
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Combination of PLGF and PAPPA as a biochemical markers to the first trimester maternal screening
Zouhoor M Elbaz1; Magdy M2; Manjunath N1; PK Menon1; Eman M EL-Sayed3; Osamma KZ3
1Genomics Lab, Gulf Medical University Laboratory, GMU, Ajman, UAE.
2Biochemistry Department, Faculty of Science, Ain Shams University Cairo, Egypt.
3Unit of Children Inherit, Faculty of Medicine, Ain Shams University Cairo, Egypt.
*Corresponding Author : Mahmoud Magdy
Biochemistry Department, Faculty of Science, Ain Shams University Cairo, Egypt.
Email: mutation6119@yahoo.com
Received : Sep 19, 2022
Accepted : Nov 22, 2022
Published : Nov 29, 2022
Archived : www.jcimcr.org
Copyright : © Magdy M (2022).
Abstract
Screening of fetal chromosomal abnormalities is an essential part of antenatal care. Effective first trimester screening involves PAPP-A (pregnancy associated plasma protein A) and free HCG (human chorionic gonadotropin) levels in the maternal serum along with ultrasound examination. The objective of this study is to investigate whether the measurement of PLGF (Placental Growth Factor) can improve the performance of first trimester combined screening for Trisomy 21, 18 and 13. A total of 350 samples were collected from pregnant women during the first trimester between 10 to 14 weeks of gestation. The ultrasound (US) data were collected from all cases which include US gestational age, NT value, CRL, and fetus number, if any. Blood samples were collected and tested for PAPP-A and free HCG tests. The combined risk of trisomy 21, 18 and 13 were calculated using PRISCA software. The screen positive cases (more than a defined cutoff rate) were stored at -20oC for PLGF testing. A total of 97 cases, including low and high risk patients were analyzed for PLGF. A significant reduction was observed among the risk group p ≤ 0.005 when compared to the negative control group. A positive correlation between PLGF and PAPPA was identified (r=0.69) p ≤0.001. In conclusion the study provide data indicating that inclusion of serum PLGF improve the performance of first trimester combined test for screening of Trisomy 21, 18 and 13 risk
Keywords: PLGF; First trimester screening; PAPP-A; Free HCG; Combined risk; Trisomy 21; Trisomy 18; Trisomy 13.
Citation: ZM Elbaz, Magdy M, Manjunath N, PK Menon, EL-Sayed EM, et al. Combination of PLGF and PAPPA as a biochemical markers to the first trimester maternal screening. J Clin Images Med Case Rep. 2022; 3(11): 2176.
Introduction
Non-invasive screening based on biochemical analysis of maternal serum or fetal ultrasound measurements, allows estimates of the risk of a pregnancy being affected and provides information to guide decisions about definitive testing. Before agreeing to screening tests, parents need to be fully informed about the risks, benefits and possible consequences of such a test. This includes subsequent choices for further tests they may face, and the implications of both false positive and false negative screening tests (i.e. invasive diagnostic testing, and the possibility that a miscarried fetus may be chromosomally normal). The decisions that may be faced by expectant parents inevitably engender a high level of anxiety at all stages of the screening process, and the outcomes of screening can be associated with considerable physical and psychological morbidity [1].
The first trimester screening involves PAPP-A (pregnancy associated plasma protein A) and free HCG (human chorionic gonadotropin) levels in the maternal serum along with ultrasound examination. The detection rate of these methods is about 85-90% in regard to trisomy 21 and 18, with a false-positive rate of 5% [2]. Fetal nuchal translucency thickness (NT) above the 99th percentile (≥3.5 mm) is associated with a high risk for chromosomal abnormalities, major fetal defects and a wide range of genetic syndromes [3,4]. The levels of both markers are associated with adverse pregnancy outcomes, such as spontaneous loss before fetal viability, gestational hypertension, preeclampsia, preterm premature rupture of membranes, placental abruption, preterm birth, low birth weight, and stillbirth [5,6].
Placental growth factor (PLGF) consider to be a member of the vascular endothelial growth factor family and is implicated in angiogenesis and trophoblastic invasion of the maternal spiral arteries 1-3. PLGF maternal serum levels at 11 to 13 weeks of gestation are decreased in pregnancies with impaired placentation resulting in preeclampsia and neonates with small gestational age (SGA) [7,8].
