
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Fatal gastric mucormycosis in a liver transplant recipient
with thrombotic microangiopathy
Aashna Gandhi*; Pawan Hanchnale; Geethu Joe; Rajeev Soman
Jupiter Hospital, Pune, India.
*Corresponding Author : Aashna Gandhi
Infectious Diseases Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +91-987-001-8310;
Email: aashnagandhi2206@gmail.com
Received : Nov 02, 2022
Accepted : Nov 21, 2022
Published : Nov 28, 2022
Archived : www.jcimcr.org
Copyright : © Gandhi A (2022).
Abstract
Gastric mucormycosis is a rare but an often fatal form of mucormycosis. Immunocompromised patients are at a risk of this form of mucormycosis. This is a case report of a 53 year old liver transplant patient who developed gastric mucormycosis, possibly due to tacrolimus related thrombotic microangiopathy which led to mucosal damage of the lining of the stomach.
Keywords: Gastric mucormycosis; Liver transplant; Thrombotic microangiopathy.
Citation: Gandhi A, Hanchnale P, Joe G. Fatal gastric mucormycosis in a liver transplant recipient with thrombotic microangiopathy. J Clin Images Med Case Rep. 2022; 3(11): 2173.
Introduction
Infections in solid organ transplant patients can prove to be devastating and managing them can be a very daunting task [1]. A systematic review of not only the current status of immunosuppression but the drugs received peri-transplant is important, as they may reveal their effects several months later. Mucormycosis is caused by ubiquitous fungi belonging to the order Mucorales. Common forms of mucormycosis include Rhino-orbital-cerebral and pulmonary; gastrointestinal mucormycosis is very uncommon, out of which stomach involvement is the most common, followed by that of the colon and ileum [2].
Case presentation
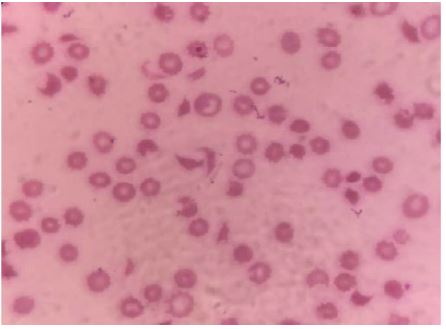
A 53 year old non diabetic, non hypertensive, chronic alcoholic patient with decompensated chronic liver disease underwent live related liver transplant. He received basiliximab and methylprednisolone as induction, followed by Tacrolimus, Mycophenolate Mofetil and Prednisolone for maintenance. Post transplant, he developed Thrombotic Microangiopathy (TMA) likely related to tacrolimus [3] as depicted by schistocytes in the peripheral smear (Figure 1).
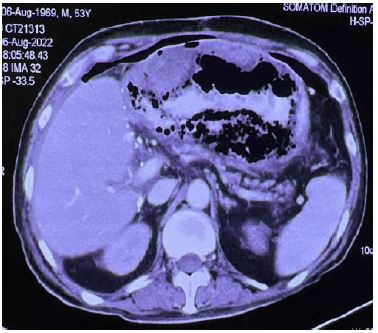
Tacrolimus was substituted with everolimus and he was also given 2 doses of eculizumab and discharged. A few days later he presented to the emergency room with fever, breathlessness and hematemesis. The CT abdomen (Figure 2) revealed the presence of hyperdense thickened and heterogenous anterior wall of stomach in the region of body, with intra-mural air locules, along with pneumoperitoneum in the upper abdomen.
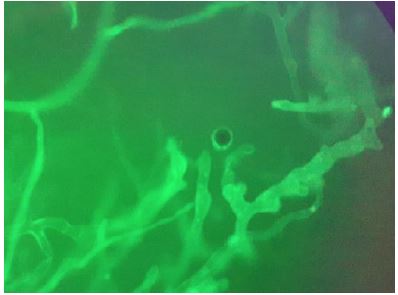
Upper gastrointestinal endoscopy revealed a necrotic stomach wall and blood clots (Figure 3).

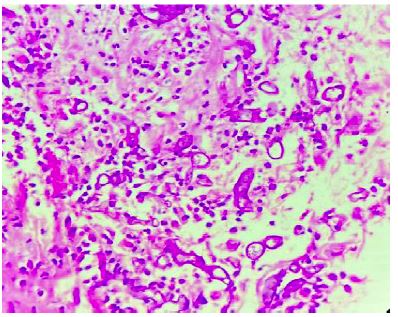
The biopsy revealed broad, pauciseptate hyphae with wide angle branching typical of Mucorales (Figure 4).
