
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Tympanic membrane cholesteatoma: A
case report in an adult and a child
Estefanía Miranda1; Victoria García-Peces1,2; Mar Martínez-Ruiz-Coello1; Cristina García-García1; Agustina Arbía; Guillermo Plaza1,2*
1Otolaryngology Department, Hospital Universitario de Fuenlabrada. Universidad Rey Juan Carlos, Madrid, Spain.
2Otolaryngology Department, Hospital Universitario La Zarzuela, Madrid, Spain.
*Corresponding Author : Guillermo Plaza
Otolaryngology Department, Hospital Universitario de Fuenlabrada, Universidad Rey Juan Carlos, Madrid, Spain.
Otolaryngology Department, Hospital Universitario La Zarzuela, Madrid, Spain.
Email: guillermo.plaza@salud.madrid.org
Received : Nov 10, 2022
Accepted : Dec 02, 2022
Published : Dec 09, 2022
Archived : www.jcimcr.org
Copyright : © Plaza G (2022).
Abstract
Introduction and objective: Tympanic Membrane Cholesteatoma (TMC) is a rare pathology of unknown etiology which occurs more frequently in pediatric population, being the presentation in adults exceptional. Resection of the lesion is usually the surgical treatment through a transcanal approach.
Method: We report two patients, one adult and one pediatric, presenting TMC with no previous otologic history. We explain diagnosis and management, detailing complementary tests and final treatment.
Discussion: TMC is a rare pathology. Despite this, it should be considered when a whitish nodular lesion appears in the tympanic membrane in patients with no previous otologic history. Currently, there are few cases published in the literature.
Conclusions: TMC is a rare and infrequent entity. Due to the limited literature on the subject, the criteria to classify a TMC as congenital or acquired and its possible pathogenic mechanisms are still under discussion. The lesion is usually limited to the tympanic membrane and the treatment of choice is surgery.
Keywords: Tympanic membrane cholesteatoma; Intratympanic cholesteatoma; Tympanic membrane; Congenital cholesteatoma.
Abbreviations: TMC: Tympanic Membrane Cholesteatoma.
Citation: Miranda E, Peces VG, Coello MMR, García GG, Plaza G, et al. Tympanic membrane cholesteatoma: A case report in an adult and a child. J Clin Images Med Case Rep. 2022; 3(12): 2192.
Introduction
Congenital cholesteatomas of the middle ear are infrequent, but even less frequent in the tympanic membrane [1,2]. Tympanic Membrane Cholesteatoma (TMC) is a rare pathology, as there are few cases reported in the literature. It is of unknown etiology, which occurs more frequently in pediatric population. However, cases have also been reported in adults. The typical presentation is characterized by presentation in patients with no previous otologic history, that is, chronic otitis media, trauma or otologic surgery [1]. In most cases, the lesion is limited to the tympanic membrane with the middle ear, ossicular chain, attic and mastoid cells being normal. In the few cases reported, resection of the lesion is usually the surgical treatment, being the transcanal approach the treatment of choice. We present the case of two patients: an adult and a child with a diagnosis of TMC. The aim of this article is to expose an uncommon pathology such as TMC.
Case presentations
Case 1
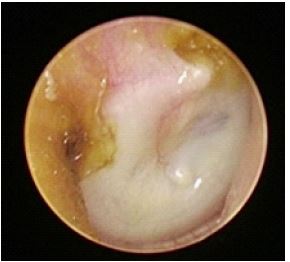
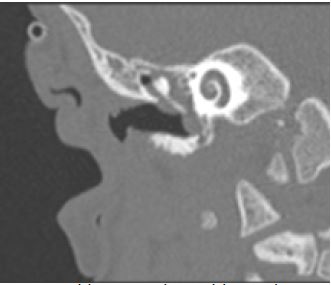
We present the case of a 66-year-old male patient who came to the otolaryngology office in our hospital for otalgia of the right ear with no other symptoms. He had no relevant pathologic history, denied any history of otitis, trauma or previous otologic surgeries. Physical examination by otomicroscope revealed a nodular lesion in the lower quadrants of the tympanic membrane (Figure 1). Audiometry and tympanogram were normal. A CT scan was performed, showing a lesion with soft tissue attenuation at the tympanic membrane level, with no alterations at the middle or inner ear level (Figure 2).
