
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Oligometastatic papillary urothelial carcinoma with FGFR2 and FGFR3 mutations: Case series of four patients and review of the literature
Hesham Yasin, MD*; Nancy Davis, MD; Jennifer Gordetsky, MD; Sally York, MD; Yu-Wei Chen, MD; Kerry Schaffer, MD
Vanderbilt University Medical Center, Nashville, Tennessee, USA.
*Corresponding Author : Hesham Yasin
Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Email: hishamyassin@gmail.com
Received : Oct 08, 2022
Accepted : Nov 25, 2022
Published : Dec 02, 2022
Archived : www.jcimcr.org
Copyright : © Yasin H (2022).
Abstract
Background: Urothelial carcinoma of the bladder is common cancer. Despite advances in treatments and the introduction of immune checkpoint inhibitors in recent years, metastatic disease carries a poor prognosis. Fibroblast growth factor receptors (FGFR) family alterations are frequently implicated in the development of papillary urothelial carcinomas. FDA-approved FGFR inhibitors demonstrate good response in patients with locally advanced and metastatic urothelial carcinomas that harbor FGFR mutations.
Case presentation: We present a case series of four patients with FGFR alterations and oligometastatic disease, all of whom developed metastasis in the setting of non-muscle invasive primary bladder tumors. The patients demonstrated impressive responses to local and systemic therapies during their course achieved prolonged survival.
Citation: Yasin H, Davis N, Gordetsky J, York S, Chen YW, et al. Oligometastatic papillary urothelial carcinoma with FGFR2 and FGFR3 mutations: Case series of four patients and review of the literature. J Clin Images Med Case Rep. 2022; 3(12): 2183.
Background
Bladder cancer is the 6th most common cancer in the United States. Despite advances in treatment options, metastatic disease carries a poor prognosis with an estimated 5-year survival of 5% [1,2]. Ninety percent of bladder cancers are of urothelial type (UC) [3]. Around 70% of diagnosed bladder cancers are non-muscle-invasive bladder cancers (NMIBC), while the remaining are muscle-invasive bladder cancers (MIBC). NMIBC has a sixty percent recurrence rate, with 10% percent of cases progressing to muscle-invasive tumors [4]. Cytotoxic chemotherapy has been the standard of care for the treatment of metastatic disease, despite good objective responses (ORR), these responses are not durable, not to forget the significant toxicities associated with chemotherapy [5]. In the recent decade immune checkpoint inhibitors have been introduced. Though well tolerated, ORR is low (20%), and median overall survival is less than a year [6]. This necessitates exploring different approaches such as targeting specific mutations that are implicated in the development of disease. UC is characterized by a wide range of genomic and molecular alterations [7-9]. Fibroblast growth facfactor receptors (FGFR) are a family of receptor tyrosine expressed on the cell membrane; they play key roles in cellular pathways such as stimulating cell growth, differentiation, survival, angiogenesis, and organogenesis. FGFR mutations are associated with the development of several human cancers such as leukemia, breast cancer, and bladder cancer [11]. FGFR 1-4 mutations are quite common in bladder cancer with FGFR3 mutations being the most frequent [12]. Billery et al. identified FGFR3 alterations in 48 out of 132 sampled bladder tumors, interestingly mutations were more frequent in low-grade tumors compared to high-grade ones: 27 out of 32 (84%) Grade 1 tumors, 16 of 29 (55%) G2, and 5 of 71 (7%) G3 tumors [13].
Recently, there has been significant interest in precision therapies due to increased knowledge of the role of genomic alterations in the pathogenesis of bladder cancer. In the BLC2001 trial, Erdafitinib, a pan-FGFR inhibitor, induced a 42% overall response rate in patients with metastatic or surgically unresectable UC with a verified mutation in FGFR3 or fusion in FGFR2 or FGFR311. Interestingly, more than two-thirds of patients who previously had been treated with ICIs in that clinical trial(Immune Checkpoint Inhibitors) had an objective response to erdafitinib [14]. While data regarding therapeutic responses to FGFR therapies is available, data on the initial presentation for UC with FGFR alterations are not well established, and the response rates to other classes of therapies are not yet well characterized. Given the increasing numbers of FDA-approved therapies for advanced UC, understanding the responses to various classes of therapies is of high interest. We present 4 cases of patients with oligometastatic disease and FGFR alterations in the setting of new or previously diagnosed non-muscle-invasive bladder cancer; here we review their course as well as their genomic alterations.
