
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A hypertensive emergency revealing renal artery
stenosis with a negative echo-doppler: A case
presentation and review of the literature
H Bendahou1*; S Zagdane1; M Selmaoui1; Y Jihane1; A Abouriche1; M Haboub²; S Arous²; G Bennouna²; S Drighil²; L Azzouzi²; R Habbal²
1Doctor, Cardiology Department, Hospital university of Casablanca, Morocco.
2Professor, Department of Cardiology, Hospital university of Casablanca, Morocco.
*Corresponding Author : H Bendahou
Cardiology Department, Hospital university of Casablanca, Morocco.
Email: bendahou.hajar1@gmail.com
Received : Nov 14, 2022
Accepted : Dec 07, 2022
Published : Dec 14, 2022
Archived : www.jcimcr.org
Copyright : © H Bendahou (2022).
Abstract
Renal Artery Stenosis (RAS) occupies a prominent place among the secondary causes of arterial hypertension (HTA), in particular resistant.
It is mainly due to atherosclerotic disease, in connection with the aging of the population and the problem of generalized atherosclerosis.
The imaging methods most commonly used for the evaluation of renal artery stenosis are echo-Doppler of the renal arteries and abdominal CT angiography.
In this article, we report the case of a 69-year-old woman who presented with a hypertensive emergency such as uncomplicated anterior myocardial infarction against a background of resistant hypertension. Our case highlights the diagnostic modalities as well as the interest of screening and monitoring of atherosclerotic stenosis to avoid impaired renal function.
Keywords: Renal artery stenosis; Hypertensive emergency; Myocardial infraction.
Citation: Bendahou H, Zagane S, Selmaoui M, Jihane Y, Abouriche A, et al. A hypertensive emergency revealing renal artery stenosis with a negative echo-doppler: A case presentation and review of the literature. J Clin Images Med Case Rep. 2022; 3(12): 2198.
Introduction
Renal Artery Stenosis (RAS) is defined as a narrowing of the renal arteries or their branches causing a decrease in blood flow.
In adults, particularly the elderly, RAS is most often associated with a diffuse atheromatous disease: Arteriopathy of the lower limbs, coronary artery disease, or carotidstenosis. In 90% of cases, the location of atherosclerotic RAS affects the ostium and the proximal third of the renal artery [1].
In addition, atherosclerotic RAS can lead to several complications: Resistant renovascular hypertension, renalischemia and cardiac decompensation, in particular the occurrence of Acute Coronary Syndromes (ACS) [2].
RAS accounts for 10-20% of people with end-stage kidney disease who are on dialysis. The diagnosis of Coronary artery Disease (CAD) in people with renal artery stenosis ranges from 11.3% to 39% [2].
The most widely used imaging modalities for the screening and diagnosis of renal artery stenosis are Doppler ultrasound and CT angiography [1].
We report here the case of a 65- year- old patient admitted for a hypertensive emergency such as myocardialinfarction, on a background of resistant arterial hypertension due to stenosis of the atherosclerotic left renal artery.
Case report
This is a 69 – year – old patient, hypertensive for 20 years well balanced on dual therapy, diabetic for 20 years on oral antidiabetics, admitted to our structure for a hypertensive emergency such as uncomplicated anterior myocardial in farction revealed by the installation of an anginal, retrosternal, constrictive chest pain radiating to both shoulders. The clinical examination shows a blood pressure of 195/110 with sinus tachycardia at 130 bpm with no heart murmur on auscultation or signs of left or right heartfailure.
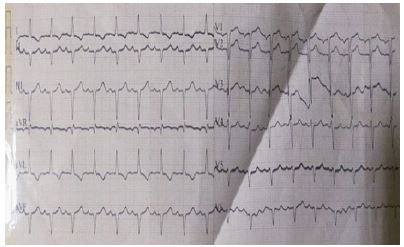
His electrocardiogram showed sinus tachycardia at 130 Bpm, ST segment elevation with an aspect of QS in the antero-septal and inferior and negative T waves in the lateral (Figure 1).
