
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
The “reversible perfusion-metabolism pattern” of radionuclide myocardial PET imaging in Takotsubo Cardiomyopathy: A case report
Zhao Ma1; Dongfeng Zhang1; Wei Dong2; Hongzhi Mi2; Xiantao Song1*
1Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, 100029, P. R. China.
2Department of Nuclear Medicine, Beijing Anzhen Hospital, Capital Medical University, Beijing, 100029, P. R. China.
*Corresponding Author : Xiantao Song
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Anzhen Road Chaoyang District, Beijing, 100029, P. R. China.
Tel: 86-010-64456371;
Email: song0929@mail.ccmu.edu.cn
Received : Nov 09, 2022
Accepted : Nov 29, 2022
Published : Dec 06, 2022
Archived : www.jcimcr.org
Copyright : © Song X (2022).
Abstract
Background: Takotsubo Cardiomyopathy (TTC) is known as a syndrome of transient and acute left ventricular dysfunction caused by emotional and physiological stressors. Due to a variety of complications in the acute phase, recently, there has been increased attention to TTC. Although an increasing emphasis is put on the value of multimodality imaging in TTC, the role of radionuclide myocardial imaging is rarely mentioned.
Case presentation: We described a case report of a 52-year-old male who was diagnosed with TTC and characterized the radionuclide myocardial imaging in detail at baseline and during follow-up. Conclusion: Radionuclide myocardial imaging can be non-invasively applied for clinical decision-making and prognostic evaluation of TTC.
Keywords: Takotsubo cardiomyopathy; Radionuclide myocardial imaging; 99mTc-MIBI SPECT; 18F-FDG PET.
Abbreviations: TTC: Takotsubo Cardiomyopathy; LV: Left Ventricular; ECG: Electrocardiogram; ACS: Acute Coronary Syndrome; CMR: Cardiovascular Magnetic Resonance; CCTA: Coronary Computed Tomography Angiography; CK: Creatine Kinase; CK-MB: Creatine Kinase-MB Isoenzyme; NT-Pro BNP: N‐Terminal Pro‐B‐Type Natriuretic Peptide; ESR: Erythrocyte Sedimentation Rate; Hs-Ctni: High-Sensitivity Cardiac Troponin I; BNP: B-Type Natriuretic Peptide; EF: Ejection Fraction; 99mtc-MIBI SPECT: 99mtc-Methoxy-Isobutyl-Isonitrilesingle-Photon Emission Computed Tomography; 18F-FDG PET: 18F-Fluorodeoxyglucose Positron Emission Tomography.
Citation: Ma Z, Zhang D, Dong W, Mi H, Song X. The “reversible perfusion-metabolism pattern” of radionuclide myocardial PET imaging in Takotsubo Cardiomyopathy: A case report. J Clin Images Med Case Rep. 2022; 3(12): 2187.
Background
TTC was first reported in 1990 in Japan by Sato et al [1], which is known as a syndrome of transient and acute Left Ventricular (LV) systolic dysfunction caused by emotional and physiological stressors [2]. Clinically, the main manifestations are chest pain, Electrocardiogram (ECG) abnormalities (ST-segment elevation, T-wave inversion, QT interval prolongation), and mildly elevation of myocardial markers. Therefore, it is hard to distinguish it from the Acute Coronary Syndrome (ACS). TTC currently comprises around 1-2% of all the patients suspecting acute coronary syndrome each year [3]. As a self-limiting disease, TTC patients’ cardiac function usually recovers spontaneously within a few weeks, whereas various complications can occur during the acute phase, such as ventricular arrhythmia, acute heart failure, outflow tract obstruction, cardiac rupture, etc. When no significant stenosis is found during coronary angiography and echocardiography shows mid-to-apical wall motion abnormality in patients presenting with ACS, the TTC diagnosis should be considered seriously.
An increasing emphasis is put on the value of multimodality imaging in TTC, especially Cardiovascular Magnetic Resonance (CMR) and coronary Computed Tomography Angiography (CCTA). However, the role of radionuclide myocardial imaging is rarely mentioned. Myocardial rest perfusion and glucose metabolism imaging can help to figure out the mechanism of TTC, particularly the aspect of microvascular dysfunction [4]. In this case, we presented a 52-year-old man who diagnosed with TTC and characterized the radionuclide myocardial imaging in detail. We found radionuclide myocardial imaging can be non-invasively applied for clinical decision-making and prognostic evaluation of TTC.
