
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Laryngeal leishmaniasis: Still a challenging diagnosis
Cristina García-García1; Andrés Navarro1; Mar Martínez-Ruiz-Coello1; Estefanía a Miranda1; Agustina Arbía1; Guillermo Plaza1,2*
1Otolaryngology Department, Hospital Universitario de Fuenlabrada. Universidad Rey Juan Carlos, Madrid, Spain.
2Otolaryngology Department, Hospital Universitario La Zarzuela, Madrid, Spain.
*Corresponding Author : Guillermo Plaza
Otolaryngology Department, Hospital Universitario de Fuenlabrada. Universidad Rey Juan Carlos, Madrid, Spain.
Otolaryngology Department, Hospital Universitario La Zarzuela, Madrid, Spain.
Email: gplaza.hflr@salud.madrid.org
Received : Nov 15, 2022
Accepted : Dec 05, 2022
Published : Dec 12, 2022
Archived : www.jcimcr.org
Copyright : © Plaza G (2022).
Abstract
Introduction and objective: Laryngeal leishmaniasis is a rare disease that should be considered in patients presenting with hoarseness or dyspnea having risk factors as immunodeficiency (systemic or local) and previous Leishmania infections
Method: We report an adult patient with history of dysphonia, cough and episodes of nausea and vomiting due to laryngeal leishmaniasis. We explain its diagnosis and management, detailing complementary tests and final treatment.
Discussion: There are few cases published of laryngeal isolate presentation of Leishmania infection and a late diagnosis of the disease is usually made. It is essential to keep this disease in mind to shorten the delay of diagnosis, especially in patients with immunodeficiency clinical history, previous renal transplantation, chronic inhaled steroids treatments, or living in endemic areas.
Conclusions: Laryngeal leishmaniasis is an uncommon entity that should be considered in patients presenting with hoarseness and dyspnea, especially those who come from endemic areas.
Keywords: Laryngeal leishmaniasis; Leishmania spp; Immunodeficiency; Hoarseness.
Abbreviations: CT: Computed Tomography; PCR: Polymerase Chain Reaction.
Citation: Garcia CG, Navarro A, Coello MMR, Miranda E, Plaza G, et al. Laryngeal Leishmaniasis: Still a Challenging Diagnosis. J Clin Images Med Case Rep. 2022; 3(12): 2194.
Introduction
Leishmania spp is a protozoon transmitted by the bite of the female Phlebotomus or Lutzomyia sandflies. The Leishmania species and the immune condition of the patient influence the type of disease that might develop. Leishmania may cause cutaneous, mucocutaneous, or visceral infections. The clinical spectrum differs from one patient to another, ranging from a banal skin lesion to a visceral life-threatening condition.
The involvement of the larynx is rare, and only a few cases have been reported [1-13]. Described risk factors related to laryngeal leishmaniasis are immunodeficiency (systemic or local), previous renal transplantation, chronic inhaled steroids treatments, or living in endemic areas, and previous Leishmania infections.