Recent research highlights the role of PLGF in the screening of fetal chromosomal aneuploidies. In this study we assessed the ability of PLGF to improve the first trimester screening test for trisomy 21, 18 and 13.
Material and methods
A total of 350 blood samples were collected from pregnant women visiting GMU laboratory or received to the lab from other sites of Thumaby labs for prenatal testing during the period of January 2015 to September 2017. Gestational age was maintained for all the cases between 10 to 14 weeks of pregnancy (first trimester). The ultrasound data was collected for all the patients which include US gestational age, NT value, CRL, fetus number and if any other abnormality present in the fetus. Double marker requisition forms were filled with the patient information which include all of the following demographic and clinical information: date of birth; maternal weight; maternal race; smoking history; first day of the last menstrual period or gestational age as determined by ultrasound examination; specimen draw date; initial or repeat specimen; presence of medication-dependent diabetes; family history of neural tube defect, and presence of multiple gestation if known. The sampling date should be within 7 days of the ultrasound.
The samples were tested for PAPPA, free HCG test (double marker test) from pregnant women in the first trimester of gestations using Electro Chemiluminescence Immunoassay (ECLIA) method and analyzed by Immulit 2000xp instrument. The tests were validated before processing the patient samples for precision, accuracy, linearity of the assay and the manufacture reference range was verified. The data was analyzed for risk calculation using PRISCA software which provides statistical risk assessment for Down syndrome (Trisomy 21) and Edwards’s syndrome (Trisomy 18) in the first and second trimesters of pregnancy. The risk for Patau’s syndrome (Trisomy 13) is also reported, together with the risk for Trisomy 18 in the first trimester. The screened positive women samples less than define cutoff value (1:250 for T 21 and 1:100 for T18, 13) were stored at – 20oC for PLGF testing. A total of 95 out of 350 patient samples were analyzed for PLGF which include high and low risk patients. Of these, 65 patients at high risk (35 cases of trisomy 21 and 30 cases of trisomy 18/13) in addition to 30 cases at low risk and used as a negative control group. The assay was analyzed using automated technique of immunefluorescent. The assay is specific for the measurement of human free PLGF. The measurement principle is based on TRACE technology (Time Resolved Amplified Cryptate Emission) which measures the signal that is emitted from an immunecomplex with time delay. The basis of TRACE technology is non-radiative energy transfer from a donor to an acceptor. When two components are bound in an immunecomplex, both the signal amplification and the prolongation of the life span of the acceptor signal occur at 665 nm, so that it can be measured over micro seconds. This long- life signal is proportional to the concentration of the analyte.
Results
Table 1 distributions of all the study cases among the risk groups.
During the study period of January 2015 to September 2017 a 350 pregnant women samples were examined for prenatal screening test. The demographic and sonographic data collected from the pregnant women along with the biochemical marker results of PAPP-A and free HCG were applied for risk calculation of Trisomy 21, 18 and 13 using PRISCA software.
In the study population of 350 cases there were 285 (81.4%) with low risk of trisomy 21, 18 and 13 and 65 (18.57%) with high risk of chromosomal abnormities of trisomy 21 (n= 35) and trisomy 18,13 (n=30). Table (1), shows the distributions of all the cases among different risk groups.
Table 1: Distributions of all the study cases among the risk groups.
| Risks | High Risk (<250) | Intermediate Risk (250-500) | Low Risk (>500) | |
|---|---|---|---|---|
| Biochemical risk for Trisomy 21 | No. | 45 | 33 | 272 |
| % | 12.9 | 9.4 | 77.7 | |
| Total Scan and Biochemical risk for Tr.21 | No. | 35 | 10 | 305 |
| % | 10 | 2.9 | 87.1 | |
| Biochemical risk for Tr.18 | No. | 38 | 16 | 296 |
| % | 10.9 | 4.6 | 84.5 | |
| Total Scan and Scan Biochemical risk for Tr.18 | No. | 30 | 9 | 311 |
| % | 8.6 | 2.6 | 88.9 | |
PRISCA software compares the subject’s serum result with the median for that gestational age to express the result as a multiple of the median (MoM), for PAPP-A, free Beta hCG and NT value. It is able to provide MoMs corrected for variable factors such as gestational age, maternal weight, ethnicity, smoking, twin pregnancy, diabetes and IVF procedures. Once the corrected MoM value is obtained, the likelihood ratio is calculated for each of these values, and the combination of all likelihood ratios with maternal age related risk (a prior risk) yields the final risk assessment. A screen-negative result indicates that the calculated screen risk is below the established cutoff of 1/250 for Down syndrome and 1/100 for trisomy 18. The Socio-demographic Characteristics for all the pregnant women participate in the study was demonstrated in Table 2.