His echocardiography showed an undilated left ventricle, the site of moderate concentric ventricular hypertrophy (inter ventricular septum at 14 mm and the posterior wall at 13 mm) (Figure 2), with anterior kinetic disorders, and a fraction 50% ejection (SB), left ventricular filling pressures were non-elevated without valvulopathy or other associated signs.
The patient was quickly transported to the catheterization room, where a coronary angiography with primary angioplasty was performed.
During his stay in the hospital, an unbalanced blood pressure profile was observed, with an average blood pressure of 180 mm Hg systolic and 110 mm Hg diastolic throughout the day and during the nychthemeron, proven by a 24-hour MAP. The patient was put on full-dose triple therapy (an ACE inhibitor, a calcium channel blocker and a beta-blocker), and yets he had an unbalanced blood pressure profile. The decision for the introduction of a hydrochlorothiazide has been taken.
Blood pressure monitoring in the intensive care unit did not show any improvement in blood pressure figures.
The diagnosis of resistant hypertension was retained, for this, an assessment was carried out, namely:
A biological assessment: A correct blood count, without anemia or hyper leukocytosis, with correct renal function (Urea: 0.5 g/l; Creat: 7.8 mg/l with a GFR of 77.9 ml/min/1, 73 m²), no hydro electrolyte disorder, normal 8 a.m. cortisol level sat 12.8 μg/dl, methoxylated derivatives and the aldosterone/renin ratio without particularities.
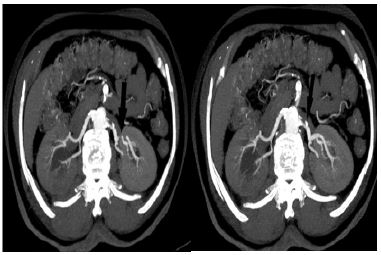
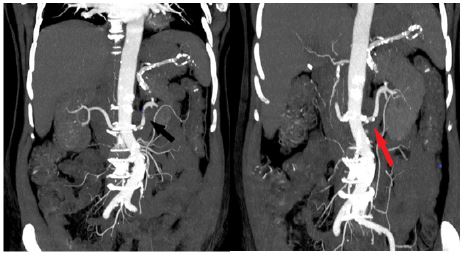
On the radio logical level, a Doppler ultrasound of the renal arteries showed bilaterally patent renal arteries, and an abdominal CT angiography objectifying a severe diffuse atheromatous overload, with a stenosing atheromatous plaque at the level of the ostial and juxta-ostial portions of the left renal artery. Estimated at 70% extending over 15 mm, and a partially calcified non-stenosing atheromatous plaque of the right renal artery secondarily reducing its caliber by 14% (Figures 3,4,5).
The diagnosis of resistant hypertension secondary to stenosis of the renal arteries of atheromatous origin revealed by an acute coronary syndrome was retained. And, after a discussion with the multi disciplinary staff, medical treatment and close monitoring were indicated.
The evolution, after 6 months of follow-up, was marked by the stabilization of the Blood Pressure Figures (BP = 135/85 mm Hg) after the introduction of an optimal anti hypertensive and anti-ischemic treatment.


Discussion
Renal artery stenosis secondary to osclerosis is the most common cause of renovascular hypertension. Often it aggravate spre-existing essential hypertension [1]. It should be suspected in all patients over 55 with resistant hypertension [3].
Its prevalence increases with age and affects 30% of patients with coronary artery disease and up to 50% of patients with peripheral arterial disease [4].
Renal artery stenosisis said to be significant with hemodynamic repercussions if the stenosisis >50%. Thus causing an imbalance of the renin-angiotensin-aldoster one system resulting in accelerated hypertension [5]. The development of stenosing atherosclerotic plaques is often found at the level of the ostia of the renal arteries [6].
