
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Nocardia beijingensis: An elusive diagnosis,
but a favourable outcome
Geethu Joe; Sourabh Chakraborty; Rajeev Soman; Shailesh Rohit; Aashna Gandhi*
Jupiter Hospital, Pune, India.
*Corresponding Author : Aashna Gandhi
Infectious Diseases Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +91-987-001-8310;
Email: aashnagandhi2206@gmail.com
Received : Nov 02, 2022
Accepted : Nov 22, 2022
Published : Nov 29, 2022
Archived : www.jcimcr.org
Copyright : © Gandhi A (2022).
Abstract
A 71 year old male, diabetic; had cough, low-grade fever with significant weight loss. A lesion along the mediastinal surface of the lung was seen. CT guided biopsy showed acute suppurative inflammation. Tuberculosis, Melioidosis, Mould infection, Nocardia & Actinomycosis were in the differential diagnosis and was treated with Doxycycline. However, 2 months later, abdominal discomfort with fever developed and a new necrotic lesion had developed in the right adrenal gland. Biopsy revealed Nocardia beijingensis, identified by MALDI TOF MS. Treatment with TMP SMX & Linezolid led to cure.
Keywords: Nocardia beijingensis; Posaconazole; Diagnostic difficulty.
Abbreviations: MALDI TOF MS: Matrix-Assisted Laser Desorption/Ionization-Time of Flight Mass Spectrometry; TMP SMX: Trimethoprim Sulfamethoxazole; ID: Infectious Diseases; DST: Drug Susceptibility Testing.
Citation: Joe G, Chakraborty S, Soman R, Rohit S, Gandhi A. Nocardia beijingensis: An elusive diagnosis, but a favourable outcome. J Clin Images Med Case Rep. 2022; 3(11): 2174.
Introduction
Nocardia are aerobic bacteria that belong to the order Actinomycetales. They usually spread via inhalation, but ingestion and direct inoculation are other modes of entry. Up to 54 species of Nocardia have been identified in causing human disease. Nocardia bejingensis was first isolated in 2001. This case is presented to highlight diagnostic difficulties & various tests that are needed to identify & speciate a rare pathogen.
Case report
A 71 year old male, resident of North Gujarat, was diabetic for 10 years & well controlled on oral hypoglycemic agents. In Nov 2020 cough, dyspnea, intermittent low-grade fever started & was accompanied by a weight loss of 8 kilograms over the next 3 months. X-Ray chest showed a left upper zone lesion & was evaluated by an oncosurgeon & referred for ID opinion elsewhere. Total Leukocyte count was found to be 20000/ mm3, Procalcitonin normal, Beta-D-Glucan < 7 pg/ml and a CT scan PET CT & CT guided biopsy had been done. 1 month later the patient presented to Jupiter Hospital for ID opinion. On review of CT scan a heterogeneously enhancing lesion along the mediastinal surface of left upper lobe of the lung was seen encasing the aorta & left subclavian artery (Figure 1). Loss of fat planes had occurred between the lesion, esophagus & trachea, along with tiny sub centimetric nodules in the apico-posterior segment of the left lung & enlarged, heterogeneously enhancing lymph nodes in the mediastinum. This had been reported as indicative of neoplastic etiology.
PET scan had shown a high grade, metabolically active lesion along with bony erosion, para vertebral soft tissue extension (Figure 2).
About the use of antibiotics, a 5-day course of Amoxicillinclavulanic acid had been given around the time of CT guided biopsy & there was a brief improvement in fever. Various possibilities were considered (Table 1).
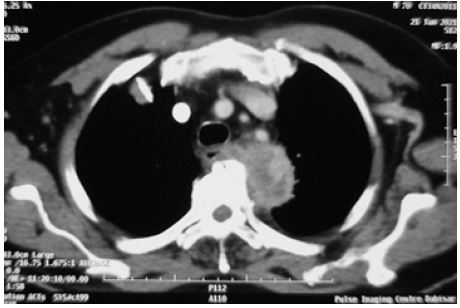
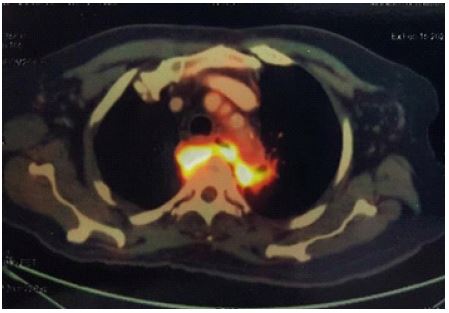
Table 1: High grade, metabolically active lesion along with bony erosion, para vertebral soft tissue extension on PET CT.
