
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Isolated Salter-Harris type IV distal ulna fracture: A case report
Michael Czulinski, DO*; Eric Taris, DO; Kent Lord, MD; Brandon Green, DO; B Roy Smith Jr, MD
Orthopedic Surgery Department, East Tennessee State University, USA.
*Corresponding Author : Michael Czulinski
Orthopedic Surgery Department, East Tennessee State University, USA.
Email: czulinski@etsu.edu
Received : Oct 20, 2022
Accepted : Nov 15, 2022
Published : Nov 22, 2022
Archived : www.jcimcr.org
Copyright : © Czulinski M (2022).
Abstract
Isolated physeal fractures in the pediatric distal ulna are relatively uncommon. While the skeletally immature patient generally has higher remodeling potential than adults, special considerations should be given to the pediatric wrist. We report the case of a 15-year-old male with an isolated Salter-Harris (SH) type IV distal ulna fracture.
Keywords: Physeal injury; Ulna; Salter-Harris IV.
Citation: Czulinski M, Taris E, Lord K, Green B, Smith Jr R. Isolated Salter-Harris Type IV Distal Ulna Fracture: A Case Report. J Clin Images Med Case Rep. 2022; 3(11): 2166.
Introduction
Fractures in the pediatric population have been estimated to involve the growth plate 15-18% of the time [1]. While forearm fractures are among the most common pediatric fractures, isolated distal ulna physeal fractures are relatively rare. Approximately 81% of longitudinal ulnar growth has been estimated to occur at the distal ulnar physis [2]. It is for this reason that fractures involving the ulnar physis are of particular concern. Fractures of the distal ulna may lead to growth arrest, deformity of the forearm and altered wrist kinematics. To our knowledge, we present the only reported isolated SH IV distal ulnar fracture managed nonoperatively without attempted reduction.
Case presentation
A right-hand dominant 15-year-old male presented after a fall onto an outstretched right hand while playing baseball. He reported immediate ulnar-sided wrist pain worse with use, specifically “twisting” which caused sharp pain on the ulnar aspect of the wrist. On physical examination the extremity was closed and neurovascularly intact. He had mild swelling about the wrist and significant tenderness to palpation over the dorsal ulna and fovea. Posteroanterior and lateral radiographs of the wrist demonstrated a displaced SH type IV fracture of the distal ulna without associated radius fracture (Figure 1a). The patient was made non weight-bearing (NWB) and placed in a sugar tong splint. An MRI was ordered to evaluate the distal radioulnar joint (DRUJ) and triangular fibrocartilage complex (TFCC). The MRI was obtained and reviewed five days after the injury. Findings included SH IV fracture of the ulna with subtle edema in the mid-radial scaphoid without associated fracture. The TFCC, scapholunate, lunotriquetral ligaments remained intact.
Surgical and nonsurgical options were discussed with the family. Conservative management without attempted closed reduction was selected. The patient was kept NWB in a sugar tong splint for two weeks. On examination at two weeks, the splint was removed, but the patient remained tender at the distal ulna. The patient had 40 degrees of both pronation and supination at the wrist with radiographs showing no interval displacement (Figure 1b). He was placed into a sugar tong splint for an additional two weeks.

The four-week follow-up radiographs demonstrated significant healing with evidence of early central physeal bar formation (Figure 1c). The patient had minimal tenderness to palpation about the fracture. He had full pronation, but only 40 degrees of supination with palpable crepitus at the DRUJ. At this time, he was advanced to gentle active range of motion with maintained NWB and a removable wrist splint. The three-month follow-up radiographs demonstrated distal ulna fracture remodeling and central physeal bar formation. Clinically, the patient is nontender about the DRUJ with full pronosupination and a reported complete return to activity as tolerated without pain. The patient will continue to be followed until skeletal maturity is reached.
Discussion
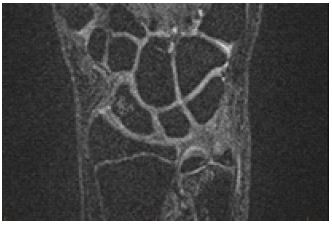
The infrequent occurrence of isolated ulnar physeal injury may be due to the anatomy and biomechanics of the wrist. The ulna is estimated to bear approximately 1/3rd of the axial load across the wrist [11]. Additionally, the ulnar styloid has strong ligamentous attachments that may lead to avulsion injuries of the ulnar styloid more frequently than intraphyseal injuries [4]. In the reviewed literature and associated case reports, falling onto an outstretched hand is the most commonly reported injury mechanism. More specifically, compression across a pronated forearm in an ulnarly deviated and dorsiflexed wrist has been described [5]. While our patient did not recall the exact wrist position, the mid-radial scaphoid edema noted on the MRI may suggest an axial loading injury on a slightly ulnarly deviated wrist at the time of injury (Figure 2).
