
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Coexistence of pancreatic lymphoepithelial cyst and uroepithelial carcinoma: A rare case report
Ufuk Avcıoğlu*; Müge Ustaoğlus
Department of Gastroenterology, Faculty of Medicine, Ondokuz Mayıs University, 55200 Atakum, Samsun, Turkey.
*Corresponding Author : Ufuk Avcıoğlu
Department of Gastroenterology, Faculty of Medicine, Ondokuz Mayıs University, 55200 Atakum, Samsun Turkey.
Tel: +90 362 3121919- 2711,
Fax: + +90 362 457 6041;
Email: ufukavcioglu@yahoo.com
Received : Oct 26, 2022
Accepted : Nov 10, 2022
Published : Nov 17, 2022
Archived : www.jcimcr.org
Copyright : © Avcıoğlu U (2022).
Abstract
Pancreatic Lymphoepithelial Cysts (PLECs) are very rare and benign lesions of the pancreas. They are commonly detected incidentally during radiological examinations. Proper diagnosis of Pancreatic Cystic Lesions (PCLs) is very important, and physicians should be aware of the different types of cystic lesions and their characteristics before the treatment choice. However, preoperative diagnosis of PLECs, which have no malignant potential and rarely symptomatic or cause complication, are difficult due to nonspecific imaging and the presence of cytological features that overlap with other PCLs. Although many methods are used to avoid unnecessary surgery, most cases are diagnosed after surgery. We report a very rare case of PLEC with coexisting uroepithelial carcinoma.
Keywords: Pancreatic cystic lesion; Lymphoepithelial cysts; Uroepithelial carcinoma.
Citation: Avcıoğlu U, Ustaoğlus M. Coexistence of pancreatic lymphoepithelial cyst and uroepithelial carcinoma: A rare case report. J Clin Images Med Case Rep. 2022; 3(11): 2160.
Introduction
Cystic Lesions of the Pancreas (PCLs) were extremely rare. Today, PCLs are commonly seen due to the more frequent use of imaging methods such as Computed Tomography (CT) and Magnetic Resonance Imaging (MRI). The reported prevalence rate of PCLs varies from 0.7 % to 38% in the literature [1-3]. PCLs include a broad spectrum of lesions and can be categorized into neoplastic and nonneoplastic. They differ extensively in their clinical behavior, malignant potential, and prognosis. Therefore, proper diagnosis of pancreatic cystic lesions is very important, and physicians should be aware of the different types of cystic lesions and their characteristics before treatment choice [1,2]. Pancreatic Lymphoepithelial Cysts (PLECs) are very rare, benign lesions of the pancreas, and no recurrence or malign transformation have been reported up to now. They are mostly detected incidentally during radiological examinations [4]. Although there is an increased interest in preoperative diagnosis of PCLs, most cases are diagnosed after surgery [5]. Therefore, the confirmation for the diagnosis of PCLs inappropriate stage is very important. The preoperative diagnosis of these patients prevents the morbidity and mortality caused by the unnecessary surgical intervention [1,6,7]. We report a very rare case of the coexistence of pancreatic lymphoepithelial cyst and uroepithelial carcinoma that is diagnosed postoperatively.
Case report
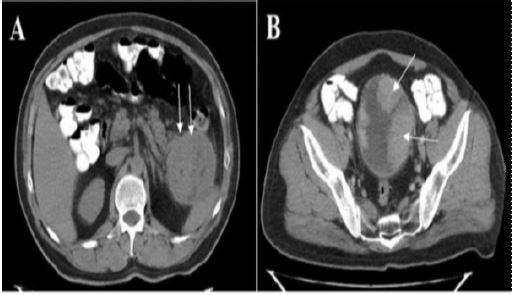
A 56-year-old man presented with hematuria. During sonographic imaging, there were multiple polypoid solid masses on the bladder wall. A solid mass measuring approximately 8 cm located at the pancreatic tail was incidentally determined. The patient did not have any complaints related to the pancreatic lesion. Physical examination was unremarkable. In routine blood tests, Carbohydrate Antigen (CA 19-9) and Carcinoembryonic Antigen (CEA) levels were within normal limits. Contrast Enhanced Tomography (CECT) revealed a mass lesion with a diameter of 8 cm as a well-defined lesion with peripheral enhancement and small internal macroscopic fatty foci. There was no dilatation of the pancreatic canal or the common bile duct.The lesion was not typical for pancreatic adenocarcinoma or islet cell tumor. There were polypoid enhancing masses on the bladder wall, one of which caused lobulation and angulation of the bladder wall that was consistent with wall/serosal invasion (Figure 1).
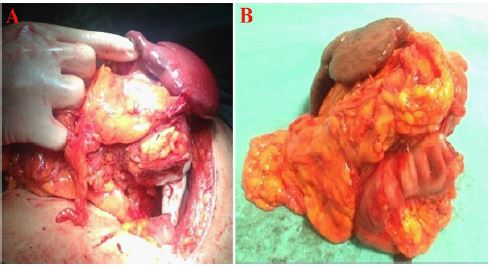
As malignancy could not be ruled out, surgery of the pancreatic mass was planned. During exploration, the pancreatic mass could not be dissected from the splenic hilum and the splenic flexure of the colon. The lesion was completely resected with distal pancreatectomy, splenectomy, and segmental colectomy (Figure 2). Transurethral resection was performed for the bladder lesions. There were no postoperative complications and the patient was discharged on the fourth day.