| Chroni c infecti on | Tissue planes transgress ed | Suppurati on | fistul a | Partial response to Amoxicilli n- Clavulanicacid | Predisposig factor | |
|---|---|---|---|---|---|---|
| Tuberculosis | ✓ | +/- | X | ✓ | X | Diabetes mellitus |
| Gene Xpert MTB/Ultr a –ve | ||||||
| ✓ | ✓ | ✓ | Diabetes mellitus | |||
| Mould infection | +/- | +/- | X | +/- | X | No severe immunocompromise |
| Nocardia | ✓ | ✓ | ✓ | ✓ | Diabetes mellitus, but no steroids | |
| Actinomycosis | ✓ | ✓ | ✓ | ✓ | ✓ | Aspiration, injury to esophagus |
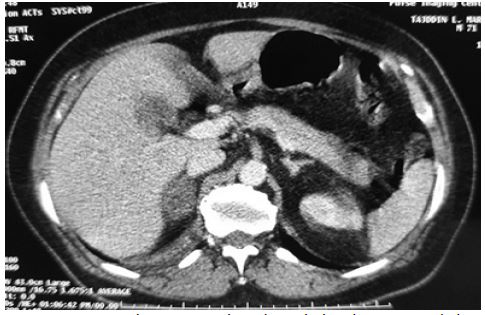
The 2 main possibilities considered were Actinomycosis & Nocardia, of which Actinomycosis was considered more likely. Actinomycosis can result from aspiration & involve the lung, but left apicoposterior site is not common for aspiration & the patient’s dentition was good. On specific inquiry the patient had a vague recollection of a fish bone esophageal injury during swallowing. It is possible that this could have introduced the organism into tissue. Disease could have been primarily in the mediastinum with invasion of the apico-posterior segment of the lung. CT guided biopsy may have been too small to detect Splendore-Hoeppli phenomenon & anaerobic cultures may not have been done to provide a diagnosis of Actinomycosis. Hence Amoxicillin was started empirically & was changed to Doxycycline due to diarrhea. However, 2 months later, abdominal discomfort with mild fever developed. Imaging showed that the chest & paravertebral lesions had remained static but a new necrotic lesion had developed in the right adrenal gland (Figure 3)
Since this was not in contiguity with the previous lesions, as would be expected with Actinomycosis, the diagnosis was reviewed. Nocardia which had been the next likely possibility produces multi focal non-contiguous lesions & literature search revealed a case report of an adrenal abscess due to Nocardia [1]. CT guided biopsy was done but very little material could be obtained. However culture on LJ medium grew matt, dry, crumbly, adherent colonies (Figure 4) [2].
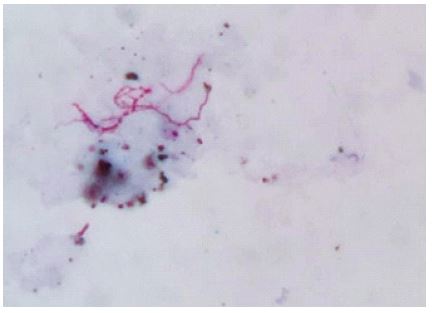
Gram staining showed thin, delicate, weakly gram-positive, irregularly stained or beaded branching filaments (Figure 5) [3].
MALDI TOF MS identified the isolate as Nocardia beijingensis. DST showed susceptibility to Ceftriaxone, TMP-SMX & Line zolid which was concordant with the findings by BertránLópez J et al [4]. The patient refused intravenous treatment & was treated with TMP SMX (160/800 mg) & Linezolid (600 mg) daily for 1 month & continued TMP SMX (160/800 mg) further for 1 year with good recovery.

Discussion
Nocardia bejingensis was first isolated in 2001. The first human infections were reported in Asia and subsequently, cases were reported from Europe and few cases were reported from United States but it has been infrequently cited in the literature [5]. Nocardia are aerobic bacteria that belong to the order Actinomycetales. They usually spread via inhalation, but ingestion and direct inoculation are other modes of entry. Up to 54 species of Nocardia have been identified in causing human disease, Nocardia beijingensis is a rare type. Immunocompromised patients are at a high risk for infection with Nocardia spp. Common sites of involvement are lungs, central nervous system and skin. Nocardia are delicate, filamentous, beaded, branching, gram positive rods. They are also partially acid fast. Although routine media support the growth of Nocardia, special media like buffered charcoal yeast extract, modified Tm agar and LJ media may be used to increase yield. Further speciation can be done via MALDI-TOF MS as in this case or other techniques like 16s RNA sequencing. Antibiotics usually used are TMP-SMX, amikacin and 3rd generation cephalosporins. Severe disease may warrant usage of more than one agent until susceptibility testing results are awaited. Appropriate interpretation of history, radiologic findings, histology, partial response to previously received therapy & immune status may point to certain diagnoses. Lack of response to a therapeutic trial, development of additional lesions & literature search for rare sites of involvement can help. The physician must have diagnostic flexibility & be willing to revisit the diagnostic considerations. Adrenal biopsy is often technically difficult & the scanty material obtained has to be prioritized for various microbiological & histopathological tests with advice from the laboratory. Identification of the pathogen to species level & DST help in selecting appropriate therapy.
Declarations
Acknowledgements: Management, Jupiter hospital, Pune.
Funding: None.
References
- Chong YL, Tan JK, Teo N. Clinics in diagnostic imaging (109). Singapore medical journal. 2006; 47: 425.
- Khadka P, Basnet RB, Rijal BP, Sherchand JB. Pulmonary nocardiosis masquerading renascence of tuberculosis in an immunocompetent host: A case report from Nepal. BMC research notes. 2018; 11: 1-5.
- Patil SP, Nadkarni NJ, Sharma NR. Nocardiosis: Clinical and pathological aspects. Martinez EP: Histopathology–Reviews and Recent Advances. In Tech. 2012; 81-96.
- Bertrán-López J, Abbott A, Archibald LK, Benninger L, Lascano J, Kalyatanda G, et al. Disseminated Nocardia beijingensis masquerading as pulmonary tuberculosis in a patient with human immunodeficiency virus/acquired immune deficiency syndrome. In Open forum infectious diseases. US: Oxford University Press. 2020; 7: of aa186.
- Moore-Pardo SM, Asquith J, Aslam S, Mayer C, Greene J, Alrabaa S. 1354. Nocardia bejingensis: A Novel Isolate Affecting Immunocompromised Patients in the United States. In Open Forum Infectious Diseases. US: Oxford University Press. 2019; 6: S490-S490.