
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Hepatotoxicity secondary to ribociclib and echinacea: Case report
Clara García González1*; Francisco de Asís Aparisi Aparisi1,2; Martín Núñez Abad1; Silvia Calabuig Fariñas1,2; María Concepción Godes Sanz de Bremond1,2; Vega Iranzo González-Cruz1,2,3; Carlos Camps Herrero1,2,3
1Hospital General Universitario de Valencia, Spain.
2CIBERONC, Spain.
3Facultad de Medicina, Universidad de Valencia, Spain.
*Corresponding Author : Clara García González
Hospital General Universitario de Valencia, Spain.
Ph: +34 639-471645;
Email: claragargon@gmail.com
Received : Nov 02, 2022
Accepted : Nov 22, 2022
Published : Nov 29, 2022
Archived : www.jcimcr.org
Copyright : © González CG (2022).
Abstract
The consumption of medicinal herbs has increased in recent years. There is little evidence with regards to their real benefits and a small number of scientific papers about adverse effects. A case of a 55-year-old woman is presented, with recent diagnosis of luminal A de novo metastatic breast cancer. She starts first-line treatment with Ribociclib in combination with letrozole. After 2 months, a partial response is achieved. However, the patient presents grade 4 hepatotoxicity. She had started to take Echinacea two months ago. Other causes of liver failure are ruled out. Both Echinacea and Ribociclib present hepatic metabolism through cytochrome p450, which means that there could be a potential interaction between them. This is the first reported case of a potential interaction between Ribociclib and Echinaea. We highly recommend avoiding the concomitant use of both medications.
Keywords: Hepatotoxicity; Ribociclib; Echinacea; Breast cancer.
Citation: González CG, Aparisi FAA, Abad MN, Fariñas SC, Bremond MCGS, et al. Hepatotoxicity secondary to ribociclib and echinacea: Case report. J Clin Images Med Case Rep. 2022; 3(11): 2175.
Introduction
Herbal medicines are generally considered by the population to be beneficial for health, with no side effects. As a result, consumption of them has increased exponentially in recent years [1]. In particular, Echinacea extracts have several inflammation-related bioactivities. Echinacea is native to North America [2]. There is little information with regards to its real health benefits and adverse effects, as well as interactions with other drugs. A case of a 55-year-old woman is presented, with metastatic luminal a breast cancer and showing severe hepatotoxicity secondary to Ribociclib, which is aggravated by Echinacea. This is the first case reported in the literature about the potential interaction between these two drugs.
Case presentation
A case of a 55 years old woman is presented, with no medical history of interest, and no previous treatment. During a breast cancer screening review, a 5 Centimeter (cm) breast lump was detected. A biopsy was performed, with the result of infiltrating hormone-sensitive ductal carcinoma with a low proliferation index. A mastectomy and axillary lymphadenectomy were performed in May 2018. The definitive pathological anatomy reported an infiltrating luminal ductal carcinoma luminal 2 A-like (Estrogen Receptors (ER) +, Progesterone Receptors (RPg) +, Ki67 10%, factor receptor 2 Human Epidermal Growth (HER2)) -) pT3pN3a. An extension study was carried out, which showed lung metastatic micronodules in both hemithorax and multiple liver and bone metastases. In June 2018 the patient started treatment with Ribociclib 600 mg/day for 21 days every 28 day, letrozole 2.5 mg/day and zoledronic acid each 28 days as a first line treatment for advanced luminal breast cancer treatment.
After two cycles a partial response was achieved (August 2018). However, there was a grade 4 liver toxicity, requiring drug discontinuation with jaundice, asthenia and gastric discomfort. Physical examination highlighted jaundice and painless hepatomegaly.