Case presentations
Case 1
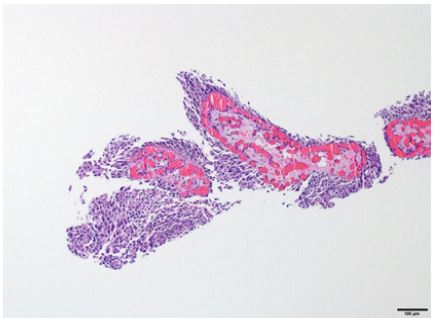
A 62-year-old male patient with a 35-pack year smoking history presented to the urology clinic for evaluation of gross hematuria. On the first cystoscopy, multiple papillary tumors were found, transurethral resection of the bladder tumor (TURBT) was done, and biopsy demonstrated high-grade papillary urothelial carcinoma, suspicious for invasion into the lamina propria, muscularis propria (MP) was present and not involved by the tumor. Repeat cystoscopy and TURBT one month later demonstrated the same previous pathological findings, MP was also present. The patient was then referred to a urology clinic at a tertiary cancer center. A third TURBT, two months after the second one, showed again NMIBC, MP was present. Computed tomography (CT) of chest, abdomen, and pelvis with urogram was obtained to rule out metastatic disease, which only remarkable for multiple filling defects in the bladder consistent with tumor infiltration. The patient then underwent BCG induction followed by a maintenance course. A repeat TURBT after BCG treatment demonstrated again recurrent NMIBC (Figure 1), and no lymphovascular invasion was identified in the specimens. At that time, he underwent CT of the chest, abdomen, and pelvis for evaluation of his recurrent disease which showed thickening of the bladder wall and a isolated irregular lobular lesion within the left lower lobe of the lung measuring 2.5 cm in diameter. A biopsy of the nodule showed metastatic carcinoma, Immunohistochemical stains were positive for GATA3 and negative for TTF1, findings consistent with urothelial origin. The patient was referred to medical oncology for treatment and received 4 cycles of Carboplatin and Gemcitabine systemic chemotherapy (Cisplatin was not used due to impaired kidney function). The patient was hesitant to receive avelumab maintenance. A follow-up CT scan post-chemotherapy showed disease response with a slight shrinkage of the known lung nodule (2.5 cm to 2.1 cm in diameter) and no new metastatic lesions were identified. A follow-up CT scan 1 month later showed enlargement of the known metastatic lung lesion to 4 cm with no additional metastatic lesions identified. He received 4 doses of Pembrolizumab, but a follow-up CT scan showed substantial growth of the metastatic lesion, therefore the treatment was discontinued. A genomic sequencing profile was obtained which showed a mutation in FGFR3 in the tumor sample (Table 1). Given the presence of the FGFR3 mutation, the decision was to start the patient on Erdafitinib, and he also underwent irradiation to the pulmonary nodule. His treatment course was remarkable for a brief interruption of erdafitinib for dry eyes and skin peeling. Surveillance images while on treatment showed a continued rereduction of the known pulmonary lesion to 1.5 cm, which means shrinkage of 63% of tumor mass (Figure 5). After one year of erdafitinib, the treatment was stopped due to grade III toxicities including skin rashes, oral sores, and profound fatigue. A CT scan was done one month after discontinuation and showed an increase in the size of the known lung nodule in addition to a new smaller nodule. The patient then received 5 cycles of carboplatin and gemcitabine, however, had to discontinue therapy due to cytopenia and recurrent urinary tract infections (UTI). Repeat imaging after 1.5 months showed an increased size of the known pulmonary nodules and no other metastasis. Enfortumab vedotin was recommended, however, the patient unfortunately had hospitalization 3 months after discontinuing Carboplatin and Gemcitabine due to pain and failure to thrive. He was then diagnosed with significant disease progression including multifocal brain metastases, and he transitioned to hospice.
