient is undergoing second-line chemotherapy.
Conclusion: A case of MNA is uncommon and malignancy was not detected by conventional diagnostic method. Therefore, gynecologic oncologists should be recognized in to avoid misdiagnosis.
Citation: Bak S, Song H, Hur SY. A case of mesonephric adenocarcinoma of the uterine corpus in a woman with postmenopausal bleeding. J Clin Images Med Case Rep. 2022; 3(11): 2156.
Introduction
Mesonephric Adenocarcinoma (MNA) is a rare malignant tumor that originates from mesonephric remnants of the female genital tract [1]. Mesonephric duct, also known as Wolffian duct, is one of two primitive reproductive ducts, the other one is paramesonephric (Müllerian) duct. During embryonic development Müllerian ducts become the female reproductive ducts, while the mesonephric ducts degenerate [2]. Generally, MNA is considered that it is originated from remnant mesonephric duct. Hyperplastic lesions derived from mesonephric remnants are not common proliferations. The remnants of mesonephric duct to arise from the ovarian hilum, the broad ligament, the mesosalpinx, the lateral wall of the vagina, or the uterine cervix [3]. So, MNAs in the female genital tract occur commonly in the cervix, vagina, and less frequently in the upper female genital tract such as uterine body.
Several studies have demonstrated inconsistent findings and no large studies have examined the mesonephric adenocarcinoma because of rarity. In this report, we report herein the case of a 66-year-old woman diagnosed with a mesonephric adenocarcinoma arising in the uterine corpus-endometrium. That cancer recurred with vagina of the patient after 9 months since the last cycle of chemotherapy. By reviewing this disease showing an aggressive pattern, the clinical characteristics are identified and important factors in diagnosis and treatment are summarized.
Case presentation
Patient information, clinical findings
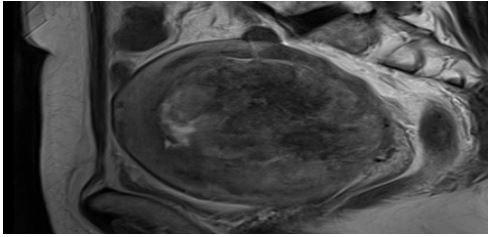
A 66-year-old woman (gravida 1, reaching menopause in her 55-year age) was admitted to Seoul Saint Mary’s hospital with post-menopausal vaginal bleeding that occurred a week ago, and there was no underlying disease. Transvaginal sonogram demonstrated 5 cm sized with mixed echogenic mass and 3 cm-sized calcified mass, probably uterine myoma, were seen in intramural layer and endometrial thickness was measured about 0.3 cm (Figure 1). Endometrial and cervical cytology was also done, and the result of endometrial samples was proliferative endometrium with no other abnormal findings. After 1 year later, her follow up visit, she complained of general abdominal pain, the size of intramural myoma was growing up to 10 cm by transvaginal sonogram. Pelvic magnetic resonance imaging revealed intramural myoma increased of its size with hemorrhagic degeneration (Figure 2), and tumor marker was higher than the normal range. (CA125: 1037.1 U/ml, CA 19-9: 159.21 U/ml)

Initial treatment
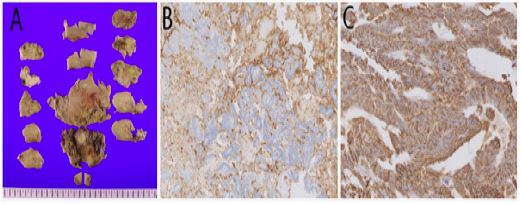
Since the possibility of malignancy of the uterine lesion could not be excluded, we planned to do total hysterectomy with bilateral salpingo-oophorectomy. On the chest X-ray performed before surgery, a micronodule was observed on the lower left side, and chest CT was performed. It was planned to determine whether malignancy was found after uterine surgery because the micronodules seen on CT were found to be metastasizing leiomyomas. The surgery was done by laparoscopy. During operation, patient’s status was stable. Several types of immunostaining were performed by pathologists to differentiate between primary adenocarcinoma of the uterine corpus and metastatic carcinoma (Figure 3). The final pathology was mesonephric adenocarcinoma arising from endometrium with myometrial and uterine serosa invasion, so FIGO staging was IIIA. Depending on the National Comprehensive Cancer Network (NCCN) guideline of uterine neoplasms, we applied chemotherapy, consisting of paclitaxel and carboplatin. After 1st cycle of chemotherapy, the patient complained of pain. We already knew PET-CT finding about concurrent presacral invasion from lower sacral bone metastasis. So, patient got palliative ERT on the Right acetabular region and sacrum. Afterwards, she continued to get chemotherapy, total 9 cycle of carboplatin-paclitaxel. Subsequent to those treatments, the patient visited outpatient clinic regularly for follow-op examinations.