The histopathology revealed similar hyphae with vascular invasion (Figure 5).
Treatment with IV Isavuconazole was initiated. Liposomal Amphotericin B was not chosen as the patient had developed kidney injury due to unremitting TMA.
Gastrectomy and esophago-jejunostomy was done, as depicted via intra-operative resected specimen (Figure 6) and Amphotericin deoxycholate was instilled locally.

Despite multiple sessions of plasmapharesis and further doses of eculizumab, TMA was unremitting and the patient succumbed to multiorgan dysfunction and likely progression of mucormycosis.
Discussion
Mucorales are ubiquitous fungi which occur naturally in the environment, found usually in decaying vegetations and soil. They belong to the order Mucorales. Various species include Rhizopus, Mucor, Rhizomucor, Cunninghamella, Absidia (now reclassified as Lichtheimia), Saksenaea, and Apophysomyces. Hyphae of Mucorales are typically broad, pauciseptate and irregularly branched. Rhino-orbital-cerebral and pulmonary forms are common, however, gastrointestinal is a rare form of mucormycosis. Among the gastrointestinal sites, stomach involvement is the most common, followed by that of the colon and ileum [2]. The various risk factors for developing this disease include diabetes mellitus, especially ketoacidosis, glucocorticoid therapy, haematological malignancy, hematopoietic cell transplant, solid organ transplant, deferoxamine treatment, iron overload, COVID-19 infection, etc [4]. Gastrointestinal mucormycosis likely occurs due to ingestion of spores. Usual presentations are abdominal pain and hematemesis [2]. Necrotic ulcers can occur, leading to perforation and peritonitis. In this patient it is plausible that microvascular occlusion due to TMA, mucosal ischemia, severe immunosuppression and ingestion of spores present in some common foods [5] may have led to gastric mucormycosis. Successful management of all forms of mucormycosis requires both extensive and thorough surgical debridement as well as appropriate antifungal therapy. Liposomal amphotericin B is the current drug of choice [6] followed by posaconazole/isavuconazole as alternative /stepdown/salvage therapy [7,8]. Progression of disease despite radical surgery [9] and antifungals in this patient was possibly due to the fact that the underlying condition did not allow reduction of immunosuppression, which is a crucial component of therapy for mucormycosis.
Declarations
Acknowledgements: Division of gastroenterology & hepatobiliary surgery, Department of histopathology, Management, Jupiter hospital, Pune.
Funding: None.
References
- Shoham S. Emerging fungal infections in solid organ transplant recipients. Infectious Disease Clinics. 2013; 27: 305-316.
- Spellberg B. Gastrointestinal mucormycosis: An evolving disease. Gastroenterology & hepatology. 2012; 8: 140.
- Al-Nouri ZL, Reese JA, Terrell DR, Vesely SK, George JN, et al. Drug-induced thrombotic microangiopathy: A systematic review of published reports. Blood, the Journal of the American Society of Hematology. 2015; 125: 616-618.
- Mcnulty JS. Rhinocerebral mucormycosis: Predisposing factors. The Laryngoscope. 1982; 92: 1140-1143.
- Naqvi HA, Yousaf MN, Chaudhary FS, Mills L. Gastric mucormycosis: An infection of fungal invasion into the gastric mucosa in immunocompromised patients. Case reports in gastrointestinal medicine. 2020; 2020.
- Cornely OA, Alastruey-Izquierdo A, Arenz D, Chen SC, Dannaoui E, et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. The Lancet infectious diseases. 2019; 19: e405-421.
- Marty FM, Ostrosky-Zeichner L, Cornely OA, Mullane KM, Perfect JR, Thompson, et al. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. The Lancet infectious diseases. 2016; 16: 828-837.
- Soman R, Chakraborty S, Joe G. Posaconazole or isavuconazole as sole or predominant antifungal therapy for COVID-19-associated mucormycosis. A retrospective observational case series. International Journal of Infectious Diseases. 2022; 120: 177-178.
- Lee SH, Son YG, Sohn SS, Ryu SW. Successful treatment of invasive gastric mucormycosis in a patient with alcoholic liver cirrhosis: A case report. Experimental and therapeutic medicine. 2014; 8: 401-404.