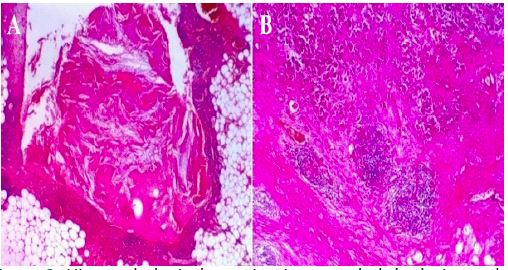
Histopathological examination revealed a cystic lesion lined by squamous epithelium with the presence of lymphoid tissue that formed lymphoid follicles in the subepithelial zone. There was sebaceous differentiation on the cyst wall. The findings consisted of pancreatic lymphoepithelial cyst (Figure 3). Histopathological examination of the bladder mass was reported as low grade papillary uroepithelial carcinoma.
Discussion
The prevalence of PCLs has been increasing due to the development and frequent use of imaging devices such as CT, Endoscopic Ultrasound (EUS). In clinical practice, proper preoperative diagnosis of these lesions is an important issue both to determine the prognosis of the disease and to avoid unnecessary surgical interventions, because the treatment and prognosis of each lesion are very different. Despite the increasing use of high-quality imaging studies and EUS guide biopsy; these lesions may not be properly diagnosed. Surgical resection can be considered for symptomatic PLECs or if the diagnosis remains uncertain and the suspicion of malignancy is high. PLECs are rare and benign lesions comprising approximately 0.5% of all PCLs. They occur predominantly in men in the 5th and 6th decades of life. They range in size from 1.2 to 17 cm (mean size 4.6 cm) and can arise in any part of the pancreas [2]. The most common locations are tail (43.5%), body (33.2%), and head (23.4%) of the pancreas, respectively [8]. Most of these PLECs are asymptomatic until they reach large sizes. Abdominal pain and discomfort are the most common symptoms [2,8]. Although imaging and Fine Needle Aspiration Biopsy (FNAB) are useful tools for differential diagnosis, complete excision of the lesion may be necessary for accurate diagnosis [9].
The exact etiology of the PLECs is unknown. But various theories such as epithelial remnants in lymph nodes, a cystic transformation of pancreatic ducts with squamous metaplasia, displaced branchial cleft cysts that were fused with the pancreas during embryogenesis, or a form of teratoma have been proposed [2,10]. PLECs do not appear to be associated with autoimmune disorders, HIV infection, or lymphoma [1,5].
Macroscopically, they appear as uniformly bounded cysts with caseous or cheesy contents. In the microscopic examination, the cyst wall is lined by squamous epithelium, and a dense lymphoid tissue in the subepithelial zone that forms lymphoid follicles is typical. The lymphoid cells on the wall of the cyst are mostly mature T lymphocytes and B lymphocytes which form germinal centers. Sebaceous differentiation of the cyst is rare but mucinous cells can be seen. If sebaceous and mucinous components are dominant, then the accurate diagnosis is dermoid cyst [2]. In our case, the cyst wall was lined by squamous epithelium with lymphoid follicles and there were a few scattered sebaceous differentiation foci in the center. We think that this sebaceous differentiation focuses reported as a macroscopic fatty component on CECT.
Pancreatic lymphoepithelial cysts are benign lesions and no recurrence or malign transformation has been reported up to now [4]. EUS is important in terms of determining the lesion characteristics as well as evaluating the cyst content and allowing histological examination [5,7,8]. Some reports supporting that Contrast Enhanced Endoscopic Ultrasound (CEEUS) and Fine Needle Aspiration Biopsy (FNAB) may be useful for preoperative differential diagnosis [7,11]. In a review recently reported by Osiro and colleagues, it was mentioned that preoperative diagnosis of PLECs could be provided with 3D-CT scans, in-phase and out-of-phase magnetic resonance scans, and FNAB studies with the guidance of CEEUS [12]. EUS can also be used in the treatment of symptomatic or complicated PLECs [13]. In a small series including 6 patients published by Martin et al., surgical treatment was applied to all patients because mucinous cystic neoplasm could not be ruled out although CT, MRI, and EUS-FNAB were used all together [14]. Groot et al., in a study of 29 patients, demonstrated that only 7 (34%) patients could be diagnosed preoperatively and 22 (76%) patients were diagnosed after surgery, although EUS was performed in 19 (66%) patients and EUS-FNA was performed in 16 patients [8]. Even if CT, MRI, EUS-FNA, and cystic fluid analysis are performed, the differentiation of mucinous cysts with PLECs is often difficult [8,14]. Nevertheless, the presence of basic features such as exophytic growth pattern, absence of pancreatic duct dilatation and histological features specific to PLECs are findings in favor of PLECs [8]. Pancreatic lymphoepithelial cysts differ from mucinous neoplasms as they have low levels of CA 19-9, CEA, and low viscosity. Histopathologic examination of mucinous neoplasms does not include subepithelial lymphoid tissue. Lymphoepithelial cysts do not show papillary changes and the mucinous cells are rare [15]. The diagnosis with fluid-based aspiration is doubtful because there are only limited cases in the literature.
