
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cardiac tamponade in a male as an initial presentation of SLE.
An interesting case report
Ziad Affas, MD*; Diana Singh, MD; Sumeet Aujla, MD; Vijay Patel, MD
Department of Internal Medicine, Henry Ford Macomb Hospital, Michigan, USA
*Corresponding Author : Ziad Affas, MD
Department of Internal Medicine, Henry Ford Macomb Hospital, Michigan, USA.
Email: zaffas2@hfhs.org
Received : Nov 01, 2022
Accepted : Nov 17, 2022
Published : Nov 24, 2022
Archived : www.jcimcr.org
Copyright : © Affas Z (2022).
Abstract
A relapsing and remitting illness that may affect any organ system, systemic lupus erythematosus (SLE) is a chronic autoimmune inflammatory condition. Autoantibodies and immune complex development are its defining features. The heart is one of the organs that it might impact. In patients with SLE, the immune system’s response to dying cells is aberrant. The diagnosis of SLE is made on the basis of distinctive clinical findings in the skin, joints, kidneys, and central nervous system, as well as serological indicators like antinuclear antibodies (ANA), specifically antibodies to dsDNA. Nonsteroidal anti-inflammatory medicines (NSAIDs), corticosteroids, immunosuppressive medications, and biological agents may be used to treat lupus, depending on the symptoms, findings of blood tests, and the specific organs affected. Here we are reporting a rare case of a male with pericardial tamponade as a first symptom of SLE.
Case presentation: A 33-year-old male with a past medical history significant for Asthma and Raynaud’s phenomenon presented to the emergency department after his outpatient hematologist noticed he was tachycardic with bilateral lower extremity edema. Patient was referred to hematology by his primary care physician when he reported 3 months of fatigue and his labs revealed elevated gamma globulins and anemia and a cough with clear sputum for several weeks. On physical examination, the patient was hypotensive to 116/18 and tachycardic to 138 bpm, his respiratory rate was 16 breaths per minute and he was afebrile. He was notably short of breath and tachycardic. S1 and S2 were heard but distant, with no additional heart sounds, murmurs, rubs, or gallops, JVD was mildly raised. He had decreased breath sounds in the right lower lobe but no wheezes, rales, or rhonchi. Bilateral lower extremities were remarkable for 1+ pitting edema. His Urine albumin to creatinine ratio was elevated (82.7 mg/g) with a normal creatinine and GFR. A kidney biopsy was scheduled for further investigation of his moderate proteinuria. Electrocardiogram revealed sinus tachycardia with a rate of 134 beats per minute with low voltage QRS but no evidence of electrical alternans. Echo showed moderately sized pericardial effusion. Cardiothoracic surgery (CTS) created a subxiphoid pericardial window and inserted a right thoracostomy tube for drainage of fluid. Patient reported improvement in his shortness of breath and pleuritic chest pain.
Discussion: SLE commonly affects the heart. Heart-related issues will affect around half of SLE patients. The most common cardiac problems in SLE patients are pericarditis, myocarditis, valve issues, thrombosis, and anomalies of the conduction system. Only 9 of the 41 SLE patients who presented with pericardial effusion in retrospective research that examined cases from 1985 to 2006 had cardiac tamponade. Each of them was a female. Despite receiving high dosage corticosteroid therapy, five of them needed a pericardial window. Low blood C4 levels, being a woman, having concomitant renal illness, hemolytic anemia, and pleurisy were revealed to be the most probable predictors of tamponade in SLE patients who present with pericarditis and pericardial effusions. Systemic sclerosis and SLE have the greatest rates of pericardial involvement (60%) among the other connective tissue disorders. In individuals with various connective tissue disorders, pericarditis is an uncommon hemodynamic consequence that may be effectively treated with NSAIDS and corticosteroids. Although pericardial illness is seen often in autopsies and echocardiograms, there may be another explanation for the low prevalence of tamponade. Pericardiocentesis is only performed in cases of tamponade that poses a serious risk to life and persistent massive pericardial effusion. Those who don’t react need a pericardial window. When pericardiocentesis is not practicable, intravenous immunoglobulins are another therapy option. Cardiac tamponade in systemic lupus erythematosus should be treated with high dosage steroids and pericardiocentesis.