Case 2
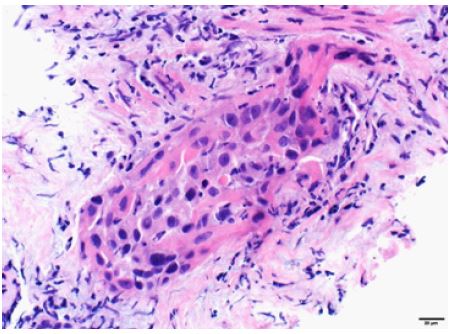
A 58-year-old male patient with a previous 20-pack-year smoking history presented with pelvic pain, difficulty urinating, and intermittent gross hematuria. He underwent CT scan with contrast of the abdomen and pelvis, which showed enhancing 4.6 cm lobulated mass involving the urinary bladder. In addition, a 3.2 cm lytic lesion was identified involving the left pubic bone. The patient underwent a cystoscopy and TURBT. Pathology showed invasive high-grade papillary urothelial carcinoma into the lamina propria (Figure 2). Muscularis propria was present and uninvolved. A biopsy from the pelvic lesion was performed, which showed metastatic urothelial carcinoma. CT scan of the chest was negative for metastatic disease. Genomic sequencing of the tumor sample came back positive for FGFR3 and TACC gene fusions (Table 1). The patient underwent 4 cycles of cisplatin and gemcitabine. A follow-up CT scan after chemotherapy showed stable disease. Repeat cystoscopy and TURBT showed invasive high-grade urothelial carcinoma into the lamina propria, again with no muscularis propria invasion. 5 months after completing chemotherapy, CT scans again confirmed no distant metastatic disease, and the patient underwent radical cystectomy. Pathology showed focal residual noninvasive high-grade papillary urothelial carcinoma pTaN0. Ablative local radiation to the pelvic bone lesion was performed with dose of 40 Gy over 5 fractions and later the patient started Avelumab maintenance therapy. As of 10 months post radical cystectomy there has been no progression on surveillance imaging.
Case 3
A 71-year-old male patient, a previous smoker, presented for evaluation of gross hematuria. He underwent cystoscopy, which identified a 2 cm posterior bladder wall tumor. Histologic examination showed a low-grade noninvasive papillary urothelial carcinoma with focal high-grade areas. The patient underwent 6 cycles of intravesical mitomycin bladder instillation. Repeat cystoscopy and TURBT showed a recurrent 2 cm noninvasive low-grade papillary urothelial carcinoma, no muscle invasion was present. 2 years later the patient presented to urology clinic with complaints of nocturia, urinary urgency, and frequency. Repeat cystoscopy showed a lesion in the prostatic urethra, which was biopsied and pathological exam demonstrated noninvasive low-grade papillary urothelial carcinoma, MP present (Figure 3). Repeat cystoscopy two months later was normal. Atthe same time, the patient underwent a CT scan of the chest which showed a 4.2 cm lobulated mass and a 1.7 cm (about 0.67 in) spiculated lesion in the left lobe of the lung (Figure 6). Biopsies from the lesions showed two distinct malignancies; Immunohistochemical stains identified the left upper lobe lesion as a primary non-small cell adenocarcinoma while the left lower lobe lesion was metastatic urothelial carcinoma (positive for GATA3 and p40 and negative for TTF-1). Wedge resection was done for both lesions. Genomic sequencing of the metastatic urothelial tumor showed an FGFR3 mutation (Table 1). After a discussion of various options, including the potential for adjuvant platinum-based chemotherapy, the patient opted for surveillance. Surveillance imaging at four months demonstrated several liver nodules, mediastinal lymphadenopathy, and osseous metastases in the lumbar spine. Biopsy of a liver lesion showed metastatic carcinoma, consistent with urothelial primary. The patient received 3 cycles of cisplatin and gemcitabine (discontinued due to poor tolerance), as well as radiation to the spinal lesion for symptom relief. Follow-up imaging after treatment showed good disease response with mild shrinkage of all lesions and the patient decided to stop treatment after 6 doses of maintenance Avelumab. A recent cystoscopy was performed and showed no evidence of disease recurrence in the bladder.