Case presentation
A 52-year-old male presented to the community hospital due to the paroxysmal chest tightness and shortness of breath. The biochemical examination showed Creatine Kinase (CK) 75 U/L (38-174 U/L), Creatine Kinase-MB Isoenzyme (CK-MB) 14.1 U/L (0-24 U/L), N‐terminal pro‐B‐type Natriuretic Peptide (NT-pro BNP) 2488 pg/mL (0-300 pg/mL) at that time. The ECG showed T-wave inversion in the leads II, III, aVF, V5-V6 and the echocardiography showed LV generalized dyskinesia. Since the patient’s sick condition, he was referred to our hospital. The patient had a history of hypertension for 5 years, diabetes for 4 years, hyperlipemia for 2 years, and he failed to follow advice regarding regular medication and supervision. The patient had a smoking history of 20 cigarettes/day for 20 years. No obvious abnormality was found in the physical examination. The patient had a normal blood routine examination and Erythrocyte Sedimentation Rate (ESR). A series of cardiacbiomarker were collected at admission: high-sensitivity cardiac troponin I (hs-cTNI) 4.1 pg/mL (0-19.8 pg/mL), CK 41 U/L (50-310 U/L), CK-MB 0.7 ng/mL (0.6-6.3 ng/mL), B-type Natriuretic Peptide (BNP) 142 pg/mL (0-100 pg/mL), NT-pro BNP 403 pg/mL (0-125 pg/mL), D-dimer 384 ng/ml (0-243 ng/ml). Echocardiography demonstrated the typical ballooning of the apical segments, and hypokinesis of the right ventricular free wall, the basal to mid segments of the left ventricle inferior-posterior wall and all apical segments of LV. The LV Ejection Fraction (LVEF) was only 25%.
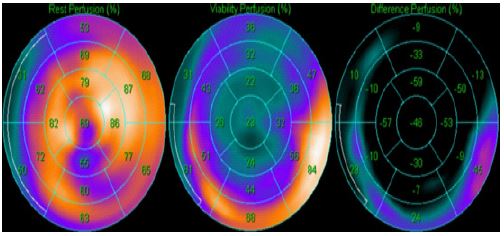
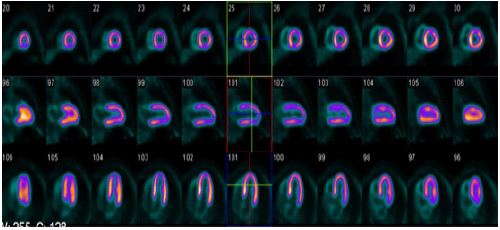
The patient’s symptoms and past medical history suggested that the patient might have unstable angina. Myocardial rest perfusion and metabolism imaging were performed by means of 99mTc-MIBI Single-Photon Emission Computed Tomography (SPECT) and 18F-FDG Positron Emission Tomography (PET). The myocardial rest perfusion indicated the left ventricular cavity was enlarged and spherical remodeling apex, severely decreased perfusion of the apical segment, inferior wall regions (including apical and mid), and mildly decreased perfusion of basal segments (including inferior, posterior-lateral and anterior wall) regions. The reduced perfusion area was about 32% (Figures 1,3). The metabolic imaging indicated that besides the basal segment of the posterior septal, inferior and posterior-lateral wall, the distributions of the radioactivity of the remaining segments were sparse (Figures 2,3). The basal segment of the inferior and posterior-lateral wall (about 12%) showed a pattern of perfusion/metabolism mismatch. And the uptake of 18F-FDG was markedly reduced relative to perfusion (Figure 3). The LVEFs were 20% and 26% by semi-quantitative analysis of 99mTc-MIBI SPECT and 18F-FDG PET respectively. In addition, except for the basal segment of the inferior and posterior-lateral wall, the wall motion and thickening rate of the resting LV segments were weakened. The hypoperfusion regions were significantly smaller than the akinesia regions. Considering that the patient had a large range of hibernating myocardium and could benefit from revascularization, the patient underwent coronary angiography. No significant stenosis was observed during coronary angiography.
An in-depth history of the patient’s emotional state demonstrated that a sudden illness of his family member was identified as his emotional stressor. The possibility of a diagnosis of TTC should be considered. During the admission, beta-blocker and sacubitril/valsartan were applied to meliorate the ventricular remodeling, digoxin to enhance cardiac output, and nicorandil to improve microcirculation. Furosemide and spironolactone were applied for diuresis. Other therapies included antiplatelet, antihypertension, lipid-lowering and glucose-lowering therapy. Diazepam was also given to improve sleep quality. Thereafter, the symptoms were relieved and the patient was discharged 15 days following admission.