Citation: Affas Z, Singh D, Auila S, Patel V. Cardiac tamponade in a male as an initial presentation of SLE. An interesting case report. J Clin Images Med Case Rep. 2022; 3(11): 2171.
Introduction
A relapsing and remitting illness that may affect any organ system, systemic lupus erythematosus (SLE) is a chronic autoimmune inflammatory condition. Autoantibodies and immune complex development are its defining features [1]. The heart is one of the organs that it might impact. In patients with SLE, the immune system’s response to dying cells is aberrant. The systems that keep self-tolerance in place have fundamentally failed. Because dying cells’ nuclear material is not effectively eliminated, an immunological reaction is triggered, which increases the production of autoantibodies against nuclear antigens and autoreactive T and B cells. The final outcome is a cycle of immune cell activation and antigen release those results in the creation of high-affinity autoantibodies. About 90% of SLE patients are female, and when female sex hormones began to emerge, the risk of the illness substantially increased [2].
The illness comes in a variety of morphologies, with clinical symptoms ranging from modest mucocutaneous signs to severe central nervous system involvement involving many organs. Pericarditis, myocarditis, and endocarditis are three different cardiac manifestations of SLE. The most frequent cardiac issue associated with SLE is pericarditis [3]. However, cardiac tamponade as the disease’s primary symptom is uncommon. A potentially fatal side effect of SLE is cardiac tamponade, which happens when a significant quantity of fluid collects in the pericardium and reduces blood flow to the ventricles [4]. Hypotension, pulsus paradoxus, dyspnea, orthopnea, and chest discomfort are typical symptoms and indicators (Figure 1).
SLE may be difficult to diagnose, and there is no one clinical symptom or laboratory abnormalities that can definitively rule out the disease [5]. SLE is instead identified based on a combination of symptoms, signs, and relevant laboratory tests. Histopathology and imaging might both be quite important. With varied sensitivity and specificity, a number of autoantibodies have been identified in SLE. Others may operate as a sign of disease activity, while certain autoantibodies may be linked to a particular clinical subtype of SLE.
The first test should check for antinuclear antibodies (ANA), which are the disease’s defining feature. The gold standard ANA test is known as the immunofluorescence assay. Although multiplex tests and other detection techniques like the enzyme-linked immunosorbent assay (ELISA) are frequently used, they lack sensitivity [6].
The diagnosis of SLE is made on the basis of distinctive clinical findings in the skin, joints, kidneys, and central nervous system, as well as serological indicators like antinuclear antibodies (ANA), specifically antibodies to dsDNA, which rule out other conditions that may present with comparable symptoms (such as Lyme disease) [7]. Nonsteroidal anti-inflammatory medicines (NSAIDs), corticosteroids, immunosuppressive medications, and biological agents may be used to treat lupus, depending on the symptoms, findings of blood tests, and the specific organs affected. With the right care, most lupus sufferers may anticipate a normal lifetime, but many may endure some degree of impairment [8]. More serious health issues associated with lupus, such neurological issues and kidney damage, need for aggressive therapy. Here we are reporting a rare case of a male with pericardial tamponade as a first symptom of SLE.
