
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Intraoperative electrocardiograph artifact mimicking
ventricular tachycardia during a spine surgery
Fei Wu; Shauna Williams; Jingping Wang*
Massachusetts General Hospital, Department of Anesthesia, Critical Care and Pain Medicine Boston, Massachusetts, USA.
*Corresponding Author : Jingping Wang
55 Fruit Street, GRB 444, Boston, MA 02114, USA.
Phone: 617-726-3030.
Email: JWANG23@mgh.harvard.edu
Received : Nov 04, 2022
Accepted : Nov 25, 2022
Published : Dec 02, 2022
Archived : www.jcimcr.org
Copyright : © Wang J (2022).
Abstract
Ventricular Tachycardia (VT) is a dangerous form of arrhythmia that often warrants immediate treatment. We report here a case of “intraoperative VT” as a result of Electrocardiograph (EKG) artifacts during a spine surgery. Differentiating EKG artifacts from real VT can be challenging for clinicians and we reviewed some practical strategies. Awareness to rule out artifacts is important to avoid unnecessary interventions, especially in the acute care setting of the operating room for anesthesia providers.
Keywords: Electrocardiogram (EKG); Artifact; Ventricular tachycardia; Unnecessary interventions; Intraoperative arrhythmia.
Citation: Wu F, Williams S, Wang J. Intraoperative electrocardiograph artifact mimicking ventricular tachycardia during a spine surgery. J Clin Images Med Case Rep. 2022; 3(12): 2182.
Introduction
Ventricular Tachycardia (VT) is a feared form of cardiac arrhythmia commonly associated with hemodynamic instability, global hypoperfusion and poor outcomes, often requiring immediate medical assessment and treatment. Diagnosis of ventricular tachycardia relies on the EKG, which is characterized as a regular, wide complex tachycardia. However other heart rhythms [1], as well as some artifacts [2-4] can mimick this EKG morphology, sometimes leading to unnecessary medical interventions [5].
Here we report a case where new onset of “wide complex tachycardia” was noted intraoperatively but was ultimately found to be artifact. We will review common EKG artifacts that can mimic VT and suggest an algorithm for differentiating artifact from real VT.
Case presentation
A 66-year-old female with chronic neck pain, type 2 diabetes mellitus, sleep apnea, obesity presented for C3-C6 laminoplasty She had no issues with her prior anesthetics. Her preoperative lab tests, including a complete blood count, basic metabolic panel, coagulation panel were unremarkable. A preoperative EKG shows normal sinus rhythm, with minor nonspecific ST-T change (Figure 1A).
She had family history of sudden deaths of unknown reason at young ages (all< 50, one< 35) in second-degree maternal relatives. On day of surgery, preoperative evaluations, including physical examination and telemetry tracing at the preop bay showed no abnormalities. ASA standard monitor including a 5-lead EKG was applied before general anesthesia was induced with 150 mg of propofol, 70 mg of rocuronium and 100 mcg of fentanyl, and endotracheal intubation was completed uneventfully. Anesthesia was maintained with sevoflurane at 0.9 MAC. Phenylephrine drip was started at rate of 20-50 mcg/min to maintain a mean arterial pressure of 75 mmHg.
Patient was positioned prone with head placed in the Mayfield pins. About 70 min after incision, abnormal EKG tracing was noted on the monitor, at that time displaying lead II and V1. It was noted to be a wide complex tachycardia with a rate of around 200 beats per minute, full tracing of which was later obtained from the control desk (Figure 1C and D). Patient was hemodynamically stable and maintained good oxygen saturation during this episode. This rhythm lasted for about 30 seconds before it reverted to baseline normal sinus rhythm with a rate of 60. Patient tolerated the remainder of the procedure with no issues and was brought back to PACU for recovery. Blood work such as CBC, BMP, magnesium and phosphorous were obtained, and all within normal limits. A formal 12 lead EKG was obtained which showed normal sinus rhythm with nonspecific ST change, no significant change from prior (Figure 1B). A Cardiology consult was called for “intraoperative ventricular tachycardia”, and after evaluation deemed the intraoperative tracing as artifact with normal underlying sinus rhythm. The patient had an uneventful recovery and was discharged home on postoperative day 2.
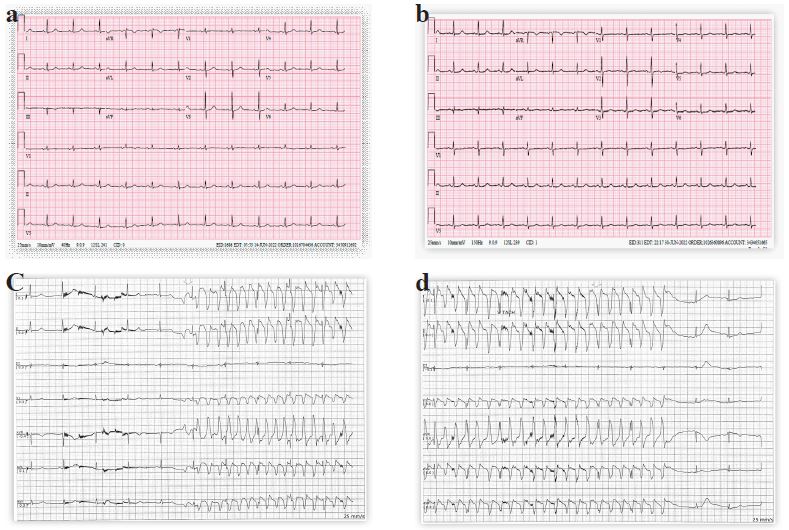
Figure b: Postoperative 12-lead EKG
Figure c: Intraoperative 5-lead EKG
Figure d: Intraoperative 5-lead EKG (cont’)
Discussion
Surface EKG tracing picks up cardiac electrical activity from cutaneous electrodes and is filtered and amplified before displaying [6], a process prone to many internal (physiological) and external (non-physiological) sources of artifacts [7].