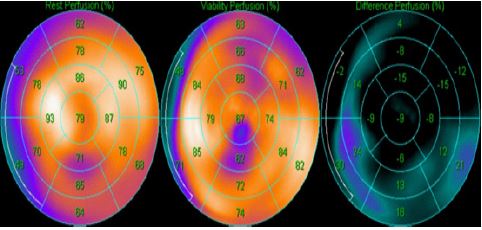
The patient was closely followed up. The stressor disappeared in the half-month and the symptoms improved remarkably 1 month after discharge. He completed an outpatient visit after 6 months. The ECG showed the T-wave reinversion in the leads II, III, a VF. The echocardiography showed the structure and function of the heart were fully restored. The LVEF byechocardiography increased from 25% to 60%. The patient repeated radionuclide myocardial imaging. The myocardial rest perfusion imaging indicated that the area of perfusion deficit decreased from 32% to 15% (Figure 4,6). The myocardial metabolism imaging indicated that except for the apical segment of the inferior wall, the tracer distribution of the rest segments returned to normal (Figure 5,6). The LVEFs by 99mTc-MIBI SPECT and 18F-FDG PETsemi-quantitative analysis increased from 20% to 57%, and 26% to 57%, respectively. The regional wall motion and wall thickening rate were significantly improved.

Discussion and conclusion
The Mayo Clinic Criteria have been the most commonly applied for TTC diagnosis [5]. The followings should be satisfied: (1) Transient hypokinesia, akinesis, or dyskinesis of the LV mid-segment, with or without apical involvement; the regional wall motion abnormalities extend beyond a single epicardial vascular distribution; a physical or emotional stressor is often, but not always present. (2) No obstructive coronary artery disease or angiographic evidence of acute plaque rupture. (3) New-onset ECG abnormalities (either ST-segment elevation and/or T-wave inversion) or modest elevation of cardiac troponin. (4) No pheochromocytoma or myocarditis.
The patient had a definite stressor and ECG showed that there was a new-onset T-wave inversion in the inferior wall leads. No obvious stenosis was found during coronary angiography. But there was an extensive area of abnormal ventricular wall motion according to radionuclide myocardial imaging and echocardiography. He had neither past history of pheochromocytoma nor evidence of myocarditis such as recent infection, elevated levels of leukocytes or myocardial markers. The final diagnosis was TTC according to Mayo criteria.
A matched, mismatched, or reverse mismatched perfusion-metabolism pattern can occur in patients with TTC. Jelena R. Ghadri etal [6] performed 13N-NH3myocardial perfusion and 18F-FDG myocardial metabolism imaging in a patient with TTC and found not only the systolic dysfunction in the apical and mid-segment of the LV, but also a simultaneous matched perfusion/metabolism pattern in the same regions. The hyperemic Myocardial Blood Flow (MBF) and Coronary Flow Reserve (CFR) were globally decreased. After 3 months, the PET/CT-follow-up-study documented full recovery. They believed microvascular dysfunction plays an important role in TTC. Mauro Feola et al [7] identified a significant inverse metabolism perfusion mismatch by performing 13N-NH3 myocardial perfusion and 18F-FDG myocardial metabolism imaging in three women who were experiencing the acute phase of TTC. And the apical segment CFR decreased to a great extent. It suggested a transient metabolic disorder at the level of myocardial cellular and microvascular dysfunction in the apical segment of LV.
By analyzing myocardial perfusion and metabolism imaging, the hibernating myocardium can be identified if the perfusion and metabolism are mismatched. It can also be judged by evaluating the abnormalities area between regional wall motion and myocardial perfusion. By accessing whether hibernating myocardium exists and the area of it, clinical decisions and prognosis evaluation can be made consequently. The patient underwent radionuclide myocardial imaging which indicated various segments had a mismatched perfusion/metabolism pattern. Meanwhile, the LV function quantitative analysis concluded the range of perfusion defected was smaller than that of dysfunction. Hence, the existence of a large area of hibernating myocardium could be deduced, which means the patient might have a favorable prognosis. Considering there was no significant epicardial stenosis, the microvascular dysfunction might play a key role in the development of the patient’s condition.
The radionuclide myocardial imaging also indicated the patient had reduced uptake of 18F-FDG, whereas normal or slightly impaired uptake of 99mTc-MIBI.The same phenomenon was also reported in other case reports [8,9]. A series of animal trials [10,11] have demonstrated that high-dose catecholamines could depress glucose uptake in rat heart. Alpha-1 adrenoreceptor could be simulated by norepinephrine, which might play an important role in the ischemia-mediated increase in glucose transporter trafficking. Therefore, Yoshida et al [12] speculated that a metabolic disorder caused by catecholamine surging could be one of the pathogenesis of this condition.
