
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Bilateral complete duplication of ureters with upper moiety PUJO and ectopic insertion: A rare case report
Naman Aggarwal*; Shruti Pandit; Arun Chawla
Department of Urology and Renal Transplant, Kasturba Hospital, MAHE, Manipal, Karnataka, India.
*Corresponding Author : Naman Aggarwal
Department of Urology and Renal Transplant, Kasturba Hospital, MAHE, Manipal, Karnataka, India.
Email: drnamanaggarwal@gmail.com
Received : Oct 31, 2022
Accepted : Nov 11, 2022
Published : Nov 18, 2022
Archived : www.jcimcr.org
Copyright : © Aggarwal N (2022).
Abstract
Duplication of the ureter and renal pelvis is one of the most common anomalies of the upper tracts with incidence reported to be approximately 2% [1]. An increased incidence of uretero-renal pathology has been documented with duplication anomalies. Here we present a case report of a 27-year-old married male who presented with a bilateral complete duplex system with ectopic insertion into the prostatic urethra. On evaluation he was found to have a non-functioning left upper moiety and a right upper moiety ureteropelvic junction obstruction. In this case report we discuss the complications and therapeutic implications of a duplicated system.
Keywords: Bilateral; Duplex collecting system; Complete duplication.
Citation: Aggarwal N, Pandit S, Chawla A, et al. Bilateral complete duplication of ureters with upper moiety PUJO and ectopic insertion: A rare case report. J Clin Images Med Case Rep. 2022; 3(11): 2163.
Introduction
Nearly 10% of all human beings are born with some form of congenital anomaly of the urogenital system [2], the most common anomaly being duplication of ureter which is seen in approximately 1 in 160 individuals [3]. Duplication occurs when two separate ureteric buds arise from a single wolffian duct [4].The upper pole is more likely to be affected by conditions of abnormal ureteral formation, like ureterocele and ectopic ureter. Whereas, the lower moiety is more likely to be affected by ureteropelvic junction obstruction and vesicoureteric reflex. Upper pole ureteropelvic junction obstruction has been reported but is exceptionally rare [6]. In this case report we describe a bilateral complete duplication with a right upper moiety UPJO and non-functioning left upper moiety.
Case report
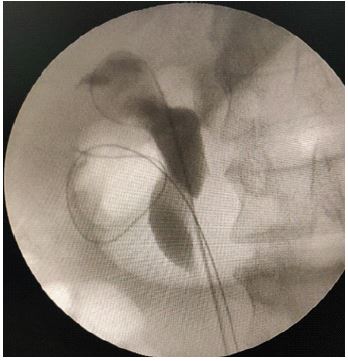
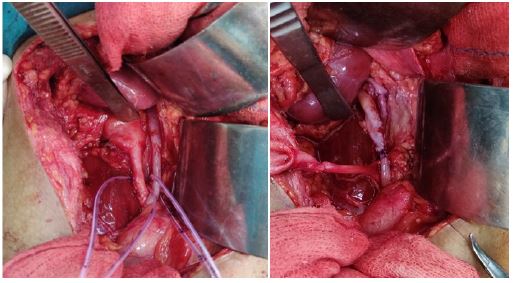
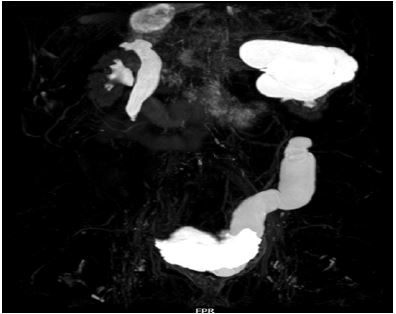
27 year old married male patient presented to Urology OPD of Kasturba Medical Hospital with complaints of right flank pain. He was a known case of bilateral complete duplication of ureters with history of left upper pole nephrectomy three years ago for non-functioning left upper moiety. A contrast enhanced computed tomography (Figure 1) showed a dilated right upper moiety pelvicalyceal system with a narrow ureteropelvic junction and adequate opacification on delayed imaging. He was diagnosed to have a right upper moiety ureteropelvic junction obstruction. A cystourethroscopy was done where the ectopic location of the right ureter was identified in the prostatic urethra (Figure 2), confirmed to drain the dilated upper moiety on retrogradepyelogram (Figure 3). He underwent a right end to side pyelo-pyelostomy (Figure 4) of the duplicated system to relieve the obstruction. He has been on regular follow up since then and is currently asymptomatic. His renal parameters being normal throughout the course of disease. Four months after surgery he underwent a MR Urogram, showing compact pelvicalyceal system of both moieties (Figure 5). A retrograde pyelogram was done showing the blind ending upper moiety ureter, with a patent anastomosis of the upper and lower moiety pelvis (Figure 6, Figure 7).