From a pathophysiological point of view, and when this stenosisis very important, several mechanisms may be involved, namely: activation of the sympathetic system, inhibition of NO production, damage to the microcirculation of the kidney, renal hypoperfusion and neurohormonal changes, which lead to RAAS activation [7].
Hypertensive patients must be regularly monitored, and in the event of any suspicion of resistant hypertension, an assessment in search of RAS must be carried out. Biologically, and in first intention, the renal function and the water-electrolyte balance can direct to wards renal suffering.
And radiologically, the most common tests used to assess the presence of renal artery stenosis include Doppler ultrasound, MRI angiography and CT angiography [6].
Renal artery Doppler is usually the first-line test, as it is non-invasive, affordable, radiation-free, and can be easily used in almost all patients. It allows anatomical and functional assessment of the kidneys and arteries as well as Doppler hemodynamic study, such as measurement of blood flow velocity and pressure wave forms [7].
Prevalence of RAS identified by ultrasound Doppler in an American study ranges from 0.5% to 7% of individuals [2].
However, this examination has low sensitivity, it takes a long time, depends heavily on the operator, it is difficult to perform in obeses patients or in the event of the presence of diffuse intestinal gas, there is the risk of not visualizing or identify the accessory renal arteries [7]. But a normal exam will not rule out renal artery stenosis.
This is evident in our case, where the Doppler ultrasound of the renal arteries returned to normal, with kidneys of good size, without modification of the Doppler flow or hemodynamic repercussions down stream.
Abdominal CT angiography has a high sensitivity and specificity for detecting RAS, it allows better resolution of the renal arteries and surrounding structures in time and space, it is a rapid examination which allows better visualization of the arteries and less sensitive to motion artifacts [7].
MRI Angiois the most accurate diagnostic test, and can be used in patients with kidney failure and contrast allergy, however, it is limited due to high cost and availability.
The cardiovascular risk associated with the presence of atherosclerotic renal artery stenosis is linked to the presence of atherosclerotic plaques in other vascular sites, in the context of generalized chronicvascular disease. The most serious of these attacks is the occurrence of acute coronary syndromes and which represents the vital emergency in these patients. As is the case with our patient.
The natural course of RAS leads to progressive renal ischemia with renal a trophy, some times progressing to complete occlusion by artery thrombosis [1].
And so the care must be fast and thorough.
It focuses mainly on controlling high blood pressure, managing cardiovascular risk factors (stopping smoking, controlling diabetes, and managing over weight), and preserving kidney function, and therefore, reduce cardiovascular and renal risks. Treatment options essentially include optimal medical treatment, inter ventional or surgical revascularization [2].
Medical therapy is the main stay of treatment for atherosclerotic renal artery stenosis.
The latest recommendations from the American College Of Cardiology and American Heart Association (ACC/AHA) indicate for the treatment of arterial hypertension associated with class I renal arterystenosis: ACE inhibitors (ACE inhibitors), or Angiotensin II Receptor antagonists (ARAII), combined or not with calcium channel blockers and beta-blockers [8].
Renal artery stenosis causes a decrease in renal perfusion and therefore it activates the renin-angiotensin-aldosterone system, therefore the use of an enzyme-converting enzyme inhibitor or an angiotens in receptor antagonist reduces blood pressure effectively [6]. This was confirmed in several other studies [9].
It should be noted that medical care in this type of patient should be global, and there fore combines several drugs, namely: anti-platelet agents, statins [7].
With regard to revascularization, several studies have been carried out recently, in order to seek the clinical benefit that it brings compared to medical treatment.
The ASTRAL study, one of the main large studies in which 403 patients with renal arterystenos is received drug treatment and 403 others, drug treatment associated with angioplasty and/or a renal artery stent, followed on a duration of 27 weeks, confirmed at the end of the study, that revascularization therapy had no benefit for renal function, blood pressure, renal or car diovascular events or over all mortality compared to patients treated with optimal medical treatment. In fact, a number of patients in the trial who underwent revascularization suffered serious complications from the procedure, leading the authors to conclude that not only did revascularization have no significant benefit, but that it also involved significant risk [10].