After a comprehensive assessment, an appropriate clinical decision emerged subsequently: Beta-blocker was given to alleviate the toxic effects of catecholamine; Nicorandil to ameliorate microcirculatory disturbance; Diazepam to improve sleep quality; the rest treatments were as described above. The symptoms improved remarkably 1 month after discharge. After 6 months, the echocardiography showed the structure and function of the heart were fully restored. The myocardial rest perfusion/metabolism imaging and regional wall motion/thickening rate were all significantly improved. The reversible radionuclide myocardial imaging further affirmed our diagnosis and the plausibility of the treatment scheme.
In this case, we find that LV function quantitative analysis with myocardial perfusion and metabolism, radionuclide myocardial imaging can be non-invasively applied for clinical decision-making and prognostic evaluation of TTC. However, further studies are still needed to confirm its clinical utility and potential replication.
Declarations
Ethics approval and consent to participate: This study was performed in accordance with the principles of the Declaration of Helsinki, and the patient provided informed consent. As the current study was a case report, there was no ethics committee to approve the study.
Consent for publication: Written informed consent was gained from the patient for the publication of this article.
Availability of data and materials: Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Competing interests: The authors declare that they have no conflicts of interest.
Funding: This study was supported by the Science and Technology Project by Chaoyang District Bureau Science Technology and Information Technology of Beijing (NO. CYSF2114) and the Youth Program by Beijing Municipal Administration of Hospital (NO. QML20210602).
Author contribution: Zhao Ma wrote the manuscript and was first author. Wei Dong and Dongfeng Zhang contributed to the data collection and revised the manuscript. Xiantao Song and Hongzhi Mi helped to conceive the topic. All authors read and approved the final manuscript.
Acknowledgments: The authors thank Feng Xu who performed the coronary angiography as well as Yulong Guan and Ziqi Zhang who helped with the manuscript revision.
References
- Sato H, Tateishi H, Uchida T, Dote K, Ishihara M, et al. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. In Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure Tokyo. Kodama K, Haze K, Hori M. Eds.; Kagakuhyoronsha Publishing Co.: Tokyo, Japan. 1990; 56–64.
- Kurowski V, Kaiser A, von Hof K, et al. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): Frequency, mechanisms, and prognosis. Chest. 2007; 132: 809-816.
- Medina de Chazal H, Del Buono MG, Keyser-Marcus L, et al. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018; 72: 1955-1971.
- Vitale C, Rosano GM, Kaski JC. Role of Coronary Microvascular Dysfunction in Takotsubo Cardiomyopathy. Circ J. 2016; 80: 299-305.
- Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am Heart J. 2008; 155: 408-417.
- Ghadri JR, Dougoud S, Maier W, et al. A PET/CT-follow-up imaging study to differentiate takotsubo cardiomyopathy from acute myocardial infarction. Int J Cardiovasc Imaging. 2014; 30: 207-209.
- Feola M, Chauvie S, Rosso GL, et al. Reversible impairment of coronary flow reserve in takotsubo cardiomyopathy: A myocardial PET study. J Nucl Cardiol. 2008; 15: 811-817.
- Albert CL, White KT, Cremer PC, et al. Stress for a stressed out heart: Classic cardiac PET findings in takotsubo cardiomyopathy. J Nucl Cardiol. 2019; 26: 679-680.
- Bybee KA, Murphy J, Prasad A, et al. Acute impairment of regional myocardial glucose uptake in the apical ballooning (takotsubo) syndrome. J Nucl Cardiol. 2006; 13: 244-250.
- Egert S, Nguyen N, Schwaiger M. Contribution of alpha-adrenergic and beta-adrenergic stimulation to ischemia-induced glucose transporter (GLUT) 4 and GLUT1 translocation in the isolated perfused rat heart. Circ Res. 1999; 84: 1407-1415.
- Huang MT, Lee CF, Dobson GP. Epinephrine enhances glycogen turnover and depresses glucose uptake in vivo in rat heart. FASEB J. 1997; 11: 973-980.
- Yoshida T, Hibino T, Kako N, et al. A pathophysiologic study of tako-tsubo cardiomyopathy with F-18 fluorodeoxyglucose positron emission tomography. Eur Heart J. 2007; 28: 2598-2604.