Among 350 patients, 45.8% were in the age group 20-35 years at the time of delivery. Majority of them were Asians (78.7%), 5.9% were diabetic, twins noticed for 9 women and 7 patients conceived after IVF. At the time of sampling, most of the samples (25.6%) were in the gestational age of 12th week followed by 21% of women who were at 11th week. Mean age at the time of delivery observed as 32 years & 8 months (32.8 ± 5.4), age ranges from 20.3 years to 45.1 years among the total samples.
Table 2: Characteristics of the study groups in the screening population.
| Characteristics | Normal | Trisomy 21 | Trisomy 18 |
|---|---|---|---|
| Maternal Age at delivery, years < 35 <= 35 |
162 123 |
11 24 |
12 18 |
| Maternal weight, Kg < 60 Kg >=60 Kg |
165 120 |
12 23 |
4 26 |
| Ethnic origin African Asian Caucasian |
18 237 30 |
6 18 11 |
3 19 8 |
| Diabetes | 21 | 16 | 8 |
| Fetal CRL/mm Median value | 69 | 82.2 | 80.8 |
| Fetal NT/ mm Median value | 0.9 | 2.19 | 2.7 |
| PAPP-A Median value | 2.7 | 1.2 | 0.98 |
| FreeHCG Median value | 30.2 | 55.3 | 11.3 |
| PLGF Median value | 38.8 | 15.6 | 10.4 |
By median test, median of NT MoM, free HCG MoM and PAPP-A MoM were significantly different according to different risk groups (with p value ≤0.05, ≤0.01 and ≤0.001 respectively). Significant reduction observed in PAPP-A value in the risk group of trisomy 21 and trisomy 18, 13 when compare to the no risk group, while significant increase was found in free HCG values among the same risk groups. Tr.21 risk found more among Caucasians, diabetics as well as women with 35 years and above. Age and diabetes has significant association with Tr.21 risk (chi-square test). It is observed that 2.8 times higher chance for Tr.21 risk if the patient is with age above 35 years (significant with p value ≤0.05, CI: 1.04 – 7.6). If the patient is diabetic, 8 times more chance for Tr.21 risk found with statistical significance (p value ≤0.01, CI: 1.87 - 34.89). Tr.18 risk was noticed higher among Caucasians compared to other nationals. Tr.21 risk was prominently seen among the women at the pregnancy period of 3 months and below, specifically at gestational age of 11th week. Similar trend found for Tr.18 in relation to the effect of gestational age.
PLGF test was done for 95 pregnant women with low and high risk. A significant reduction was observed in risk group of trisomy 21 with p≤ 0.005 and p≤0.001 for trisomy 18 & 13, Table 2. Using sensitivity test PLGF shows 90.9% (true positive) of positive results of trisomy 21 and could be correctly identified as positive by PLGF test. Similarly 89% was identified or trisomy 18, 13.
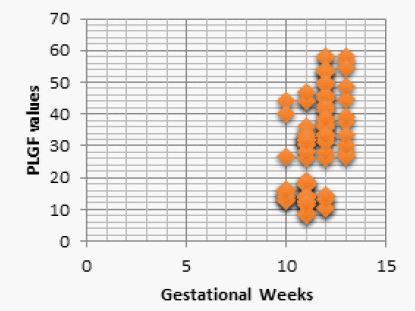
Gestational weeks and PlGF values are positively correlated with correlation coefficient 0.55 and correlation found statistically significant with p value ≤0.001 (by Spearman’s Rank Correlation Test). When weeks increases, PLGF values are also increases and hence positive correlation is identified. A strong positive correlation between PAPPA and PLGF values are observed with correlation coefficient, r=0.93. Correlation is statistically significant with p value ≤ 0.001 (By Spearman Rank Correlation Test). When PAPPA values reduced, PLGF values also proportionally reduced.