Table 1: Characteristics of FGFR mutations, other somatic mutations, immune markers.
| Mutated gene | Protein change | Mutation type | VAF | Other significant mutations | TMP (mMB) and percentile | MSI | |
|---|---|---|---|---|---|---|---|
| Case 1 □ | FGFR3 | S249C | Missense Variant-GOF | 74.5% | KDMGA, PIK3CA, CDKN2A, MTAP | 5.8 (76) | Stable |
| Case 2 □ | FGFR3 | N/A | FGR3 -TACC3 genes Chromosomal rearrangement | - | TERT, ELF3 CDKN2A CDKN28, FAT1, RUNX1 | 7.9 (82) | Stable |
| Case 3ⴕ | FGFR3 | S249C | Missense Variant -GOF | 49.5% | RBM10, ARID1A, TERT CDKN2A, CDKN2B, MTAP, PAK1, RSF1 | 5.3 (67) | Stable |
| Case 4Δ | FGFR2 | N/A | FGFR2-BICC1 genes chromosomal rearrangement | N/A | BAP1, TP53 | N/A | Not assessed |
*VAF: Variant allele fraction. TMP: Tumor mutational burden MSI: Microsatellite instability. GOF: Gain of function
□: Genomic testing was performed on bladder specimen
ⴕ: Genomic testing was performed on metastatic tissue specimen
Δ: Genomic testing was performed on Blood sample only


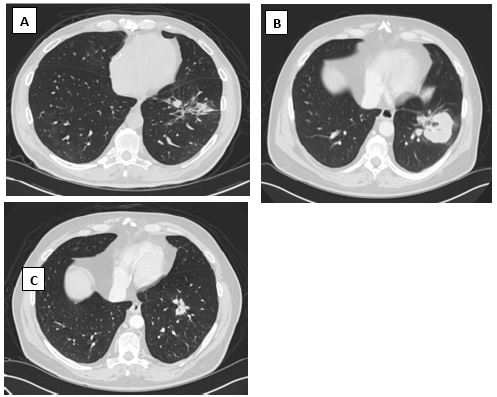
(B): the lesion after progression while on pembrolizumab,
(C): lesion shrinkage after Erdafitinib.

Case 4
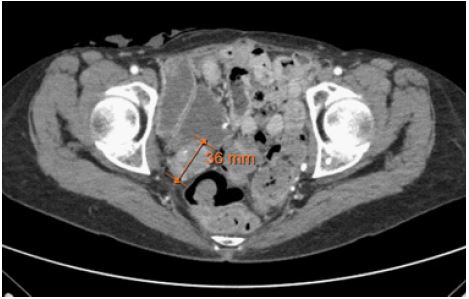
A 62-year-old former smoker female patient underwent radical cystectomy with ileal conduit urinary diversion for BCG-refractory high-grade pTaN0 papillary urothelial carcinoma with negative margins. 6 years later she presented with progressive pelvic pain and underwent CT imaging which identified a 2.4 cm right-sided pelvic mass, concerning for oligometastatic disease (Figure 7). Biopsy of the mass showed carcinoma with squamous differentiation, with immunohistochemical stains negative for p16 therefore suggestive of urothelial origin (Figure 4). The patient then received 3 cycles of Carboplatin and Docetaxel. Follow-up imaging showed no change in the size of the tumor, however, the patient had significant relief of pain. Shortly thereafter, the patient underwent local palliative radiation to the pelvic lesion (600 Gy in 15 fractions), followed by surveillance. Follow-up imaging at 18 months showed an increase in the size of the pelvic mass with involvement of the piriformis muscle and no other sites of metastatic disease. Erdafitinib was selected for treatment due to the presence of an FGFR2 mutation that was detected on genomic sequencing testing of tumor tissue biopsied from the metastatic site. Two months into erdafitinib the patient underwent imaging for abdominal pain which demonstrated a slight reduction in the pelvic wall mass and no other areas of metastasis. At the time of chart review, 3 months on erdafitnib, the patient has been tolerating the treatment well.

