
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cerebrotendinous xanthomatosis case report in Peru: Bilateral xanthomas of tendoachilles in a slow learner patient
Cintia Armas-Puente1,2*; Elison Sarapura-Castro1; Jeny Bazalar-Montoya1, 3; Andrea Rivera-Valdivia1,4,5; Maryenela Illanes-Manrique1; Andrea DeBarber6; Mario Cornejo-Olivas1,7
1Neurogenetics Research Center, Instituto Nacional de Ciencias Neurológicas, Lima, Peru.
2Departamento de Enfermedades Neurodegenerativas, Instituto Nacional de Ciencias Neurológicas, Lima, Peru.
3Servicio de Genética, Instituto Nacional del Niño San Borja, Lima, Peru.
4Fogarty Northern Pacific Global Health Fellowship, Peru.
5Fogarty Interdisciplinary Cerebrovascular Diseases Training Program in South America Fellow, 2020 -2021, Lima –Peru.
6Department of Chemical Physiology & Biochemistry, Oregon Health & Science University, EEUU, Peru.
7Center for Global Health, Universidad Peruana Cayetano Heredia, Lima, Peru.
*Corresponding Author : Cintia Armas Puente
Instituto Nacional de Ciencias Neurológicas 1271 Ancash St, 1503, Lima, Peru.
Email: Cintiamargoth@gmail.com
Received : Nov 11, 2022
Accepted : Dec 06, 2022
Published : Dec 13, 2022
Archived : www.jcimcr.org
Copyright : © Armas C (2022).
Abstract
Chronic diarrhea, juvenile cataracts, and tendon xanthomas, among other neurological and systemic disturbances, characterize Cerebrotendinous xanthomatosis, an autosomal recessive lipid storage disease. We report a 49-year-old Peruvian man, with no relevant family history, who experienced progressive gait disturbance and exhibited cognitive impairment. On examination, he presented cerebellar ataxia, slurred speech, and brisk tendon reflexes, enlarged Achilles’s tendons with subcutaneous mass and bilateral cataracts. Neuropsychological profile showed severe cognitive impairment. MRI revealed global cerebellar atrophy and bilateral hyper intensities in the dentate nucleus. Serum cholestanol level was high (951 ng/ml; NV: < 25 ng/ml), compatible with biochemical diagnosis of Cerebrotendinous xanthomatosis. Timely biochemical or genetic diagnostic tests should be implemented to prevent long-term complications.
Keywords: Cerebrotendinous xantomatosis; Cholestanol; CYP27A1; Xanthomas; 27- hydroxycholesterol.
Citation: Armas C, Sarapura E, Bazalar J, Rivera A, Illanes M, et al. Cerebrotendinous xanthomatosis case report in peru: Bilateral xanthomas of tendoachilles in a slow learner patient. J Clin Images Med Case Rep. 2022; 3(12): 2197.
Introduction
Cerebrotendinous Xanthomatosis (CTX) is a rare autosomal recessive disorder, caused by a deficiency of the mitochondrial enzyme 27α-sterol-hydroxylase, which is encoded by the CYP27A1 gene (2q33-qter) [1] is characterized by an abnormal accumulation of cholesterol and cholestanol affecting many tissues including the brain [2]. The most common clinical manifestations include xanthomas, cataracts, and progressive neurological dysfunction [1]. The first case of CTX was described in 1937 by van Bogart [3], since then, more than 300 cases have been reported around the world [4]. CTX is rarely reported in Latin American countries, where biochemical and genetics testing have limited availability [5]. We present a Peruvian CTX that the clinical and biochemical features revealing the diagnosis.
Case presentation
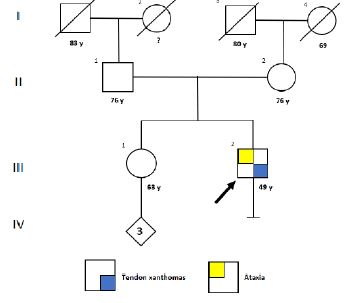
A 49-year-old male (III-1 individual, Figure 1), experienced 10-year history of gait disturbances and progressive postural instability with frequent falls, He also developed slurred speech over the last 3 years. According to his parents, he had learning difficulties at school and quit during elementary school. He had several sporadic and temporary jobs until mid-thirties. He stopped working collaborating in household chores.
The neurological examination, revealed moderate dysarthria, spasticity in all extremities with increased tendon reflexes, cerebellar ataxia, dysmetria and bilateral dysdiadokinesia, as well as multidirectional nystagmus in primary gaze. Physical examination revealed xanthomas in both Achilles’s tendons (Figure 2). The ophthalmological evaluation revealed bilateral sub capsular cataracts. Cognitive assessment demonstrated significant cognitive decline scoring 9/30 on MoCA test. Neuropsychological battery found IQ of 43 points affecting verbal fluency, attention, concentration, abstraction, calculation and working and visuospatial memory.
Nerve conduction study revealed mixed mononeuropathy in the right median nerve. MRI neuroimaging showed hypo intensities surrounded by external hyper intensities in both cerebellar dentate nucleus and global brain atrophy (Figure 3). Laboratory tests found both serum cholesterol and triglycerides in normal range. Cholestanol levels were measured in external laboratory and found it markedly elevated 951 ng/ml (NV: < 25 ng/ml). Genetic testing was not performed. Patient evolution was stationary for the next 6 months. Unfortunately, chenodeoxycholic acid was not available locally, and then he was put on atorvastatin 20 mg/day. Patient get lost on follow-ups.