Case presentation
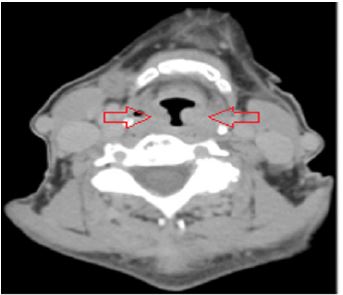
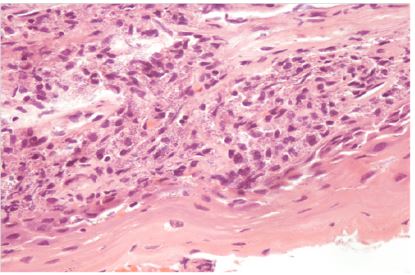
We present the case of a 69-year-old woman, a local resident in Fuenlabrada, Madrid (Spain). She had a three-year clinical history of dysphonia, cough and episodes of nausea and vomiting. She was a non-smoker and suffered from severe asthma and rheumatoid arthritis that had required treatment with corticosteroid inhalers, injections of methotrexate, and low doses of oral prednisone. The initial flexible laryngoscopy was unremarkable, showing just erythematous vocal folds (Figure 1). Progressively, her condition worsened, and the findings of the laryngeal exploration changed to edematous swelling patches that fluctuated over the epiglottis, arytenoids, and false and true vocal cords (Figure 2, QR. 1) confirmed by a CT scan, showing a marked laryngeal inflammatory stenosis (Figure 3). She was then treated with higher doses of steroids and antibiotics, under the suspicion of rheumatic involvement of the larynx. However, after several months, the patient presented a severe episode of dyspnea. A bilateral CO2-laser cordectomy and tracheotomy were performed. The histopathological results suggested an inflammatory process compatible with leishmaniasis, confirmed by Polymerase Chain Reaction (PCR) of the laryngeal samples, positive for Leishmania (Figure 4). Blood samples were negative. She did not remember any cutaneous lesion and had no other mucosal lesions, or in rhynopharynx nor the nasal cavity. She neither had visceral involvement and had not recently traveled abroad.
Chronic laryngeal lesions might be due to tumoral, infectious, or inflammatory processes. In smoker patients with laryngeal isolated lesions, the principal differential diagnosis is carcinoma. Moreover, infectious laryngitis syndromes can be caused by bacterial or parasitic agents like Mycobacterium tuberculosis, Paracoccidioides spp, etc. Similarly, Leishmania spp should be considered, especially if the nasal mucosa is also involved.
On the other hand, patients who suffer autoimmune diseases with chronic inflammatory manifestations, such as rheumatoid arthritis, may have laryngeal lesions. Either way, the key to a correct assessment of the disease is the histology of the lesions, but several clinical features may orientate the diagnosis.
She underwent several cycles of antibiotics and steroids, and even surgery (tracheotomy and laser cordectomy) before reaching the final diagnosis. Afterwards, she was treated with liposomal amphotericin B in a 3 mg/kg/day dose for two weeks (total dose of 21 mg/kg) with relevant clinical improvement and complete resolution of laryngeal findings (QR. 2).
The patient is still being followed up by the Infectious Diseases Department and Otolaryngology Department every six months. After five years, she remains free of new laryngeal symptoms. During follow-up, 4 years after diagnosis, the patient received an empirical liposomal amphotericin B second cycle because of recurrent respiratory infections, even though a negative PCR for Leishmania was reported with subsequent clinical improvement. After 7 years, she remains asymptomatic.




Discussion
There are few cases published of isolate laryngeal presentation of Leishmania infection [1-13]. It is believed to be due to a direct inoculation of the protozoa to the mucosa or a migration of the microorganisms from the inoculation point. If that is the case, usually it starts affecting the oral or nasal mucosa, which may be subclinical and then migrates to the larynx.
Immunodeficiency clinical history, as HIV infection [4,7] or previous renal transplantation [5], is a common predisposing comorbidity. However, laryngeal leishmaniasis has also been reported in immunocompetent patients [2,6,9-11]. In these cases, chronic inhaled steroids treatments, smoking and a personal history of Leishmania infection are risk factors described in the literature [9]. Our case has a long history of chronic inhaled steroids treatments.
Moreover, it is essential to consider this infection in patients from endemic areas, like certain areas in Spain and Southern Europe. It should be noted that the area where the patient lives is considered to have the largest community outbreak diagnosed of leishmaniasis in Europe [14].
Furthermore, this patient had suffered from a rheumatologic disease that hindered its immune response which, in addition to immunosuppressant treatments, might have been her main risk factor.
The delay in diagnosing laryngeal leishmaniasis, like our case, is commonly referred to in the literature and is usually explained by its low incidence and broad differential diagnosis. Thus, a biopsy is necessary to state the correct diagnosis as soon as possible [11,15,16]. Surgery has been reported as a successful treatment [8], but in our case the pharmacological treatment was effective and resolved the symptoms and lesions. It is essential to keep this disease in mind to shorten the delay of diagnosis.