Case presentation
A 33-year-old male with a past medical history significant for Asthma and Raynaud’s phenomenon presented to the emergency department after his outpatient hematologist noticed he was tachycardic with bilateral lower extremity edema. Patient was referred to hematology by his primary care physician when he reported 3 months of fatigue and his labs revealed elevated gamma globulins and anemia. He reported 60 lb of intentional weight loss over the last 8 months secondary to diet and exercise. The patient denied any recent trauma, viral or bacterial illnesses, history of other rheumatological conditions, family or personal history of connective tissue disorders, and cancer
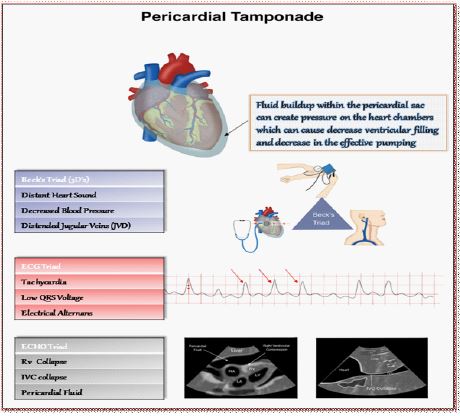
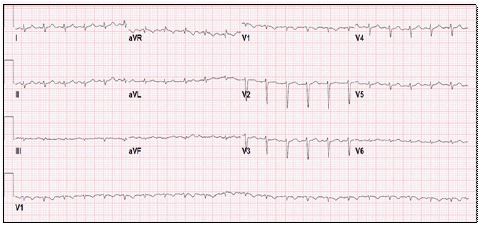
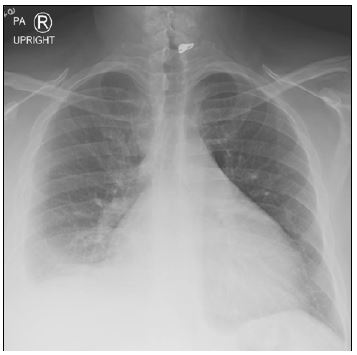
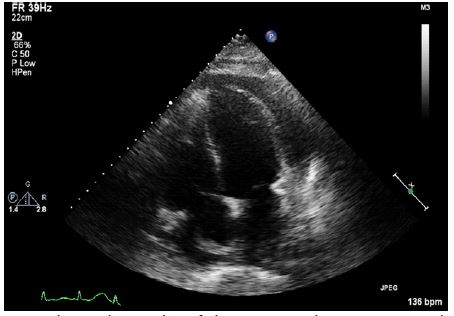
Table 1: Initial laboratory investigations
| Test | Laboratory results | Normal range |
|---|---|---|
| Albumin | 1.9 g/dL | 3.7 - 4.8 g/dL |
| Hemoglobin | 11 g/dL | 13.5 - 17.0 g/dL |
| Iron Saturation | 8% | 15 - 50 % |
| Serum Ferritin | 751 ng/mL | 24 - 336 ng/mL |
| High Sensitivity Troponin | 26 ng/L | < 4 ng/L |
| D-Dimer | 8.58 ug/ml | < 0.74 ug/mL |
| BNP | 131 pg/ml | < 50 pg/mL |
Table 2: Rheumatologic workup
| Test | Laboratory results | Normal range |
|---|---|---|
| CRP | 3.8 mg/dL | < .5 mg/dL |
| ESR | >140 mm/Hr | 0-20 mm/Hr |
| IgG | 2,134 mg/dL | 635-1741 mg/dL |
| Histone Antibody | 11.5 units | < .9 units |
| ANA antibody | 1:1280 titer | < 1:80 titer |
| Anti dsDNA | 1:160 titer | < 1:10 titer |
| Complement C3 | 58 mg/dL | 90 - 230 mg/dL |
| Complement C4 | < 8 mg/dL | 10 - 51 mg/dL |
| β2- Microglobulin | 3.9 mg/L | < 2.4 mg/L |
| Cardiolipin Ab G | 18 GPL | < 15 GPL |
| Cardiolipin Ab M | 25 MPL | < 12.5 MPL |
| IL-6 | 84.5 pg/mL | < 17.4 pg/mL |
| SSA/B | Negative | < 1.0 Elisa Units |
| Cryoglobulin | None detected | 100-300 mg/L |
| Cardiolipin Ab A | None detected | < 12 APL |
| HIV | Non reactive | Non reactive |
| Hepatitis C Antibody | Negative | Negative |
On admission, he reported pleuritic chest pain and tightness, shortness of breath, palpitations, and a cough with clear sputum for several weeks. On physical examination, the patient was hypotensive to 116/18 and tachycardic to 138 bpm, his respiratory rate was 16 breaths per minute and he was afebrile. He was notably short of breath and tachycardic. S1 and S2 were heard but distant, with no additional heart sounds, murmurs, rubs, or gallops, JVD was mildly raised. He had decreased breath sounds in the right lower lobe but no wheezes, rales, or rhonchi. Bilateral lower extremities were remarkable for 1+ pitting edema. His initial laboratory findings are mentioned in table 1.