There had been a handful of case reports about different sources of EKG artifacts mimicking VT, most commonly tremor [2,8,9], sometimes resulting in surgery cancellation and unnecessary interventions [5]. Differentiation of VT from artifact can sometimes be difficult, even for cardiologists and electrophysiologists [10]. Huang et al. suggested an algorithm to differentiate tremor artifacts from real VT [11], focusing on identifying the underlying normal sinus rhythm in the strips. In our case, EKG tracing in lead III was not influenced by artifact and maintained normal sinus rhythm. There are “VT complexes” in all other available leads at a rate around 200 Hz. However on closer inspection, small, but regular spikes that coincide with the QRS complexes on Lead III temporally are seen in the leads with “VT”, representing the “hidden QRS complexes” among the artifact. Lead III seems to be most resistant to the artifacts, as shown in our case and many of above-mentioned reports. This may be due to lead III picking up the electrical vector perpendicular to the main cardioelectrical axis, making it inherently less susceptible to artifacts that are obvious in the left/anterior-directing leads, which do make up the majority of the EKG paper and tend to catch the reader’s eye at first glance. Therefore, it is important to view all available leads tracings to differentiate artifact from true arrhythmia. Also, concurrent hemodynamic stability demonstrated by a stable blood pressure, a normal pulse oximetry wave form and stable pulse rate would be other indication of EKG artifact, as seen in our case.
Our artifact was less likely from tremor as patient was paralyzed during this procedure. There are many known sources of EKG interferences in the operating room [6], and new electrical equipment introduced into the OR brings a constant flow of new suspects. In particular, Gaiser et al reported microdebrider used in endoscopic sinus surgery causing EKG artifacts mimicking VT due to stray electrical current [3]. We did use an ultrasonic bone shaver in our case, but the artifact did not correlate with the use of the shaver and was not reproducible. We did not identify the direct source of the artifact in our case.
Intraoperative VT is just as dangerous physiologically as in other settings yet is of particular diagnostic challenge as patients under anesthesia are unable to report symptoms of palpitation, chest pain, or show signs of syncope, altered mental status. That being said, while attention to the EKG tracing change is important, anesthesia provider should focus more on the hemodynamic stability. Abnormal EKG tracing not associated with hemodynamic compromise usually does not warrant immediate action, and careful differentiation of artifact versus true arrhythmia is feasible and important for avoiding unnecessary interventions.
Conclusion
Current surface EKG tracing is susceptible to various sources of artifacts, particularly in the operating room. Artifacts mimicking VT can be differentiated from real VT by evaluating tracings from all available EKG leads and looking for hidden normal QRS, as well as unchanged hemodynamics. Artifacts should be ruled out before actual treatment towards intraoperative arrhythmia is carried out, especially if the patient is hemodynamically stable.
References
- Ding WY, Mahida S. Wide complex tachycardia: Differentiating ventricular tachycardia from supraventricular tachycardia. Heart. 2021; 107: 1995-2003.
- Ortega Carnicer J. Tremor-related artefact mimicking ventricular tachycardia. Resuscitation. 2005; 65: 243-244.
- Gaiser RR, Demetry DJ, Schlosser R. Ventricular tachycardia as an electrocardiography artifact during functional endoscopic sinus surgery. Am J Rhinol. 2003; 17: 83-85.
- Duan X. Electrocardiographic artifact due to a mobile phone mimicking ventricular tachycardia. J Electrocardiol. 2014; 47: 333-334.
- Bhatia L, Turner DR. Parkinson’s tremor mimicking ventricular tachycardia. Age Ageing. 2005; 34: 410-411.
- Patel SI, Souter MJ. Equipment-related electrocardiographic artifacts: Causes, characteristics, consequences, and correction. Anesthesiology. 2008; 108: 138-148.
- Littmann L. Electrocardiographic artifact. J Electrocardiol. 2021; 64: 23-29.
- Llinas R, Henderson GV. Images in clinical medicine. Tremor as a cause of pseudo-ventricular tachycardia. N Engl J Med. 1999; 341: 1275.
- Martens P, Sinnaeve P. Tremor mimicking ventricular tachycardia. CMAJ. 2015; 187: E326.
- Knight BP, Pelosi F, Michaud GF, Strickberger SA, Morady F, et al. Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia. Am J Med. 2001; 110: 335-338.
- Huang CY, Shan DE, Lai CH, Fong MC, Huang PS, et al. An accurate electrocardiographic algorithm for differentiation of tremor-induced pseudo-ventricular tachycardia and true ventricular tachycardia. Int J Cardiol. 2006; 111: 163-165.