Isolated distal ulnar fractures involving the growth plate are uncommon and are associated with a significant risk of physeal arrest. There are limited reports available on the evaluation of isolated ulnar physeal injury. However, in a case series by Golz et al., 18 patients with ulnar physeal injuries in association with radius fractures were evaluated. They noted that the most common distal ulnar fracture pattern in the case series was SH Type 1 (n-8) followed by SH Type 3 (n-6) and included only a single SH Type 2 and SH Type 4 [3]. Two patients had unspecified physeal injury patterns [3]. Golz et al. noted that at an average of 3 ½ years follow-up there was physeal arrest present in 55% of the patients with the majority being asymptomatic and the most common complaint being cosmesis [3]. In our review of the literature, we identified two additional reported cases of isolated SH Type 4 fractures and one with an associated distal radius fracture. None of the reported cases were managed nonoperatively and all sustained physeal arrest.
Growth disturbances can lead to subsequent radial or ulnar angulation, distal radial ulnar joint pain, instability, ulnar translation of the carpus or ulnar negative variance. It is for this reason that operative management should be considered in younger skeletally immature patients. When considering surgical treatment, it is important to evaluate the amount of growth remaining, damage to surrounding structures and the family goals on a case-by-case basis. The three identified case reports of displaced SH type IV distal ulnar fractures were treated with attempt and failure of closed reduction or open reduction with pinning in an anatomic reduction [6-8]. Open reduction was required in all three cases. In one case, a volar-ulnar approach was used, and in another case, a longitudinal dorsal wrist incision was utilized. The third case did not specify the approach used [6,8]. In all three mentioned cases physeal arrest occurred despite surgical intervention [6-8].
In the largest reported series examining ulnar physeal injuries, only 4 of the 18 included patients were treated operatively and the majority of patients were asymptomatic at 3 ½ years [3]. The high likelihood of physeal closure despite attempted open reduction should be considered in management of fractures, especially in those approaching skeletal maturity. Additionally, the risk of iatrogenic injury to surrounding structures such as the TFCC or DRUJ, as well as further injury to the physis during surgical approach should be considered when choosing operative versus nonoperative management. Due to the patient approaching skeletal maturity, in addition to MRI demonstrating a reduced DRUJ, an intact TFCC, and no evidence of extensor carpi ulnaris entrapment, surgical intervention was felt to offer minimal benefit. In those patients approaching skeletal maturity, major deformity is unlikely given minimal remaining growth, but discussion should address the increased risk for later DRUJ arthritis and negative ulnar variance.
Conclusion
We reported a conservative approach to an isolated Salter-Harris type IV distal ulnar physeal injury in a patient approaching skeletal maturity who opted for conservative, nonoperative management without attempted closed reduction. Isolated ulnar physeal injuries remain an uncommon injury with limited reports in the literature. As such, patients should be managed on a case-by-case basis taking special consideration for remaining growth potential and possible subsequent deformity. Surgical intervention should be considered in those patients who have displaced fractures with the possibility of remaining growth potential. The goals of surgery should include anatomic reduction with minimal additional iatrogenic physeal injury. In those select patients approaching skeletal maturity conservative management is reasonable, but should be monitored closely. Treatment should include surveillance into skeletal maturity in all patients, regardless of treatment selected. In the event of growth disturbance, surgical intervention following skeletal maturity should be considered in those who have clinically significant symptoms.
References
- Meyers AL, Marquart MJ. Pediatric Physeal Injuries Overview. [Updated 2021 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560546/
- Noonan KJ, Price CT. Forearm and distal radius fractures in children. J AM Acad Orthop Surge 1998;6:146-56.
- R. J. Golz, D. P. Grogan, T. L. Greene, R. J. Belsole, and J. A. Ogden, “Distal ulnar physeal injury,” Journal of Pediatric Orthopedics, Vol. 11, no. 3, pp. 318-326, 1991.
- Ogden JA, et al. Radiology of Postnatal skeletal development. IV. Distal radius and ulna. Skeletal Radiol 1981;6:255-66.
- Mitrousias, Vasileios et al. “Isolated Salter-Harris Type II Fracture of the Distal Ulna.” Curēus (Palo Alto, CA) 13.6 (2021).
- Faraj, Adnan A et al. “An Irreducible Salter–Harris Type IV Distal Ulna Fracture.” Injury 31.9 (2000): 746–748.
- Kasis, Ata G, Waleed E. A Hekal, and Ahmed Mubashir. “Isolated Salter-Harris Type IV Fracture of the Distal Ulna in a 12-Year-Old Boy.” European journal of trauma 30.2 (2004): 127–129.
- Marrannes, Stephanie, Delphine Lambrecht, and Arne Decramer. “Reduction of an Unusual Salter-Harris Type IV Fracture of the Ulna.” Case reports in orthopedics 2020 (2020): 8498401–5.
- Tiwari, Vivek, Samir Dwidmuthe, and Samrat S Sahoo. “A Rare Case of Isolated Type III Salter-Harris Physeal Injury of the Distal Ulna.” Curēus (Palo Alto, CA) 13.4 (2021).
- Clesham, Kevin, Robert P Piggott, and Eoin Sheehan. “Displaced Salter-Harris I Fracture of the Distal Ulna Physis.” BMJ case reports 12.8 (2019).
- H. Shaaban; G. Giakas; M. Bolton; R. Williams; P. Wicks; L.R. Scheker; V.C. Lees. “The load-bearing characteristics of the forearm: pattern of axial and bending force transmitted through ulna and radius.” 31(3), 0–279.