His urinalysis was negative for bacteria, nitrates, and leukocyte esterase but revealed moderate proteinuria (30 mg/dL). Urine albumin to creatinine ratio was elevated (82.7 mg/g) with a normal creatinine and GFR. A kidney biopsy was scheduled for further investigation of his moderate proteinuria.
Electrocardiogram (Figure 2) at the time revealed sinus tachycardia with a rate of 134 beats per minute with low voltage QRS but no evidence of electrical alternans.
A chest x-ray (Figure 3) revealed cardiomegaly with bilateral pleural effusions. In the setting of an elevated D-dimer, he underwent Computed tomography (CT) PE which was negative for a pulmonary embolism but demonstrated a 3.3 cm pericardial effusion, moderate right and left pleural effusions, and a small amount of ascites.
Cardiology was consulted and a 2D echocardiogram was ordered and revealed a Left Ventricular Ejection Fraction (LVEF) of 60% with a moderately sized pericardial effusion (Figure 4).
In the setting of a moderate pericardial effusion and the patient’s persistent tachycardia, cardiology suspected cardiac tamponade may develop. Cardiothoracic surgery (CTS) created a subxiphoid pericardial window and inserted a right thoracostomy tube for drainage of fluid. Patient reported improvement in his shortness of breath and pleuritic chest pain. A pericardial biopsy was completed and pericardial serology revealed no malignant cells on cytology and cells with focal mesothelial changes. He was started on Lopressor 12.5 mg bid for tachycardia and Lisinopril 20 mg for its antiproteinuric effect. Given the patient’s history of Raynaud’s phenomenon, with a new pericardial effusion, hypoalbuminemia, bilateral lower extremity swelling, and anemia, a rheumatologic workup was initiated, results mentioned in (table 2).
Patient was started Solumedrol 60 mg every 8 hours initially in the hospital. Kidney biopsy showed no evidence of glomerular global sclerosis, segmental sclerosis, or active glomerulonephritis, immune complex deposition disease by immunofluorescence or electron microscopy. Staining for IgA, IgM, C1q, C3, C4, fibrinogen, kappa, and lambda were negative.
In the setting of serositis, hypocomplementemia, hypoalbuminemia, proteinuria, anemia of chronic disease with a positive ANA, dsDNA, anti-Histones Ab, the diagnosis of Systemic Lupus Erythematosus (SLE) was made and the patient was started on Hydroxychloroquine 400 mg daily, Prednisone 60 mg daily and scheduled to follow up outpatient for further management.
Discussion
The genesis of the chronic, multisystemic illness known as systemic lupus erythematosus (SLE), which has a wide range of clinical symptoms, remains unclear. The development of SLE is influenced by a number of immunopathogenic mechanisms [3]. When a genetically vulnerable person is exposed to environmental variables, a break in their tolerance results in the activation of their autoimmune system. The immune system is exposed to self-antigens as a result of cell damage brought on by infectious agents and other environmental variables [9]. This activation of T and B cells causes a persistent immunological response that is specifically directed against the damaged cells. Organ damage results from the release of cytokines, activation of complement, and generation of autoantibodies.
SLE commonly affects the heart. Heart-related issues will affect around half of SLE patients. The most common cardiac problems in SLE patients are pericarditis, myocarditis, valve issues, thrombosis, and anomalies of the conduction system [10]. Pericarditis, which has been associated with poor mortality, is the most frequent cardiac symptom of SLE. Approximately 25% of all SLE patients eventually have symptomatic pericarditis, most often in association with concurrent pleuritis [11]. In SLE, pericardial effusion is often mild and hemodynamically unimportant. Even though pericarditis is widespread, cardiac tamponade is a rare and unusual illness that is estimated to impact fewer than 1% of SLE patients. As the first symptom of SLE, it is a startlingly uncommon event.