Conclusion
Laryngeal leishmaniasis is an uncommon entity that should be considered in patients presenting with hoarseness and dyspnea, especially those who come from endemic areas. A complete head and neck exam is mandatory and a biopsy will allow histopathological and microbiological findings that are the diagnostic key. This pathology should be appropriately treated with liposomal amphotericin B until clinical improvement is achieved.
Declarations
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Grant A, Spraggs PD, Grant HR. Laryngeal leishmaniasis. Laryngol Otol J, et al. 1994; 108: 1086-1088.
- Cocuzza S, Strazzulla A, Pinzone, M. Isolated Laryngeal Leishmaniasis in Immunocompetent Patients: An Underdiagnosed Disease. Case Rep Infect Dis. 2013; 2013: 165409.
- Teemul TA, Giles-Lima M, Williams J. Laryngeal leishmaniasis: Case report of a rare infection. Head Neck. 2013; 35: E277-E279.
- Cánovas DL, Carbonell J, Torres J. Laryngeal leishmaniasis as initial opportunistic disease in HIV infection. J Laryngol Otol. 1994; 108: 1089-1092.
- Jha PK, Vankalakunti M, Siddini V. Postrenal transplant laryngeal and visceral leishmaniasis—a case report and review of the literature. Indian J Nephrol. 2012; 22: 301-303.
- Casero R, Laconte L, Fraenza L. [Recidivant laryngeal leishmaniasis: An unusual case in an immunocompetent patient treated with corticosteroids]. Rev Argent Microbiol. 2010; 42: 118-121.
- González-Anglada MI, Peña JM, Barbado FJ. Two cases of laryngeal leishmaniasis in patients infected with HIV. Eur J Clin Microbiol Infect Dis Off Publ Eur Soc Clin Microbiol. 1994; 13: 509-11.
- Navarro Cunchillos M, Villanueva Marcos JL, Torre-Cisneros J. Isolated laryngeal leishmaniasis in an immunocompetent patient: Successful treatment with surgery. J Laryngol Otol. 1994; 108: 249-251.
- Roberts RM, Mukherjee J and Phillips D. Laryngeal leishmaniasis in a patient taking inhaled corticosteroids. BMJ Case Rep. 2016; 2016: bcr 2016215444.
- Moraes B, Amorim F, Caporrino J. Laryngeal Leishmaniasis. Int. Arch. Otorhinolaryngol. 2012; 16: 523-526.
- Aggarwal K, Kumar R, Bhardwaj N, Jat B, Kumar R, et al. Isolated Laryngeal Leishmaniasis: A Diagnostic Dilemma. Indian J Otolaryngol Head Neck Surg. 2019; 71: 872-875.
- Sevestre J, Reverso-Meinietti J, Butet V, Inedjian JM, Marty P, et al. Progressive dysphonia in a man living in an endemic area for Leishmania infantum. Med Mal Infect. 2019; 49: 228-230.
- Silva L, Damrose E, Fernandes AM. Laryngeal leishmaniasis, a rare manifestation of an emerging disease. Eur Ann Otorhinolaryngol Head Neck Dis. 2017; 134: 211-212.
- Horrillo L, San Martín JV, Molina L. A typical presentation in adults in the largest community outbreak of leishmaniasis in Europe (Fuenlabrada, Spain). Clin Microbiol Infect. 2015; 21: 269-273.
- Benito Navarro JR, Santaella Guardiola OM, Delgado Alvarez JF, Josephine Frandsen A, et al. Laryngeal leishmaniasis as a differential diagnosis of glottic leukoplakia. Acta Otorrinolaringol Esp. 2013; 64: 440-441.
- Renard L, Lemaignen A, Desoubeaux G, Bakhos D.
- Case report: Progressive Dysphonia and Dysphagia due to Laryngeal Leishmaniasis. Am J Trop Med Hyg. 2021; 105: 458-460.