Discussion
In normal pregnancy the biochemical marker including PAPP-A, free HCG and PLGF concentration are affected by maternal age, gestational age, maternal weight, racial origin, cigarette smoking and method of conception, and these factor should be taken into consideration before comparing high risk with low risk pregnancies [9]. The concentration of PAPP-A and PLGF in maternal circulation increases with gestational age with double time of 3 to 4 days during the first trimesters, then the level continues to rise throughout pregnancy until delivery.(10) While the maternal serum HCG peaks at 8-10 weeks and then declines to reach a plateau at 18-20 weeks of gestation and remain quiet constant until term [11].
The finding of this study demonstrate that in trisomy 21,18 and 13 pregnancies maternal serum PAPP-A and PLGF at 10 to 14 weeks of gestation are significantly reduced and also affected by maternal age, weight, pre-existing diabetes mellitus and method of conception [12].
While free HCG value was increased in trisomy 21 pregnancies only.
Decreased levels of PAPP-A are found in association with abnormal placental function which has formed the basis for the first trimester screening of fetal Down syndrome [13,14]. PAPP-A is also said to have a positive relationship with birth weight [15]. As PAPP-A decrease, the risk of small gestational age infants increases. Studies have shown that down regulation of insulin- like growth factor II availability due to decrease PAPP-A serum level may be one of the causes of spontaneous abortion in these women [16]. The decrease in PAPP-A is not associated with any change in the placental synthesis of protein, since PAPP-A m RNA expression is not significantly decreased in Down’s syndrome placentas. Furthermore, the correlation between serum and tissue expression levels of PAPP-A is lost in down’s pregnancies. These observation suggest that the decrease in maternal serum PAPP-A is posttranslational and may be caused by an alteration of the placenta releasing mechanisms or by a modification of the stability of the secreted protein [17]. PAPP-A found to be significantly higher in twin pregnancy on an average of 1.86 times greater than in singletons.
Moreover, a lower maternal PLGF was observed in women carrying a fetus with T21, 18 and 13. PLGF level were inversely related to NT thickness, a surrogate marker of Down syndrome [18]. NT is define as nuchal fluid accumulation visible on ultrasound. Increased expression of type IV collagen, leading to an accumulation of highly hydrophilic hyaluronan, has been considered in the pathogenesis of NT in trisomy 21 fetuses [19,20].
PLGF is expressed in endothelial cells, trophoblasts, monocytes and erythroid cells. Glial cell missing 1 (GCM1) is a transcription factor of PLGF in trophoblasts. Hypoxia triggers GCM1 degradation, which results in decreased expression of PLGF, the low level of angiogenic factor may contribute to endothelial dysfunction, one of the symptoms of preeclampsia [21]. Similarly maternal serum level of PLGF at 10 to 13 weeks of gestation are dcreased in pregnancies with fetal aneuploidy due to impaired placentation and delivery of small gestational age neonates [22].
In trisomy 21, 18 and 13 pregnancies there was a significant association between serum levels of PLGF and PAAP-A, which presumably reflects the postulated roles of these peptides in the placental development and/or their common origin from trophoblast. Addition of PLGF to free HCG and PAPP-A was associated with substantial improvement in the performance of first trimester biochemical screening.
References
- Copel JA, Bahado-Singh RO. Prenatal screening for Down’s syndrome—a search for the family’s values. N Engl J Med. 1999; 341(7): 521–522.
- Stembalska A, Ryszard OE, Karolina P, Justyna G, SasiadekMM. Prenatal diagnosis—principles of diagnostic procedures and genetic counseling. Folia Histochem Cytobiol. 2007; 45(Supp 1): 11–6.
- Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10–14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group. Lancet. 1998; 352: 343–346
- Souka AP, von Kaisenberg CS, Hyett JA, Sonek JD, Nicolaides KH. Increased nuchal translucency with normal karyotype. Am J Obstet Gynecol 2005; 192: 1005–1021.
- Dugoff L, Hobbins JC, Malone FD, et al. First-trimester maternal serum PAPP-A and free-beta subunit human chorionic gonadotropin concentrations and nuchal translucency are associated with obstetric complications: a population-based screening study (the FASTER Trial). Am J Obstet Gynecol. 2004; 191(4): 1446–1451.
- Smith GC, Shah I, Crossley JA, et al. Pregnancy-associated plasma protein A and alpha-fetoprotein and prediction of adverse perinatal outcome. Obstet Gynecol. 2006; 107(1): 161–166.