Surgical treatment was proposed with resection of the lesion through a transcanal approach. During the procedure, the edges of the lesion were detached, leaving the tympanic membrane intact (Video 1). The diagnosis of TMC was confirmed by histopathology. The patient was evaluated 6 months after with a normal tympanic membrane (Figure 3).



Case 2
A 1-year-old male patient was evaluated in the otorhinolaryngology office referred by his primary care physician for suspicion of a foreign body in the left ear. The mother perceived adequate hearing. He had no previous otologic history. Physical examination revealed a nodular lesion in the inferior quadrants of the tympanic membrane (Figure 4). A CT scan was performed, showing otomastoid occupation without destruction of local structures (Figure 5). Therefore, a transcanal resection of the TMC was performed without violating the integrity of the tympanic membrane. Myringotomy was performed suctioning mucus. The tympanomeatal flap was lifted and the middle ear was explored without evidence of cholesteatoma. A transtympanic tube was placed. The diagnosis of TMC was confirmed by histopathology. After four years of follow-up tympanic membrane remained intact, with no recurrence of TMC (Figure 6).


Discussion
Congenital cholesteatoma represents 2-5% of all cholesteatomas observed [1]. However, it is believed that TMC is significantly rarer than congenital middle ear cholesteatoma and that these two entities may have a different pathogenesis [2].
The first description of a TMC was in 1863 by Hinton, who described it as a “sebaceous tumor” located on the external surface of the tympanic membrane [3]. In 1936, Teed found a total of five congenital cholesteatomas in the literature that were compatible with a TMC [4]. In 1997, Weber and Adkins described three other cases of TMC in children with no previous otologic history [5]. More recently, in 2016 and 2019, Predruzzi et al. and Cheon et al. respectively described the cases of patients with this pathology, each of these cases had a small mass on the external surface of the TM [6,7].
The etiopathogenesis of TMC is still unknown and seems to be unrelated to congenital cholesteatoma of the middle ear. In cases of otitis previa, the origin of TMC can be explained by Sade et al. who observed that inflammation can lead to metaplasia of mesenchymal tissue within the tympanic membrane, which may result in conversion to squamous epithelium [8]. On the other hand, Ruedi proposed that inflammation may develop proliferation of the basal cell layer, from the squamous epithelium of tympanic membrane into cones protruding in it to form a cholesteatoma in response to an inflammatory process [9]. Our patients differ from this theory because of the absence of prior middle ear pathology.
When cholesteatoma develops in subjects with no history of previous inflammatory processes of the external and middle ear, as in the cases we present, an embryologic origin is suspected. This could be explained by the persistence of an epidermoid formation, derived from the first branchial groove that normally regresses after the 33rd week of gestation [4,10,11]; a theory that would apply to our patients, since they do not have a previous otologic history.
The biggest series reported of TMC was done by Reddy et al. [12], including 15 cases ranging in age from 6 months to 34 years, most of them younger than 4 years. There were no sex differences and no quadrant of the tympanic membrane was more likely to present TMC. In our case, the two patients reported were male and both cases presented in inferior quadrants. We present the case of the oldest patient with TMC ever reported in the literature.
As patients with TMC do not have a history of otorrhea or hearing loss, the lesion may go unnoticed for many years. Patients with this pathology have no initial complaint of hearing loss. It is believed that an undetected TMC tends to expand into the middle ear spaces thus causing different complications such as involvement of the ossicles and consequent auditory conduction disorders.
Computed tomography provides precise information about the mass and the relationship with the ossicles and middle ear spaces. In addition, it allows surgical planning in case of middle ear involvement [5,13].