Recurrent treatment
At 8 months post last chemotherapy, she visited outpatient clinic, complaining of vaginal spotting. We could find lesion presumed recurrent cancer at vagina, did biopsy using colposcopy. The pathologic result of biopsy was recurrent mesonephric adenocarcinoma. At that time, the patient’s CA125 was 6.55 U/ml and CA19 9 was 10.51 U/ml, both levels were in normal range. The computed tomography image at Seoul Saint M, at that time, showed multiple variable sized nodules scattered in both lungs supposed to be metastasis, and nodular wall thickening of vagina. So, we started 2nd line chemotherapy composed of cisplatin-doxorubin. Previous chemotherapy ended 8 months ago, we tried regimen including platinum, and the patient was afraid of neuropathic pain, so we started with cisplatin-doxorubicin. The latest 4th chemotherapy was done on 27th of August, 2022. Response evaluation will be done after 6th chemotherapy.
Discussion
When meeting post menopausal patients complaining of vaginal spotting at outpatient clinic, we usually think of diseases such as atrophic endometrium, endometrial polyp. Therefore we have to ask questions about symptoms for differential diagnosis. In addition to symptoms, we should not miss the situation about lifestyle, medications, and food by asking appropriate questions to the patient. Because some postmenopausal patients take estrogen-contatining foods to improve their quality of life, which can also cause vaginal spotting or bleeding. Above all else, we should not overlook the possibility of cancer. In postmenopausal women with symptoms of vaginal spotting or bleeding, follow-up evaluation is essential to ensure they receive appropriate treatment of any precancerous lesion of the endometrium [4].
As in this case, even if the result is confirmed as benign when performing endometrial biopsy, there is a possibility that the diagnosis through endometrial biopsy may not be complete or lesions may develop after that procedure. Therefore, closed monitoring, additional imaging such as MRI are necessary if vaginal spotting or bleeding continues even after endometrial biopsy. An aggressive treatment plan such as considering hysterectomy is required depending on risk factors, underlying disease, and symptom patterns.
The main complains of the patients differed depending on the origin of MNA. As mentioned above, in the case of uterine origin, the main complaint was vaginal bleeding, and in the case of ovarian origin, symptoms commonly seen in ovarian cancer patients such as abdominal distention and indigestion were reported [5,6].
Elevation of CA125 was not commonly accompanied, but it was often accompanied in advanced stage patients. Therefore, vaginal spotting in corpus uterine MNA may be a characteristic symptom and CA125 may not be elevated [7].
According to the literature, hysterectomy and BSO were performed in both premenopausal and postmenopausal women. And lymph node dissection was performed according to the clinician’s criteria for each case [5]. In this case, initial impression taken into consideration was uterine sarcoma and there were no enlarged lymph nodes in magnetic resonance imaging study. Therefore, hysterectomy and BSO was done without pelvic lymph node dissection through minimal invasive surgery using laparoscopy for this patient. We took specimen out using endo-bag.
When MNA recurred in this patient, the location of the lesion was located in the upper third of the vagina, slightly distant from the stump. During physical examination of a patient complaining of vaginal bleeding, careful examination is required so as not to miss these lesions. In this case, radiation-induced lesions may occur due to radiation therapy, so a biopsy was performed for differential diagnosis, and recurrence of MNA was confirmed. Therefore, it is necessary to check the symptoms complained of by the patient visiting the outpatient clinic, and in the case of malignancy, it is necessary to check whether there is a recurrence so that the patient can not delay the treatment [3].
Considering radiation therapy for MNA treatment, it can be performed for symptom control in bone metastasis or advanced stages [8], and in this patient, the pain index before and after radiation therapy was lowered from radiation therapy start day.
Although MNA is rare malignancy, treatment guidelines have not been established, but since it shows an aggressive progression [9], it should be kept in mind during differential diagnosis, in particular, it can be suspected if the mass-like lesion, CA125, accompanied by vaginal spotting is elevated. Even if malignancy is not diagnosed after endobiopsy, it is also necessary to educated patients so that they can visit a hospital if accompanied by vaginal bleeding [4].
References
- Ferry JA, RE Scully. Mesonephric remnants, hyperplasia, and neoplasia in the uterine cervix. A study of 49 cases. Am J Surg Pathol. 1990; 14: 1100-1111.
- Pors J, et al. Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study. Am J Surg Pathol. 2021; 45: 498-506.
- Montagut C, et al. Activity of chemotherapy with carboplatin plus paclitaxel in a recurrent mesonephric adenocarcinoma of the uterine corpus. Gynecol Oncol. 2003; 90: 458-461.
- Colombo N, et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann Oncol. 2016; 27: 16-41.
- Na K, Kim HS. Clinicopathologic and Molecular Characteristics of Mesonephric Adenocarcinoma Arising From the Uterine Body. The American Journal of Surgical Pathology. 2019; 43: 12-25.
- Xie C, Chen Q, Shen Y. Mesonephric adenocarcinomas in female genital tract: A case series. Medicine (Baltimore). 2021; 100: e27174.
- Ando H, et al. Mesonephric adenocarcinoma of the uterine corpus with intracystic growth completely confined to the myometrium: A case report and literature review. Diagnostic Pathology. 2017; 12.
- Mueller I, et al. Mesonephric adenocarcinoma of the vagina: Diagnosis and multimodal treatment of a rare tumor and analysis of worldwide experience. Strahlenther Onkol. 2016; 192: 668-671.
- Montalvo N, Redrobán L, Galarza D. Mesonephric adenocarcinoma of the cervix: A case report with a three-year follow-up, lung metastases, and next-generation sequencing analysis. Diagnostic Pathology. 2019; 14.