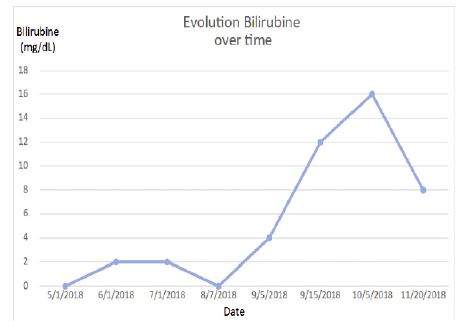
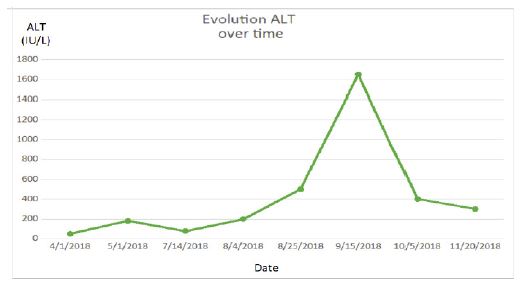
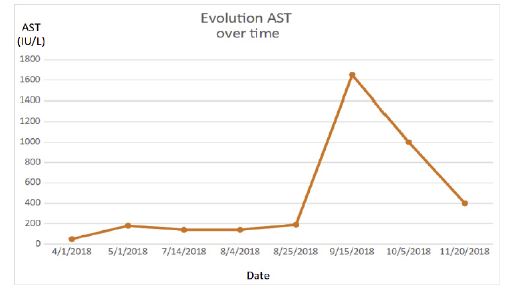
In the blood test stands out bilirubin 14,52 mg/dL (normal < 1.1 mg/dL) (Figure 1), Alanine Aminotransferase (ALT) 1.101 IU/L (Figure 2) and Aspartate Aminotransferase (AST) 1.330 IU/L (normal < 31 IU/L) (Figure 3), Gamma Glutamyl Transferase (GGT) 223 IU/L (normal < 36 IU/L), Lactate Dehydrogenase (LDH) 622 IU/L (normal < 350 IU/L). All other tests, including albumin, iron, ferritin, ceruloplasmin, copper, alpha-1 antitrypsin, and immunoglobulin G were within the normal range. Viral hepatitis markers as well as antibodies for other hepatotropic viruses, Human Immunodeficiency Virus (HIV) test, anti-smooth muscle antibody, antinuclear antibodies, antimitochondrial antibodies, anti-soluble liver antigen antibodies and anti-liver/kidney antibodies were all negative.
Ultrasound revealed a multi-metastatic liver with no evidence of intra- and extrahepatic bile duct dilation. A liver biopsy could not be performed due to severe liver failure, with high risk of bleeding from coagulopathy.
The first diagnostic guess is hepatotoxicity due to Ribociclib. However, in the directed anamnesis the patient reported having taken royal jelly and liquid Echinacea (1 ml every 8 hours) as complementary medication since June 2018.
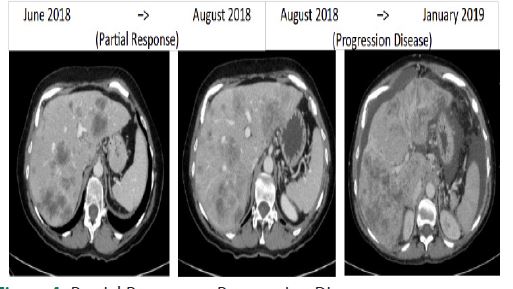
In August 2018, after a partial response, Ribociclib was discontinued due to grade 4 liver toxicity. Hospital admission was required for symptomatic treatment and to rule out other causes of liver failure. In October 2018, CT scan showed progression disease (increased ascitic fluid and a slight new pleural effusion) (Figure 4).
The patient stopped taking Echinacea in October 2018. In November 2018, blood tests showed slight improvement of hepatitis, persisting bilirubin 7.93, ALT 291, AST 297, GGT 116. The patient followed treatment with letrozole. In January 2019 there was a disease progression with increased size and number of liver and lung metastases. She started a second line treatment with fulvestrant [3]. Finally, the patient was admitted to the hospital due to signs of liver failure and pain, with a visceral crisis in April 2019. It was decided to limit therapeutic effort and palliative symptomatic treatment. At the end, the patient died of breast cancer in a situation of disease progression.