Ching et al in 2017 performed a systematic review where they observed that most patients deny previous otologic history. On the other hand, they observed that there is a significant positive correlation between patient age and cholesteatoma size, because cholesteatoma gradually increases with time [1].
Therefore, several authors recommend the necessary surgical treatment as these lesions may progress to middle ear involvement. A transcanal approach is recommended as long as the cholesteatoma can be detached from the tympanic membrane and the fibrous cap of the tympanic membrane is kept intact. If the TMC is suspected to extend into the middle ear, as in the case of our second patient, a tympanoplasty or a more extensive approach will be necessary [1,14,15]. Due to the few reported cases, the optimal management of this pathology is unclear. Data on the natural history and prognosis of this pathologic entity are lacking.
Recurrence of TMC appears to be lower than cholesteatoma of the middle ear [1]. However, postoperative follow-up of these patients is necessary.
Conclusion
Tympanic membrane cholesteatoma is a rare and infrequent entity that should be taken into consideration both in pediatric age and in adults, always when a nodular lesion external to the tympanic membrane is observed. Due to the limited literature on the subject, the criteria to classify a TMC as congenital or acquired and its possible pathogenic mechanisms are currently under discussion. The lesion is usually limited to the tympanic membrane and the treatment of choice is surgery.
Declarations
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Ching H, Spinner A, Ng M. Pediatric tympanic membrane cholesteatoma: Systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol. 2017; 102: 21–27.
- Kim S, Haupert M. Congenital cholesteatoma of the tympanic membrane. Otolaryngology– Head, Neck Surgery. 2002; 127: 359-360.
- Hinton J. Sebaceous tumor within the tympanum originating on the external surface of the membrane tympani. Guy’s Hosp. 1863; 9: 264-268.
- Teed R, Cholesteatoma verum tympani: Its relationship to the first epibranchial placode, Arch. Otolaryngol. 1936; 24: 455–474.
- Weber P, Adkins W. Congenital Cholesteatomas in the Tympanic Membrane. Laryngoscope. 1997; 107: 1181-1184.
- Pedruzzi B, Mion M, Comacchio F. Congenital Intratympanic Cholesteatoma in an Adult Patient: A Case Report and Review of the Literature. J Int Adv Otol. 2016; 12: 119-124.
- Cheong TY, Jo YS, Kim HS, Choi IS, Lee JM, et al. Intratympanic Membrane Congenital Cholesteatoma Removal Using an Endoscopic System: A Case Report. Ear Nose Throat J. 2019; 98: 188-189.
- Sade J, Ba Biacki A, Pinkus G. The metaplastic and congenital origin of cholesteatoma. Acta Orolaryngol. 1983; 96: 119-129.
- Ruedi L. Cholesteatoma formation in the middle ear in animal experiments. Acta Otolaryngnol. 1959; 50: 233-240.
- Michaels L. An epidermoid formation in the developing middle ear: Possible source of cholesteatoma, J. Otolaryngol. 1986; 15: 169–174.
- Wang R, Hawke M, Kwok P. The epidermoid formation (Michael’s structure) in the developing middle ear. J. Otolaryngol.1987; 16: 327–330.
- Reddy C, Goodyear P, Ghosh S, Lesser T. Intratympanic membrane cholesteatoma: A rare incidental finding. Eur Arch Otorhinolaryngol. 2006; 263: 1061-1064.
- Sakaida H, Takeuchi K. Intratympanic membrane congenital cholesteatoma. Ear Nose Throat J. 2015; 94: 256-260.
- Matsuda H, Satake K, Takahashi M, Horiuchi C, Tsukuda M, et al. Two cases of congenital cholesteatoma of the tympanic membrane. Indian J Otolaryngol Head Neck Surg. 2012; 64: 79-81.
- Grindle C, Shah G, O´Reilly R. Intratympanic membrane cholesteatoma: A rare bilateral presentation within a single-institution case series. International Journal of Pediatric Otorhinolaryngology. 2011; 6: 373–375.