Discussion
To our knowledge, our series is the first outlining clinical courses for FGFR alterations in oligometastatic UC, and there are a number of interesting patterns worth highlighting. All of the patients presented here had no muscle invasion in their bladder specimens examined; two were radical cystectomy specimens and the other two were TURBT samples. Another interesting feature is that patients have good outcomes and prolonged survival, including progression only in the original known metastatic sites.
It is worth exploring whether there is a pattern for FGFR mutated tumors to exhibit growth patterns within the bladder (perhaps within diverticula) which may not easily be detected on typical TURBT and therefore missing the diagnosis of muscle invasion [15]. Metastatic non-muscle invasive bladder cancer is rare, with one study reporting a prevalence of 0.9% among 1000 tumor samples [16]. In another study, 10% of patients with NMIBC who underwent radical cystectomy were found to have regional lymph node metastasis (9% for T1, 12% for Tis, 4.5% for Ta) [17].
In 2019 Erdafitinib was approved for locally advanced and metastatic urothelial carcinoma, with susceptible FGFR3 or FGFR2 genetic alterations that have progressed during or following platinum-based chemotherapy, including within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy [18]. In the phase III clinical trial conducted by Loroit et al. erdafitinib achieved a 40% objective response rate (ORR) with a 3% complete response; however, among the patients who had prior immunotherapy, the (ORR) was 59%. The median duration of progression-free survival was 5.5 months, and the median overall survival was 13.8 months [14]. There are many ongoing trials evaluating the efficacy and safety of other FGFR inhibitors in different clinical such as Infigratinib, Pemigartinib, and Rogaratinib [19-21]. Genomic testing on tumor tissue is now readily available and can help identify precision therapies that may provide disease control and improved survival for patients across many cancer types including bladder cancer [22,23]. Numerous publications have demonstrated the underutilization of genomic testing in UC24-26 despite several studies noting that FGFR3 mutations have an estimated prevalence of 40% of UC cases [27]. These 4 cases provide compelling evidence, as do the trials leading to approval of erdaftinib, that precision treatments for UC can be extremely effective in a large proportion of patients.
As previously mentioned, all patients in this cohort had relatively slow progression and relatively good survival compared to reported outcomes for metastatic disease in clinical trials. Previous reports indicated that FGFR3-mutated UC tend to have better prognosis and are less likely to have muscle invasion, but it is unclear whether this is the case for advanced disease [29,5]. All patients are all alive after a median of 15 months since diagnosis of metastasis compared to median OS in published therapeutic were ranging from 7.3 to 13.8 months [6,14,28].
There is no clear trend we can appreciate in this cohort about the response to IO therapy given only one patient received it. Literature does not provide enough data regarding ICI response in patients with FGFR3 mutated tumors [5]. As only 1 patient in this cohort received IO therapy, we cannot speculate on any trend. Preclinical studies demonstrated that FGFR activity correlated negatively with lymphocyte infiltration and also with response to PDL-1 inhibitors [30,31]. In regard to FGFR inhibition following ICI, the erdafitinib pivotal trial showed that patients who received prior ICI had more objective response (59% vs 40%) [11]. A possible explanation for this finding is the ICI could alter the tumor microenvironment and therefore “sensitize” it for FGFR inhibition, another explanation is tumors exposed to immunotherapies develop enhanced FGFR expression as a mechanism for resistance to immunotherapy [5].