Discussion
Derivatives of the genus Echinacea are widely used as herbal medication, being one of the most popular herbal medicines in Europe and North America. Data from the 2012 National Health Interview Survey Alternative Medicine Supplement showed that 17.7% of United States adults had used natural products in the previous year, being 0.9% Echinacea (percentages are the rate of use among United States adults) [1].
There are approximately 9 species of Echinacea. Extracts of Echinacea purpurea, pallida and angustifolia are the most frequently used [2]. Moreover, there are three major groups of chemical components in Echinacea plants: alkamides, caffeic acid derivatives and polysaccharides [3].
Echinacea spp have some inflammation-related bioactivities, such as modulating chemokine and cytokine production and inhibiting Cyclooxygenase (COX) activity [4]. Specifically, Echinacea alkamides are characterized by modulating the expression of tumor necrosis factor α, and seem to be the main phytochemicals responsible for the anti-inflammatory effects of Echinacea [3]. They also stimulate the immune system. Therefore, Echinacea is used to treat and prevent the common cold and other upper respiratory diseases [5], although there is slight evidence for its therapeutic effectiveness.
In most of the cases, it is well tolerated and has no major adverse events, mainly gastrointestinal upset and skin rashes [6,7]. Nonetheless, there are some isolated cases reported in the literature of toxic hepatitis attributed to Echinacea, with liver injury in the form of jaundice, increased bilirubin or transaminases. The most frequent pathological findings in biopsy of liver toxicity due to Echinacea are interface hepatitis, prominent cholestasis and portal lymphoplasmacytic and eosinophilic granulocyte infiltration. In two cases, hepatitis with jaundice arose 1 to 3 weeks after starting Echinacea extracts with a rapid recovery on stopping [8]. In the case presented, the toxicity begins 3 weeks after starting Echinacea. When the patient stops taking it, there is only a partial improvement.
Echinacea metabolism is mainly through cytochrome P450 enzymes. Epoxide formation, N-dealkylation and hydroxylation are the main metabolic pathways mediated by P450. Interactions with P450 determine the circulating concentrations and duration of action of these components, as well as any potential interactions with other chemicals [9]. As a consequence, patients taking herbal 4 supplements that are concomitantly taking other medications have an increased risk of pharmacokinetic interaction, either inhibition or induction of the metabolism of drugs catalyzed by the cytochrome P450 (CYP). However, data about interactions of Echinacea with CYP enzymes are scarce. On the other hand, pharmacodynamics interactions consist of additive outcomes or antagonistic ones [2].
Echinacea selectively modulates the catalytic activity of CYP3A at hepatic and intestinal sites. The type of drug interaction observed between Echinacea and other CYP3A substrates will depend on the relative extraction of drugs at hepatic and intestinal sites [10]. On the one hand, the available in vivo evidence shows significant clinical evidence of the potential of Echinacea to induce hepatic CYP3A4 activity [2]. On the other hand, Echinacea derivatives can also inhibit the intestinal metabolism of CYP3A4 drugs. Because of that, caution should be taken when CYP3A4 drugs with low oral bioavailability due to pronounced intestinal CYP3A4-mediated metabolism or CYP3A4 drugs with narrow therapeutic index are co-administered with Echinacea derivatives.
Ribociclib is an orally Cyclin-Dependent Kinase (CDK) 4/6 inhibitor, which is approved for first line treatment of hormone-receptor-positive metastatic breast cancer. Other CDK 4/6 inhibitors are palbociclib and abemaciclib.
Phase III clinical trials show a higher incidence of hepatotoxicity, compared to placebo (23.2% versus 16.5%). 7 to 10% of patients treated with Ribociclib had grade 3 or 4 elevations in transaminases and 1 % had bilirubin increased. Hepatotoxicity due to Ribociclib appears within 6 months after starting the treatment. The median time to resolution (until normalization or grade ≤2) was 22 days in the Ribociclib arm plus any combination [11].