- Akolekar R, Syngelaki A, Sarquis R, ZvancaM, Nicolaides KH: Prediction of early, intermediate and late pre-eclampsia from maternal factors, biophysical and biochemical markers at 11–13 weeks. Prenat Diagn. 2011; 31: 66–74.
- Karagiannis G, Akolekar R, Sarquis R, Wright D, Nicolaides KH: Prediction of small-for-gestation neonates from biophysical and biochemical markers at 11–13 weeks. Fetal Diagn Ther. 2011; 29: 148–154.
- Maternal Serum Placental Growth Factor in Prospective Screening for Aneuploidies at 8–13 Weeks’ Gestation Pranav Pandya a David Wright b Argyro Syngelaki c Ranjit Akolekar dKypros H. Nicolaides a, c
- Handschuh K, Guibourdenche J, Guesnon M, LaurendeauI,Evain-Brion D, Fournier T. Modulation of PAPP-A expression by PPARgamma in human first trimester trophoblast. Placenta. 2006; 27(Suppl A): S127–34.
- Butler SA, Iles RK. The free monomeric beta subunit of humanchorionic gonadotrophin (hCG beta) and the recently identified homodimeric beta–beta subunit (hCG beta beta) both have autocrine growth effects. Tumour Biol. 2004; 25: 18–23.
- Pandya P, Wright D, Syngelaki A, Akolekar R, Nicolaides KH: Maternal serum placental growth factor in prospective screening for aneuploidies at 8–13 weeks’ gestation. Fetal Diagn Ther 2012; 31: 87–93.
- Overgaard MT, Sorensen ES, Stachowiak D, Boldt HB, Kristensen L, Sottrup-Jensen L, et al. Complex of pregnancy-associated plasma protein-A and the proform of eosinophil major basic protein disulfide structure and carbohydrate attachment sites. J Biol Chem. 2003; 278: 2106–17.
- Handschuh K, Guibourdenche J, Guesnon M, Laurendeau I, Evain-Brion D, Fournier T. Modulation of PAPP-A expression by PPARgamma in human first trimester trophoblast. Placenta. 2006; 27(Suppl A): S127–34.
- Peterson SE, Simhan HN. First-trimester pregnancy-associated plasma protein A and subsequent abnormalities of fetal growth. Am J Obstet Gynecol. 2008; 198(5): 43–5.
- Santolaya-Forgas I, Leon JAD, Cullen Hopkins R, Castracane VD, Kauffman RP, Sifuentes GP. Low pregnancy-associated plasma protein-A at 10 ? 1 to 14 ? 6 weeks of gestation and a possible mechanism leading to miscarriage. Fetal Diagn Ther. 2004; 19: 456–61.
- Brizot ML, Hyett JA, Mckie AT, Bersinger NA, Farzaneh F, Nicolaides KH. Gene expression of human pregnancy-associated plasma protein-A in placenta from trisomic pregnancies. Placenta. 1996; 17: 33–6.
- Llurba E, Syngelaki A, Sanchez O, Carreras E, Cabero L, Nicolaides KH: Maternal serum placental growth factor at 11–13 weeks’ gestation and fetal cardiac defects. Ultrasound Obstet Gynecol 2013; 42: 169–174.
- Brand-Saberi B, Floel H, Christ B, Schulte-Vallentin M, Schindler H: Alterations of the fetal extracellular matrix in the nuchal oedema of Down’s syndrome. Ann Anat 1994; 176: 539–547.
- von Kaisenberg CS, Brand-Saberi B, Christ B, Vallian S, Farzaneh F, Nicolaides KH: Collagen type VI gene expression in the skin of trisomy 21 fetuses. Obstet Gynecol 1998; 91: 319–323.
- Chiang, M.H., Liang, F.Y., Chen, C.P., Chang, C.W., Cheong, M.L., Wang, L.J., Liang, C.Y., Lin, F.Y., Chou, C.C., and Chen,H. (2009) Mechanism of hypoxia-induced GCM1 degradation: implications for the pathogenesis of preeclampsia. J.Biol. Chem. 284, 17411-17419.
- Karagiannis G, Akolekar R, Sarquis R, Wright D, Nicolaides KH. Prediction of small-for-gestation neonates from biophysical and biochemical markers at 11–13 weeks. Fetal Diagn Ther 2011; 29: 148–154.