Only 9 of the 41 SLE patients who presented with pericardial effusion in retrospective research that examined cases from 1985 to 2006 had cardiac tamponade [12]. Each of them was a female. Despite receiving high dosage corticosteroid therapy, five of them needed a pericardial window. Low blood C4 levels, being a woman, having concomitant renal illness, hemolytic anemia, and pleurisy were revealed to be the most probable predictors of tamponade in SLE patients who present with pericarditis and pericardial effusions. Systemic sclerosis and SLE have the greatest rates of pericardial involvement (60%) among the other connective tissue disorders [13].
When a pericardial effusion reaches a critical level and restricts cardiac inflow, resulting in hemodynamic compromise, it becomes a medical emergency known as cardiac tamponade. Immune complex inflammation brought on by lupus-related active lupus causes cardiac tamponade in SLE patients. A decrease in cardiac output and systemic venous congestion are the causes of tamponade’s clinical symptoms [14]. Cardiac tamponade is a relatively uncommon first symptom of SLE. Hypotension, dyspnea, orthopnea, chest discomfort, pulsus paradoxus, and jugular venous distension are typical symptoms and indicators.
Echocardiography is used to confirm the diagnosis. If feasible, have an echocardiogram done since it can grade and localize pericardial effusions, identify pericardial thickness, and spot intrapericardial adhesions in addition to being the gold standard for confirming cardiac tamponade [10]. The primary echocardiographic signs of pericardial tamponade include pericardial effusion, diastolic right ventricular collapse, systolic right atrial collapse, inferior vena cava plethora with little respiratory variation, and exaggerated respiratory cycle variation in mitral and tricuspid valve in-flow velocities [15].
Pericardiocentesis is a good option for large effusions, but recurrence is frequent and in that case a less invasive procedure called pericardial window can be used in which a fistula is made connecting pericardial space with pleural space with the benefit of being able to perform tissue biopsy of the pericardium and preventing recurrences. After pericardiocentesis and steroid medication, pericardiectomy is another option if there is a subsequent buildup of pericardial fluid. This procedure is also useful in averting the development of constrictive pericarditis symptoms in the future [16].
In individuals with various connective tissue disorders, pericarditis is an uncommon hemodynamic consequence that may be effectively treated with NSAIDS and corticosteroids [17]. Although pericardial illness is seen often in autopsies and echocardiograms, there may be another explanation for the low prevalence of tamponade. Pericardiocentesis is only performed in cases of tamponade that poses a serious risk to life and persistent massive pericardial effusion. Those who don’t react need a pericardial window. When pericardiocentesis is not practicable, intravenous immunoglobulins are another therapy option [12]. Cardiac tamponade in systemic lupus erythematosus should be treated with high dosage steroids and pericardiocentesis.
Conclusion
A connective tissue condition known as systemic lupus erythematosus (SLE), it presents a wide range of clinical symptoms. By producing immunological complexes and autoantibodies, it damages organs, including the heart. The majority of SLE patients have cardiac involvement, however cardiac tamponade has very rarely been observed, particularly as the first sign of systemic lupus erythematosus (SLE), a potentially fatal consequence brought on by the inflammation of immune complexes generated during active lupus.
References
- A. Kuhn and A. Landmann, “Systemic Lupus Erythematosus,” Eur. Handb. Dermatological Treat. Third Ed., pp. 547–560, Jul. 2022, doi: 10.1007/978-3-662-45139-7_55.
- L. Rönnblom and D. Leonard, “Interferon pathway in SLE: one key to unlocking the mystery of the disease,” Lupus Sci. Med., vol. 6, no. 1, p. e000270, Aug. 2019, doi: 10.1136/LUPUS-2018-000270.
- R. P. Goswami, G. Sircar, A. Ghosh, and P. Ghosh, “Cardiac tamponade in systemic lupus erythematosus,” QJM An Int. J. Med., vol. 111, no. 2, pp. 83–87, Feb. 2018, doi: 10.1093/QJMED/HCX195.