Discussion
Duplex collecting system can be defined as an incomplete fusion of upper and lower pole moieties. Depending upon the degree of fusion it can be divided into four types. First being the bifid renal pelvis, second the partial ureteric duplication or Y shaped ureter, third the incomplete ureteric duplication where the ureters join near or in the bladder wall and the last type being a complete ureteral duplication where the ureters have separate orifices [5]. The clinical implications of duplicated system depend largely on the site of ureteral insertion. During the entire lifetime a bifid ureter may remain asymptomatic, however in a completely duplicated system complications may arise.
In this case we present a bilateral duplex collecting system with complete duplication of ureter. The right upper moiety ureter having an ectopic insertion into the prostatic urethra and being obstructed due to ureteropelvic junction obstruction. Although duplication of ureter is the most common anomaly of the urogenital system as mentioned above, bilateral complete duplication is relatively rare, unilateral is six times more common than bilateral duplication [7]. In accordance with the Weigert-Meyer law the upper pole ureter typically opens medially and caudally while the lower pole ureter opens laterally and cranially. The upper moiety is more likely to be affected due to abnormal ureteral formation, including ectopic ureter and ureterocele. The lower moiety is more likely to be affected by ureteropelvic junction obstruction and vesicoureteric reflux. In this case the left upper moiety was in accordance with the Weigert-Meyer rule, ectopic orifice causing a chronic obstruction leading to non-functioning of that moiety. However, the right upper moiety being affected by ureteropelvic junction obstruction is relatively rare [6].This association of a bilateral duplex system, with an ectopic orifice and a UPJO is not clearly described in literature to the best of our knowledge.
This patient had been asymptomatic since birth and presented at 24 years of age by which time the left upper moiety was non-functioning due to obstruction considering its ectopic orifice in the prostatic urethra. The main goal at this stage was not only to improve the patient’s symptoms but also to protect the functioning lower moiety. During this patient first visit although the bilateral duplicated system was diagnosed, both upper and lower moiety was well functioning on a contrast CT and both the pelvicalyceal systems were compact with no evidence of any obstruction. The most common complication of a complete duplication is a vesicoureteric reflux which is seen commonly on the lower pole [5]. This patient did not have evidence of a refluxing system and his symptoms of the left side were due to ectopic ureter. Duplication may also be compatible with a normally functioning renal system if both the ureters have an orthotopic orifice which is seen in case of incomplete duplication.
In a duplicated system the complication of ureteropelvic junction obstruction is commonly seen in the lower moiety, involvement of the upper moiety is relatively rare [6], which was seen in this case. At the first presentation the right upper moimoiety was normal which became progressively dilated as the UPJO set in. Since this patient was on routine follow-up this was diagnosed early with the function of the right upper moiety being well preserved. Hence a heminephrectomy was not necessary and the obstruction was relieved with an end to side pyelo-pylelostomy.
Conclusion
A bilateral duplex collecting system is a rare anatomic abnormality. Furthermore, the fact that the upper moiety ureter has an ectopic orifice into the prostatic urethra with an obstruction secondary to UPJO makes this case an exceptional case. The clinical manifestations of a duplicated ureter are varied and knowledge of the anatomical variations of the ureter are necessary for early diagnosis and treatment to prevent renal impairment in a young patient.
References
- Privett JT, Jeans WD, Roylance J. The incidence and importance of renal duplicaition. Clin Radiol. 1976; 27: 521-530.
- Burkland CE. The significance of genetic and environmental factors in urogenital disease. Journal of Urology. 1958; 79: 532.
- Nation EF. Duplication of the kidney and ureter. Astatistical study of 230 new cases. Journal of Urology. 1944; 51: 456.
- Inamoto K, Tanaka S, Takemura K, Ikoma F. Duplication of renal pelvis and ureter: Associated anomlies and pathological conditions. Radiat Med. 1983; 1: 55-64.
- Fernbach SK, Feinstein KA, Spencer K, Lindstorm CA. Ureteral duplication and its complications. Radiographics. 1997; 17: 109-127.
- Ho DS, Jerkins GR, Williams M, Noe HN. Ureteropelvic junction obstruction in upper and lower moiety of duplex systems. Urology. 1995; 45: 503-506.
- Whitaker J, Danks DM. A study of the inheritance of duplication of the kidneys and ureters. J Urol. 1966; 95: 176-178.