In the literature, bladder metastasis from pancreatic cancer has been reported very rarely [16,17]. In our patient, we thought that the pancreatic lesion was pancreatic carcinoma with bladder metastasis due to fact that the mass was seen both in the pancreas and bladder and the cystic component of the lesion was very small. If we considered this lesion as PLEC and diagnosed the case as PLEC preoperatively, surgical intervention would be unnecessary. We strongly believe that in asymptomatic cases who are diagnosed as PLECs preoperatively, close follow-up is the best choice instead of major surgical intervention. Although there is increased interest in preoperative diagnosis of PLECs, most cases are diagnosed after surgery [8,14].
Conclusion
In conclusion, PLECs are very rare lesions in the pancreas, PLECs with accompanying uroepithelial carcinoma is extremely rare in the literature. Complete excision and pathological examination are still a valid approach in symptomatic cases or case of suspected malignancy. We report this case because of the coexistence of PLECs and uroepithelial carcinoma is an unusual finding.
Declarations
Acknowledgments: I thank Dr. Şehmus Ölmez for reviewing the manuscript.
Declaration of interest statement: All authors declared that no potential conflict of interest relevant to this article was reported.
References
- Abdelkader A, Hunt B, Hartley CP, et al. Cystic Lesions of the Pancreas: Differential Diagnosis and Cytologic-Histologic Correlation. Arch Pathol Lab Med. 2020; 144: 47-61.
- Adsay NV, Hasteh F, Cheng JD, et al. Lymphoepithelial cysts of the pancreas: A report of 12 cases and a review of the literature. Mod Pathol. 2002; 15: 492-501.
- Farrell JJ. Prevalence, Diagnosis and Management of Pancreatic Cystic Neoplasms: Current Status and Future Directions. Gut Liver. 2015; 9: 571-589.
- Sewkani A, Purohit D, Singh V, et al. Lymphoepithelial cyst of the pancreas: A rare case report and review of literature. Indian J Surg. 2010; 72: 427-432.
- Borhani AA, Fasanella KE, Iranpour N, et al. Lymphoepithelial cyst of pancreas: Spectrum of radiological findings with pathologic correlation. Abdom Radiol (NY). 2017; 42: 877-883.
- Namba Y, Oshita A, Nishisaka T, et al. Lymphoepithelial cyst of the pancreas: A case report and summary of imaging features of pancreatic cysts. Int J Surg Case Rep. 2019; 55: 192-195.
- Nasr J, Sanders M, Fasanella, et al. Lymphoepithelial cysts of the pancreas: An EUS case series. GastrointestEndosc. 2008; 68: 170-173.
- Groot VP, Thakker SS, Gemenetzis G, et al. Lessons learned from 29 lymphoepithelial cysts of the pancreas: institutional experience and review of the literature. HPB (Oxford). 2018; 20: 612-620.
- Yanagimoto H, Satoi S, Toyokawa H, et al. Laparoscopic distal pancreatectomy for a pancreatic lymphoepithelial cyst: Case report and review of literature. JOP. 2013; 14: 664-668.
- Basturk O, Coban I, Adsay NV. Pancreatic cysts: Pathologic classification, differential diagnosis, and clinical implications. Arch Pathol Lab Med. 2009; 133: 423-438.
- Matsumoto K, Kato H, Tomoda T, et al. Nihon Shokakibyo Gakkai Zasshi. 2013; 110: 1823-1830.
- Osiro S, Rodriguez JR, Tiwari KJ, et al. Is preoperative diagnosis possible? A clinical and radiological review of lymphoepithelial cysts of the pancreas. JOP. 2013; 14: 15-20.
- Chowdhry M, Bilal M, Shah H, et al. Large lymphoepithelial cyst of pancreas: a rare entity managed using lumen-apposing metal stent-case report and review of the literature. Clin J Gastroenterol. 2019; 12: 609-614.
- Martin J, Roberts KJ, Sheridan M, et al. Lymphoepithelial cysts of the pancreas: A management dilemma. Hepatobiliary Pancreat Dis Int. 2014; 13: 539-544.
- Zhu LC, Grieco V. Diagnostic value of unusual gross appearance of aspirated material from endoscopic ultrasound-guided fine needle aspiration of pancreatic and peripancreatic cystic lesions. Acta Cytol. 2008; 52: 535-540.
- Chiang KS, Lamki N, Athey PA. Metastasis to the bladder from pancreatic adenocarcinoma presenting with hematuria. Urol Radiol. 1992; 13: 187-189.
- Shah A, Korrapati P, Siegel J, et al. Rare Metastasis of Primary Pancreatic Adenocarcinoma to the Bladder. ACG Case Rep J. 2018; 5: e27.