- L. T. Hiraki, S. M. Benseler, P. N. Tyrrell, E. Harvey, D. Hebert, and E. D. Silverman, “Ethnic differences in pediatric systemic lupus erythematosus,” J Rheumatol, vol. 36, no. 11, pp. 2539–2546, Nov. 2009, doi: 10.3899/jrheum.081141.
- R. Alghareeb, A. Hussain, M. V Maheshwari, N. Khalid, and P. D. Patel, “Cardiovascular Complications in Systemic Lupus Erythematosus,” Cureus, Jul. 2022, doi: 10.7759/CUREUS.26671.
- N. Morel et al., “Colchicine: A simple and effective treatment for pericarditis in systemic lupus erythematosus? A report of 10 cases,” Lupus, vol. 24, no. 14, pp. 1479–1485, Dec. 2015, doi: 10.1177/0961203315593169.
- M. Petri et al., “Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus,” Arthritis Rheum., vol. 64, no. 8, pp. 2677–2686, Aug. 2012, doi: 10.1002/ART.34473.
- X. Zhang and W. Wu, “Cardiac tamponade as the initial symptom due to systemic lupus erythematosus in a young man: A case report,” Medicine (Baltimore)., vol. 97, no. 51, Dec. 2018, doi: 10.1097/MD.0000000000013708.
- C. Chourabi et al., “Cardiac tamponade: an uncommon presenting feature of systemic lupus erythematosus (a case-based review),” Pan Afr. Med. J., vol. 36, no. 1, Aug. 2020, Accessed: Sep. 20, 2022. [Online]. Available: https://www.ajol.info/index.php/pamj/article/view/216792
- C. Chourabi et al., “Cardiac tamponade: An uncommon presenting feature of systemic lupus erythematosus (a case-based review),” Pan Afr. Med. J., vol. 36, pp. 1–5, May 2020, doi: 10.11604/PAMJ.2020.36.368.25044.
- A. Umer, S. Bhatti, and S. Jawed, “Sub-acute Cardiac Tamponade as an Early Clinical Presentation of Childhood Systemic Lupus Erythematosus: A Case Report,” Cureus, vol. 10, no. 10, Oct. 2018, doi: 10.7759/CUREUS.3478.
- W. Li, T. Frohwein, and K. Ong, “Cardiac tamponade as an initial presentation for systemic lupus erythematosus,” Am. J. Emerg. Med., vol. 35, no. 8, pp. 1213.e1-1213.e4, Aug. 2017, doi: 10.1016/J.AJEM.2017.04.075.
- M. Petri et al., “Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus,” Ar thritis Rheum, vol. 64, no. 8, p. 2677, Aug. 2012, doi: 10.1002/art.34473.
- S. S. Maharaj and S. M. Chang, “Cardiac tamponade as the initial presentation of systemic lupus erythematosus: A case report and review of the literature,” Pediatr. Rheumatol., vol. 13, no. 1, pp. 1–7, Mar. 2015, doi: 10.1186/S12969-015-0005-0/TABLES/2.
- X. Zhang and W. Wu, “Cardiac tamponade as the initial symptom due to systemic lupus erythematosus in a young man: A case report,” Med. (United States), vol. 97, no. 51, Dec. 2018, doi: 10.1097/MD.0000000000013708.
- A. Emorinken, M. O. Dic-Ijiewere, and H. O. Izirein, “Cardiac Tamponade, an Unusual First Presentation of Systemic Lupus Erythematosus: A Case Report in a Rural Tertiary Hospital,” Cureus, vol. 14, no. 8, Aug. 2022, doi: 10.7759/CUREUS.27989.
- P. D. López, R. Valvani, S. Mushiyev, F. Visco, and G. Pekler, “Cardiac Tamponade: An Unusual Presentation of Systemic Lupus Erythematosus,” Am. J. Med., vol. 131, no. 5, pp. e189–e190, May 2018, doi: 10.1016/J.AMJMED.2017.11.030.