In another cohort study of 195 patients, renal revascularization did not improve mortality, but on the other hand, the use of ACE inhibitors was associated with a decrease in long-termmortality [11].
Surgical revascularization techniques that include aorto-renal bypass, extra-anatomic bypasses, unilateral nephrectomy, extra corporeal microvascular reconstruction, end arterectomy and atherectomy [7] provide no benefit over medical treatment or percutaneous revascularization [7,12].
Conclusion
Our case illustrates resistant arterial hypertension on a background of essential hypertension revealed by an myocardial infraction, in which echodoppler of the renal arteries which is considered to be the most commonly used screening test was falsely negative, but an abdominal CT angiography revealing a renal arterystenosis. The latter should be systematically sought in patients over 55 with secondary hypertension or hypertension resistant to the usual antihypertensive treatment.
Early detection of renal arterystenosis makes it possible to maintain an effective therapeutic strategy, thus avoiding deterioration of renal function and progression to chronic kidney disease as well as the occurrence of cardiovascular events.
References
- Vipparla N, et al. Resistant Hypertension Secondary to Severe Renal Artery Stenosis With Negative Duplex Ultrasound: A Brief Review of Different Diagnostic Modalities. J Investig Med High Impact Case Rep. 2020; 8: 2324709620914793.
- Renal Artery Stenosis in the Patient with Hypertension: Prevalence, Impact and Management. Rohini Manaktala Jose D Tafur-Soto Christopher J White Ochsner Clinic Foundation, Department of Cardiovascular Medicine, New Orleans, LA, USA. Integrated Blood Pressure Control. 2020: 13 : 71–82.
- Alyamani M, Thomas J, Shanks M, Oudit GY, et al. Resistant Hypertension From Renal Artery Stenosis Leading to Heart Failure With Preserved Ejection Fraction. J Investig Med High Impact Case Rep. 2018; 6: 2324709618816501
- Harding MB, Smith LR, Himmelstein SI, et al. Renal artery stenosis: Prevalence and associate drisk factors in patients under going routine cardiac catheterization. J Am Soc Néphrol. 1992; 2: 1608-1616.
- Renal Disease and Renal Artery Stenosis in the Elderly. Donald G Vidt. American Journal of Hypertension. 1998; 11: 46S–51S.
- Renal artery stenosis. Saifan RD, Textor SC. N Engl J Med. 2001; 344 :431-442.
- Chirag Bavishi, MD, et al. Atherosclerotic Renal Artery Stenosis and Hypertension: Pragmatism, Pitfalls, and Perspectives. The American Journal of Medicine. 2016; 129: 635. e5-635. e14
- Practice Guidelines for the management of patients with peripheralarterial disease (lower extremity, renal, mesenteric, and abdominal aortic): Collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; Trans Atlantic Inter-Society Consensus; and Vascular Disease Foundation. Hirsch AT, Haskal ZJ, Hertzer NR, ACC/AHA 2005. Circulation. 2006; 113: e463-e654.
- Schwietzer G, Oelkers W. Klin Wochenschr. The antihypertensive effect of captopril in severe essential, renovascular, renal and transplant renovascular hypertension. 1982; 60: 839-846.
- Wheatley K, Ives N, N Engl J Med. Revascularization versus medical therapy for renal-arterystenosis. ASTRAL Investigators; 2009; 361: 1953-1962.
- Losito A, Errico R, Santirosi P, Lupattelli T, Scalera GB, et al. Long-term follow-up of ather oscleroticrenovascular disease. Beneficial effect of ACE inhibition. Dial Transplant. 2005; 20: 1604-1609.
- Balzer KM, Pfeiffer T, Rossbach S, J. Vasc. Prospective randomized trial of operative vs interventional treatment for Renal Artery Ostial Occlusive Disease (RAOOD). Surg. 2009; 49: 667-674.