The patients here parallel the data from the clinical trials performed with erdafitinib. The trial breakdown shows improved PFS in patients with smaller disease volumes, compared to those with larger disease volumes. In one patient who received Erdafitinib, the PFS was 12 months and ongoing in a second, significantly higher than the median PSF of 5.5 in similar patients in the previously mentioned trial [11].
Though this cohort is small, it opens a lot of questions regarding the optimal management of patients with oligometastatic disease, whether it is better treated with systemic therapy or local therapy (radiation and surgery) or combination treatment. It also emphasizes utilization of genetic testing that can tailor best precision treatment and predict prognosis. It will open ideas to better understand the biology of FGFR- mutated tumors and understand the pathophysiology that may make these tumors slow growing and less aggressive. More studies are needed to investigate the role of immunotherapies in tumors expressing FGFR mutation and investigate the sequence of treatment with ICI and FGFR inhibitors. A more extensive study on similar will support our hypotheses and can help establish a guideline for treating similar patients in the future.
References
- Saginala, K., Barsouk, A., Aluru, J. S., Rawla, P., Padala, S. A., & Barsouk, A. (2020). Epidemiology of bladder cancer. Medical sciences, 8(1), 15.
- Siegel, R. L., Miller, K. D., & Jemal, A. (2020). Cancer statistics, 2020. CA: a cancer journal for clinicians, 70(1), 7–30. https://doi.org/10.3322/caac.21590
- Chalasani V, Chin JL, Izawa JI. Histologic variants of urothelial bladder cancer and nonurothelial histology in bladder cancer. Can Urol Assoc J. 2009;3(6 Suppl 4): S193-S198. doi:10.5489/cuaj.1195
- Duenas, Marta, et al. “PIK3CA gene alterations in bladder cancer are frequent and associate with reduced recurrence in non‐muscle invasive tumors.” Molecular carcinogenesis 54.7 (2015): 566-576.
- Kacew, Alec, and Randy F. Sweis. “FGFR3 alterations in the era of immunotherapy for urothelial bladder cancer.” Frontiers in Immunology 11 (2020): 575258.
- Bellmunt, Joaquim, et al. “Pembrolizumab as second-line therapy for advanced urothelial carcinoma.” New England Journal of Medicine 376.11 (2017): 1015-1026..
- Matthews, P. N., Madden, M., Bidgood, K. A., & Fisher, C. (1984). The clinicopathological features of metastatic superficial papillary bladder cancer. The Journal of urology, 132(5), 904–906. https://doi.org/10.1016/s0022-5347(17)49939-3
- Mhawech‐Fauceglia, Paulette, Richard T. Cheney, and Juerg Schwaller. “Genetic alterations in urothelial bladder carcinoma: an updated review.” Cancer: Interdisciplinary International Journal of the American Cancer Society 106.6 (2006): 1205-1216.
- Choi, Woonyoung, et al. “Genetic alterations in the molecular subtypes of bladder cancer: illustration in the cancer genome atlas dataset.” European urology 72.3 (2017): 354-365.
- Weinstein, JN, Akbani, R, Broom, BM, et al. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014; 507: 315–322.
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322.
- Casadei, Chiara, et al. “Targeted therapies for advanced bladder cancer: new strategies with FGFR inhibitors.” Therapeutic advances in medical oncology 11 (2019): 1758835919890285.
- Billerey, Claude, et al. “Frequent FGFR3 mutations in papillary non-invasive bladder (pTa) tumors.” The American journal of pathology 158.6 (2001): 1955-1959.
- Loriot, Yohann, et al. “Erdafitinib in locally advanced or metastatic urothelial carcinoma.” New England Journal of Medicine 381.4 (2019): 338-348.
- Kim, Lawrence HC, and Manish I. Patel. “Transurethral resection of bladder tumor (TURBT).” Translational Andrology and Urology 9.6 (2020): 3056.