Interruptions and/or dose adjustments due to hepatobiliary toxicity events were reported in 10.4% of patients treated with Ribociclib plus any combination, mainly due to increased transaminases (ALT 6.9% and AST 6.1%). Discontinuations of this drug due to abnormal liver function tests or hepatotoxicity were observed in 2.3% of Ribociclib arm versus 0.4% of placebo arm [11].
Ribociclib is primarily eliminated by hepatic metabolism through CYP3A4. The main metabolic pathways for Ribociclib involved oxidation (alkylation, C and/or N oxygenation, oxidation (-2H)) and combinations thereof. Phase II conjugates of phase I metabolites of Ribociclib involved N-acetylation, sulfation, cysteine conjugation, glycosylation, and glucuronidation. 5 In vitro, Ribociclib is a reversible inhibitor of CYP1A2, CYP2E1, and CYP3A4/5 and a time-dependent inhibitor of CYP3A4/5 [12].
Here we present a case of liver toxicity as an adverse event of Ribociclib is presented, which is aggravated by taking Echinacea. This is the first case published in the literature. Echinacea is metabolized by cytochrome P450, and Ribociclib is a CYP3A4 inhibitor, so there could be a potential interaction between the drug and the medicinal herb. Echinacea-induced hepatitis is an extremely rare toxicity. Its diagnosis is often delayed and requires a high level of suspicion.
Conclusion
To conclude, although adverse events secondary to herbal drugs are uncommon, the general population should be aware of this serious toxicity, especially when other drugs are taken concomitantly.
References
- Clarke TC. Trends in the Use of Complementary Health Approaches Among Adults: United States, 2002–2012. 2015: 21.
- Wanwimolruk S, Prachayasittikul V. CYTOCHROME P450 ENZYME MEDIATED HERBAL DRUG INTERACTIONS (PART 1). EXCLI Journal. 2013: 45.
- Hou CC, Huang CC, Shyur LF. Echinacea alkamides prevent lipopolysaccharide/D-galactosamine-induced acute hepatic injury through JNK pathway-mediated HO-1 expression. J Agric Food Chem. 2011; 59: 11966-11974.
- Sullivan AM, Laba JG, Moore JA, Lee TDG. Echinacea-Induced Macrophage Activation. Immunopharmacology and Immunotoxicology. 2008; 30: 553–574. https://doi.org/10.1080/08923970802135534
- Sharma M, Anderson SA, Schoop R, Hudson JB. Induction of multiple pro-inflammatory cytokines by respiratory viruses and reversal by standardized Echinacea, a potent antiviral herbal extract. Antiviral Research. 2009; 83: 165-170.
- Barrett B, Brown R, Rakel D, Mundt M. Echinacea for treating the common cold: A randomized controlled trial. 2011; 19: 6
- Karsch-Völk M, Barrett B, Kiefer D, Bauer R, Ardjomand-Woelkart K, Linde K, et al. Echinacea for preventing and treating the common cold. Cochrane Acute Respiratory Infections Group, ed. Cochrane Database of Systematic Reviews. 2014.
- Liver Tox: Clinical and Research Information on Drug-Induced Liver Injury. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Bookshelf URL: https://www.ncbi.nlm.nih.gov/books/
- Toselli F, Matthias A, Gillam EMJ. Echinacea metabolism and drug interactions: The case for standardization of a complementary medicine. Life Sciences. 2009; 85: 97-106.
- Gorski JC, Huang SM, Pinto A, et al. The effect of echinacea (Echinacea purpurea root) on cytochrome P450 activity in vivo. Clin Pharmacol Ther. 2004; 75: 89-100.
- Im SA, Lu YS, Bardia A, et al. Overall Survival with Ribociclib plus Endocrine Therapy in Breast Cancer. n engl j med. Published online 2019:10.
- Hortobagyi GN, Stemmer SM, Burris HA, et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2019; 30: 1842.