
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Paucisymptomatic pulmonary tuberculosis in an immunocompetent young patient
Hugo Inácio1*; Leonor Soares2; Paulo Barreto1
1Hospital de Santo António dos Capuchos, Centro Hospitalar Universitário de Lisboa Central, Portugal.
2Hospital de São José, Centro Hospitalar Universitário de Lisboa Central, Portugal.
*Corresponding Author : Hugo Inácio
Hospital de Santo António dos Capuchos, Centro Hospitalar Universitário de Lisboa Central.
Phone: +351 964650329;
Email: hinacio@gmail.com
Received : Nov 30, 2022
Accepted : Dec 07, 2022
Published : Dec 14, 2022
Archived : www.jcimcr.org
Copyright : © Inácio H (2022).
Keywords: Pulmonary tuberculosis; Paucisymptomatic; Immunocompetent.
Citation: Inácio H, Soares L, Barreto P. Paucisymptomatic pulmonary tuberculosis in an immunocompetent young patient. J Clin Images Med Case Rep. 2022; 3(12): 2199.
Background
This report presents the case of a 20-year-old student girl with no medical history, no usual medications, no known allergies and living in a clean and sanitary environment. The patient was referred to the Emergency Department (ED) with a four week history of non-productive cough associated with right-sided back pain. She denied fever, dyspnea, night sweats, anorexia, or involuntary weight loss.
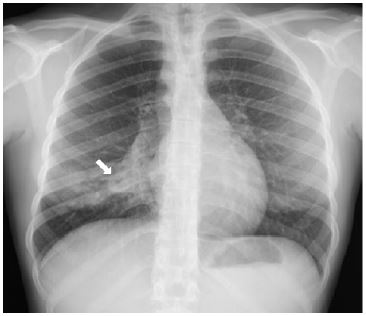
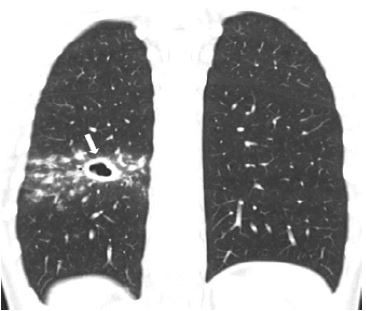
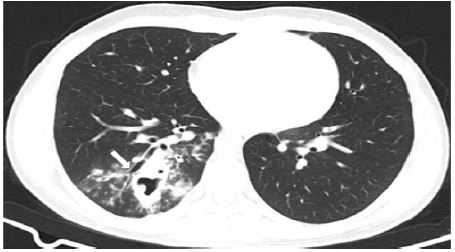
Upon presentation to the ED, both the physical examination and the blood analysis were unremarkable, but the chest X-ray showed a Right Lower Lobe (RLL) infiltrate, with a well-defined nodule measuring less than 2 cm in diameter (Figure 1). In order to clarify the image, a chest Computed Tomography (CT) scan was performed, which revealed densification of the lung parenchyma in the RLL, with a cavitated image of about 14 mm (Figures 2 and 3); no mediastinal, hilar, or axillary adenopathies were noted.
Although the cough was mostly non-productive, an acid-fast smear was performed on two consecutive samples, and it was negative for mycobacteria. A bronchofibroscopy was then performed, but the acid-fast smear from the bronchoalveolar lavage was negative for mycobacteria too. However, the nucleic acid amplification test confirmed Mycobacterium Tuberculosis complex (MT), with negative resistance to rifampicin.
Although pulmonary tuberculosis can manifest in several ways, its early symptoms are often minimal and may be mistaken for other causes. Given this report, it is important to remember that lingering symptoms should always be investigated, that tuberculosis can present in a variety of ways and it can also affect immunocompetent individuals.
References
- A Campbell and O Bah-Sow. Pulmonary tuberculosis: Diagnosis and treatment, British Medical Journal. BMJ Publishing Group. 2006; 332: 1194–1197.
- S Ates Guler, et al. Evaluation of pulmonary and extrapulmonary tuberculosis in immunocompetent adults: A retrospective case series analysis Medical Principles and Practice. 2015; 24: 75–79.
- SM Lyon and MD Rossman. Pulmonary Tuberculosis, Microbiol Spectr. 2017; 5.