
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Replacement of the descending aorta for
mediastinal sarcoma: An unusual approach
Jérémy Tricard1*; Simon Rouzé2; Erwan Flecher2; Bertrand De Latour2
1Department of Cardiac and Thoracic Surgery, Limoges University Hospital Center, France.
2Department of Thoracic, Cardiac and Vascular Surgery, Rennes University Hospital Center, France.
*Corresponding Author : Térémy Tricard
Department of Cardiac and Thoracic Surgery, Limoges University Hospital Center, 2 Avenue Martin Luther King, 87042 Limoges Cedex, France.
Fax: +33 5 55 05 63 84;
Email: jeremy.tricard@etu.unilim.fr
Received : Nov 03, 2022
Accepted : Nov 28, 2022
Published : Dec 05, 2022
Archived : www.jcimcr.org
Copyright : © Tricard J (2022).
Abstract
We report the case of posterior mediastinal myxoid liposarcoma with right intra-pleural development operated through right thoracotomy. We observed a significant invasion of a segment of the descending aorta though there was no evidence of tumor infiltration in preoperative imaging. A replacement of the descending thoracic aorta was peroperatively decided in order to perform a complete resection. Postoperative course was uneventful with a satisfactory good survival of 4 years despite a histological subtype associated with a poor prognosis. Right posterolateral thoracotomy is an unusual approach for descending aorta replacement but can be considered for malignant tumor resection.
Keywords: Mediastinal neoplasms; Sarcoma; Aorta; Thoracic.
Citation: Tricard J, Rouzé S, Flecher E, Latour BD. Replacement of the descending aorta for mediastinal sarcoma: An unusual approach. J Clin Images Med Case Rep. 2022; 3(12): 2185.
Introduction
Liposarcomas of the mediastinum are scarce and represent less than 1% of all mediastinal tumors [1]. The only treatment to improve survival remains radical surgical resection [2]. Here in we report the rare case of posterior mediastinal liposarcoma with right intra-pleural development operated through right thoracotomy. In order to perform a monobloc resection, a replacement of a segment of descending thoracic aorta through this unusual approach was realized.
Case presentation
A 50 year old woman presented with a posterior mediastinal mass discovered on a CT-scan performed for nonspecific epigastric pain. Her previous medical history reported the excision of a myxoidliposarcoma of the left leg (T2 N0 M0, radical resection) three years ago, with adjuvant chemotherapy (4 cycles of adriamycin and ifosfamide) and radiotherapy (60 gray). The mediastinal mass was well-defined, measuring 20 cm by 10 cm. There was no evidence of invasion of the adjacent structures in magnetic resonance imaging and CT-scan (Figure 1A).

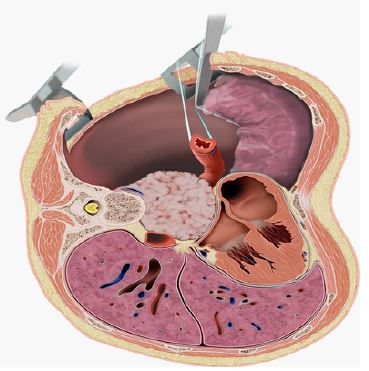
Surgery was performed with adesilet catheter introducer preventively placed in the left femoral vein in case temporary mechanical support would be necessary. A right posterolateral thoracotomy was performed in the 8th intercostal space. The mass was adherent to the spine. The azygous vein was ligated and the esophagus was dissected and pushed upward. Diaphragmatic pillars were cut. The spine was progressively released with extra-musculo-periosteal dissection on the 7th, 8th and 9th vertebrae. Titanium clips were placed at this level (Figure 1B). After opening the contralateral pleura, we observed significant adhesions of the tumor to the descending thoracic aorta (Figures 2 and 3). The en-bloc resection of the invaded descending aorta segment was decided intraoperatively. After heparinization, a replacement of the descending thoracic aorta with a 16 mm-Dacron prosthesis was performed using running sutures of 5/0 polypropylene. Aortic clamping time was 39 minutes.

The postoperative course was uneventful with extubationat day-1, an intensive care unit length of stay of 4 days and the patient was discharged 8 days after surgery. Histological analysis revealed a myxoid liposarcoma recurrence with the same phenotype as the first anatomical location. In addition, R1 resection at the cortex of the 8th vertebral level was noted and adjuvant radiotherapy (50 Gy) was performed. The patient lived at home with a good quality of life and without rehospitalization, until a retro-peritoneal recurrence of her liposarcoma caused her death four years after this thoracic resection.
Discussion
Only a few cases of liposarcoma of the mediastinum have been previously reported in the literature [3]. Indeed, liposarcomas are located in the retroperitoneum and limbs in 90% of cases [2,4]. Radical excision and histological type of tumor have been identified as independent prognostic factors of mortality with well-differentiated liposarcoma having a better prognosis than other histological subtypes (myxoid, round cell, pleomorphic and dedifferentiated) [5]. Radiotherapy and chemotherapy are usually used in association and are believed to be ineffective therapeutic modalities for survival [4].
Chen et al. showed in their series of 23 cases an overall survival of 13 months in cases of non-radical resection [2]. Moreover, invasion of the great vessels often necessitates a non-radical resection [2], resulting in impaired survival. In our case, we believe the monobloc macroscopic tumor removal combined followed by spinal radiation therapy resulted in a satisfactory good survival of 4 years despite a histological subtype associated with a poor prognosis.
The mass had a right intrapleural and retropericardial location. Considering its location we opted for a right posterolateral thoracotomy to have good exposure. This approach allowed us to control both the spine and the oesophagus, and to perform a right lung resection, if needed. The 8th intercostal space was chosen as it was in front of the mass.
In addition, it remains sometimes impossible to confirm preoperatively if surrounding anatomical structures are invaded or not. In our case, we discovered, during the procedure, an invaded aorta and we realized the resection of an aortic segment through right thoracotomy. The exposure requires the careful release of the esophagus on almost all its intra thoracic portion and to delicately retract the heart up and the diaphragm down. We believe such a complex and major surgical procedure requires good collaboration between thoracic surgeons and anesthesiologists and should be performed in tertiary centers.
Conclusion
We report the exceptional case of a liposarcoma of the mediastinum with thoracic aorta invasion. Surgical removal was obtained through right posterolateral thoracotomy and required replacement of a segment of descending thoracic aorta. This unusual approach can be considered for malignant tumor resection.
Declarations
Consent statement: Ethical Review Board approval of Limoges Hospital Center: N°577-2022-233 (29 September 2022). ERB have not recommended personal consent request because patient is dead.
Disclosure statement: Non to declare.
References
- Decker JR, deHoyos AL, DeCamp MM. Succesful Thoracoscopic Resection of a Large Mediastinal Liposarcoma. Ann Thorac Surg. 2011; 92: 1499-1501.
- Chen M, Yang J, Zhu L, et al. Primary liposarcoma: A clinicopathologic study and prognostic analysis of 23 cases. J Cardiothorac Surg. 2014; 9: 119
- Lin YY, Su WF. Liposarcoma of the Anterior Mediastinum and Neck. N Eng Med. 2010; 363: 9.
- Liu L, Wei X, Pan T. A giant primary myxoidliposarcoma of the posterior mediastinum. Eur J Cardiothorac Surg. 2010; 37: 958.
- Boland JM, Colby TV, Folpe AL. Liposarcomas of the mediastinum and thorax: A clinicopathologic and molecular cytogenetic study of 24 cases, emphasizing unusual and diverse histologic features. Am J Surg Pathol. 2012; 36: 1395-1403.