Discussion
We presented a case of a normolipemic adult patient with Achilles tendinous xanthoma and progressive neurological symptoms. Head MRI studies and plasma sterol analysis support the diagnosis of Cerebrotendinous xanthomatosis. CTX is a rare and underreported lipid storage disorder. In Peru, a case with a late clinical diagnosis has been published [5]. The accumulation of cholestanol in various tissues (crystalline, tendons, brains, blood vessels, etc.) determines its clinical manifestations, our patient presented sub capsular cataracts of early onset, its often appear during the first decade of life [6], also, we observe in the Achilles tendon, which appear in the second or third decade. Neurological symptoms of our patient was slow progression, such as signs of the pyramidal tract, cerebellar ataxia and peripheral neuropathy. The learning difficulty of our patient is described since childhood, however, the cognitive deterioration was evidently progressive after the age of 30, typically cognitive decline has been described around the age of 20 [7]. The diagnosis is often overlooked at initial presentation due to the lack of a classic clinical picture, additionally routine biochemical tests of blood, urine, and cerebrospinal fluid are often normal, except plasma sterol analysis. In our case, the cholestanol dosage could be performed, obtaining 951 ng/ml (NV: 25 ng/ml), this biochemical result being compatible with the disease. The brain MRI findings support the diagnosis in our patient; the most characteristic neuroimaging lesions have seen in the basal ganglia, cerebral peduncles and dentate nucleus [7]. In case of our patient, we can observe bilateral low intensity of the dentate nuclei surrounded by hiperintensity lesions, as well as global atrophy of the cerebellum (Figure 3). This disorder can be treat with Chenodeoxycholic Acid (CDCA), which provides negative feedback for the bile acid biosynthesis pathway therefore the treatment consists in suppressing the production of cholestanol and bile alcohols [8]. Starting treatment at an early age can improve or previse neurological injurie and cognitive decline. Unfortunately, the drug is not available in Peru, so in this case we choose atorvastatin 20 mg/day.
Conclusion
We present a case with clinical and neuroimaging criteria characteristic of CTX, which was confirmed with a biochemical study of cholestanol dosage. The diagnosis of this case was very late, with a high risk of permanent sequelae despite being a disease that, treated early, can avoid many complications. The possibility of CTX should be considered in all patients with xanthomas, juvenile cataracts, and neurological manifestations. Biochemical and genetic diagnostic studies should be implemented that allow a timely diagnosis of these cases.
Declarations
Acknowledgements: The authors thank Andrea E. De Barber, Ph.D. of Department of Chemical Physiology & Biochemistry, Oregon Health & Science University for the sterol analysis.
Conflicts of interest: The authors report no disclosures relevant to the manuscript.
References
- Cali JJ, Hsieh CL, Francke U RD. Mutations in the bile acid biosynthetic enzyme sterol 27-hydroxylase underlie cerebrotendinous xanthomatosis. J Biol Chem [Internet]. 1991; 266: 7779–7783. Available from: https://pubmed.ncbi.nlm.nih.gov/2019602/
- Nie S, Chen G, Cao X, Zhang Y. Cerebrotendinous xanthomatosis: A comprehensive review of pathogenesis, clinical manifestations, diagnosis, and management. Orphanet J Rare Dis [Internet]. 2014; 9: 179. Available from: http://dx.doi.org/10.1186/s13023-014-0179-4
- Ludo Van Bogaert, Hans J Scherer EE. Une Forme Cerebrale De La Cholesterinose Generalisee (Type Particulier De Lipidose A Cholesterine). ibraires L’academie Med. 1937.
- Matthew T Lorincz, MD, PhD; Shirley Rainier, PhD; Donald Thomas, BS; John K. Fink M. Cerebrotendinous xanthomatosis: Possible Higher Prevalence Than Previously Recognized. Neurology [Internet]. 2005; 55: 601. Available from: http://dx.doi.org/10.1212/WNL.55.4.601
- Castañeda MA, Durán Espinoza C, Cabanillas Lapa J. Xantomatosis cerebrotendinosa. Reporte de un caso en el Perú: Evaluación clínica integral y estudios de neuroimágenes. Rev Neuropsiquiatr [Internet]. 2019; 82: 140. Available from: http://dx.doi.org/https://doi.org/10.20453/rnp.v82i2.3541 %0A
- Cruysberg JRM, Wevers RA, Tolboom JJM. Juvenile cataract associated with chronic diarrhea in pediatric cerebrotendinous xanthomatosis. Am J Ophthalmol [Internet]. 1991; 112: 606–607. Available from: http://dx.doi.org/10.1016/S0002-9394(14)76874-6
- Federico A, Dotti MT, Gallus GN. Cerebrotendinous Xanthomatosis Summary Diagnosis Suggestive Findings. Cerebrotendinous Xanthomatosis [Internet]. 2003; 1–20. Available from: www.ncbi.nlm.nih.gov/books/NBK1409/
- Salen G, Meriwether TW, Nicolau G, et al. Chenodeoxycholic acid inhibits increased cholesterol and cholestanol synthesis in patients with cerebrotendinous Xanthomatosis. Biochem Med [Internet]. 1975; 14: 57–74. Available from: http://dx.doi.org/10.1016/0006-2944(75)90020-4