- Teyssonneau D, Daste A, Dousset V, Hoepffner JL, Ravaud A, Gross-Goupil M. Metastatic non-muscle invasive bladder cancer with meningeal carcinomatosis: case report of an unexpected response. BMC Cancer. 2017;17(1):323. Published 2017 May 11. doi:10.1186/s12885-017-3309-2
- Bruins HM, Skinner EC, Dorin RP, et al. Incidence and location of lymph node metastases in patients undergoing radical cystectomy for clinical non-muscle invasive bladder cancer: results from a prospective lymph node mapping study. Urol Oncol. 2014; 32(1): 24.e13-24.e2.4E19.
- Markham, Anthony. “Erdafitinib: first global approval.” Drugs 79.9 (2019): 1017-1021.
- Pal, Sumanta K., et al. “PROOF 302: A randomized, double-blind, placebo-controlled, phase III trial of infigratinib as adjuvant therapy in patients with invasive urothelial carcinoma harboring FGFR3 alterations.” J. Clin. Oncol 38 (2020).
- Rosenberg, Jonathan E., et al. Safety and preliminary efficacy of rogaratinib in combination with atezolizumab in a phase Ib/II study (FORT-2) of first-line treatment in cisplatin-ineligible patients (pts) with locally advanced or metastatic urothelial cancer (UC) and FGFR mRNA overexpression. (2020): 5014-5014.
- Galsky, Matt D., et al. FIGHT-205: Phase II study of first-line pemigatinib (PEMI) plus pembrolizumab (PEMBRO) versus PEMI alone versus standard of care (SOC) for cisplatin (CIS)—Ineligible urothelial carcinoma (UC) with FGFR3 mutation or rearrangement. (2020): TPS592-TPS592.
- Nadal, Rosa, and Joaquim Bellmunt. Management of metastatic bladder cancer. Cancer treatment reviews 76 (2019): 10-21.
- Presley, Carolyn J., et al. Association of broad-based genomic sequencing with survival among patients with advanced non–small cell lung cancer in the community oncology setting. Jama 320.5 (2018): 469-477.
- Kaminski, Allysen, Jyoti Aggarwal, and Gboyega Adeboyeje. HSR20-090: Current Utilization of Genomic Testing and Barriers to Optimal Patient Care: A Targeted Literature Review. Journal of the National Comprehensive Cancer Network. 18.3.5 (2020): HSR20-090.
- Wheler JJ, Janku F, Naing A, et al. Cancer Therapy Directed by Comprehensive Genomic Profiling: A Single Center Study. Cancer Res. 2016; 76(13): 3690-3701. doi:10.1158/0008-5472. CAN-15-3043
- Balogun, Onyinye D, and Olufunmilayo I. Olopade. Addressing health disparities in cancer with genomics. Nature Reviews Genetics 22.10 (2021): 621-622.
- Tomlinson DC, et al. FGFR3 protein expression and its relationship to mutation status and prognostic variables in bladder cancer. The Journal of pathology 213.1 (2007): 91-98.
- Powles, Thomas, et al. Enfortumab vedotin in previously treated advanced urothelial carcinoma. New England Journal of Medicine 384.12 (2021): 1125-1135.
- Van Rhijn, Bas WG, et al. The FGFR3 mutation is related to favorable pT1 bladder cancer. The Journal of urology 187.1 (2012): 310-314.
- Sweis RF, Spranger S, Bao R, et al. Molecular Drivers of the Non-T-cell-Inflamed Tumor Microenvironment in Urothelial Bladder Cancer. Cancer Immunol Res. 2016;4(7):563-568. doi:10.1158/2326-6066.CIR-15-0274
- Palakurthi, Sangeetha, et al. “The Combined Effect of FGFR Inhibition and PD-1 Blockade Promotes Tumor-Intrinsic Induction of Antitumor ImmunityErdafitinib plus Anti–PD-1 Enhances Antitumor Responses.” Cancer immunology research 7.9 (2019): 1457-1471.