
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
The curtain tieback: Typical aspect of tumoral and infectious epiduritis
Abir Lemrabet*; Meryem Benmoussa; Hajar Zebbakh; Ittimade Nassar; Nabil Moatassim Billah
Central Radiology Department, IBN SINA Hospital, Mohamed V University, Rabat, Morocco.
*Corresponding Author : Abir Lemrabet
Central Radiology Department, IBN SINA Hospital, Mohamed V University, Rabat, Morocco.
Email: abirlemrabet8@gmail.com
Received : Oct 27, 2022
Accepted : Nov 11, 2022
Published : Nov 18, 2022
Archived : www.jcimcr.org
Copyright : © Lemrabet A ( (2022).
Citation: Lemrabet A, Benmoussa M, Zebbakh H, Nassar I, Billah NM, et al. The curtain tieback: Typical aspect of tumoral and infectious epiduritis. J Clin Images Med Case Rep. 2022; 3(11): 2162.
Introduction
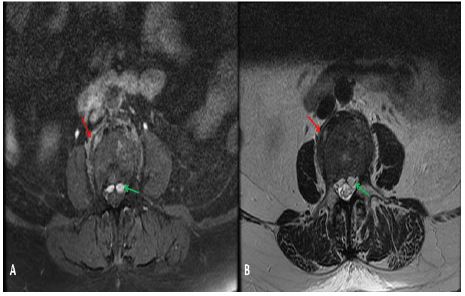
A 71-year-old woman with multiple myeloma complaining of sudden onset low back pain, associated with functional impotence of both lower limbs. The clinical examination found paraparesis of the lower limbs. An MRI was performed 72 hours after onset of symptoms.
Discussion
Epiduritis corresponds to extensive or localized inflammation in the epidural space, it can be of infectious, tumoral, inflammatory or traumatic origin, etc. All locations are possible, but it preferentially reaches the lower lumbar and thoracic level. The posterior epidural compartment is much more affected than the anterior in 80% of cases [1].
Curtain flare is a particular semiological sign on MRI in anterior epiduritis of infectious or tumoral origin. When the tumoral or infectious lesion of vertebral origin extends towards the anterior epidural compartment, the lesion presents a characteristic bilobed shape, “curtain flare”. The anterior epidural compartment is subdivided into two right and left sub-compartments by the longitudinal ligament, thus constituting an anatomical barrier to the right-left migration of any pathological process and inducing a bilobed image of the lesion “in ablaze of the curtain” [2].
MRI is the examination of choice for studying the perimedullary spaces [3]. The exploration systematically includes 2 cutting planes (sagittal and axial) and 2 weightings (T1 and T2) in order to locate the pathological process between the different perimedullary compartments, the examination can be supplemented by an injection of gadolinium in the event of discovery. Of a tumoral or infectious lesion. Possible sagittal and axial T1 sections with fat saturation after injection of gadolinium for the study of extradural pathology and without fat saturation for intradural pathology. Coronal T1 sections with fat saturation after injection of gadolinium would be proposed in the event of foraminal and/or perivertebral extension. Sagittal T2 and/or T1 images with or without fat saturation after injection of gadolinium are also proposed on the adjacent level [3].
Final diagnosis: Sign of the curtain tie in epiduritis.
References
- Epidurite staphylococcique. Oncle Paul. 2011.
- Manelfe C, Demondion X, Cognard C, Sans N, Francke J, et al. L’espace épidural à l’étage lombaire. Étude radio-anatomique. 2020; 11.
- Holl N, Kremer S, Wolfram Gabel R, Dietemann JL. Espaces rachidiens intracanalaires: de l’anatomie radiologique au diagnostic étiologique. Journal de Radiologie. 2010; 91: 950–968.