
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Extreme hypernatremia exceeding the reportable value
of the blood gas analyzer in a 64-year-old female
Abdalla Khalil1*; Laiba Khalid1; Khalil Hossenbux2
1Department of Acute Medicine, Northwick Park Hospital, London Northwest London University Healthcare, UK.
2Department of Acute Medicine, Princess Royal University Hospital, Kings College trust, London, UK.
*Corresponding Author : Abdalla Khalil
Department of Acute Medicine, Northwick Park Hospital, London Northwest London University Healthcare, UK.
Phone: 0044-7460707538
Email: abdallak59@gmail.com
ORCID: 0000-0001-6853-0284
Received : Nov 20, 2022
Accepted : Dec 09, 2022
Published : Dec 16, 2022
Archived : www.jcimcr.org
Copyright : © Khalil A (2022).
Abstract
ypernatremia is a relatively common electrolyte imbalance in hospitalized patients and is considered an independent predictor for increased mortality. Concomitant sepsis and thromboembolism are also common with severe hypernatremia and management of the fluid therapy is a challenging issue. A 68-year-old female was admitted to our hospital with extreme hypernatremia (above the reportable value of the blood gas analyzer), a significant decrease in her level of consciousness, acute kidney injury, sepsis, hypoxemia, and a suspected pulmonary embolism. She was managed in the acute medical ward with full recovery of her level of consciousness, renal function, and baseline mobility. Her serum sodium was normalized, and pulmonary embolus was excluded. She was discharged home after 12 days with a home review and renal function monitoring.
Keywords: Hypernatremia; Community acquired; Hospital acquired; Management; Outcome.
Citation: Khalil A, Khalid L, Hossenbux K, et al. Extreme hypernatremia exceeding the reportable value of the blood gas analyzer in a 64-year-old female. J Clin Images Med Case Rep. 2022; 3(12): 2203.
Introduction
Hypernatremia is a relatively common electrolyte disturbance in hospitalized patients.
The prevalence of hypernatremia in hospitalized patients has been reported as being between 1% and 4% [1,2].
The severity of community-acquired hypernatremia is an independent predictor of mortality in hospitalized patients and can be associated with sepsis and thromboembolic disorders [3,14,15].
Case presentation
A 68-year-old female presented to the ED with poor oral intake and generalized weakness for two weeks.
She used to walk for a short distance around 100 meters with support, but she became bed bounded, sleepy and less responsive during the last two weeks.
Her home carer noted that her urine was dark and smelly.
She was living in the United Arab Emirates for the last 6 months and arrived in the UK three weeks before the presentation.
Her past medical history includes a stroke in 2008 without a residual neurological deficit, essential hypertension, and depression and recently was diagnosed with Parkinson’s disease and dementia. Her current medications were Madopar, Rivastgmin, clopidogrel, and venlafaxine.
On arrival to the ED Emergency Department, her heart rate was 110/min, BP was 108/50 mmhg, oxygen saturation was 88% in room air, respiratory rate was 24/min, and temperature was 38.2oC.
She was dehydrated with dry mucous membranes and loss of the skin turgor.
She was sleepy but arousable. Her Glasgow Coma Scale GCS was 10/15 (opened eyes on response to pain 2, localized pain 5, and answered with in appropriate words 3).
Patient did not have facial asymmetry, no localization signs, her tendon jerks were normal, and her plantar reflex was flexor. She was not cooperative for the rest of neurological examination, and the rest of her clinical examination was unremarkable.
The venous blood gases revealed a high sodium level which was above the reportable range of sodium by the blood gas analyzer (the maximum reportable value of sodium in the blood gas analyzer was 190 mmol/L) (Figure 1).
Her serum chemistry confirmed a serum sodium level of 193 mmol/L with high urea, creatinine, C reactive protein, and D dimer (Table 1).
Liver function tests, coagulation screen, and respiratory viral screen including SARS CoV -2 RNA were normal.
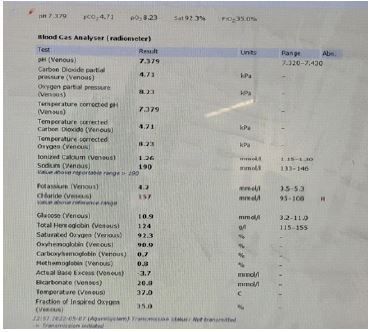
Table 1: The course of endoscopic treatments.
| Investigation | Result in ED | Normal range |
|---|---|---|
| WBC Neutrophils Platelets PCV HB MCV Neutrophils Lymphocytes |
10.9 X 109/L 9.4 X 109/L 187 X 109/L 0.49 145 g/L 98.7 fL 10.7 X109/L 1.3 x109/L |
3.4 -10 X 109/L 2.0 – 7.5 X 109/L 150-400 X 109/L 0.33 – 0.45 115-155 g/L 80-99 fL 2.0-7.5 X 109/L 1.5-4.0 X 109/L |
| Sodium Potassium Urea Creatinine Calcium Phosphate |
193 mmol/L 4.2 mmol/L 37.9 mmol/L 276 umol/L 2.49 mmol/L 1.51 mmol/L |
133-146 mmol/L 3.5-5.3 mmol/L 2.5-7.5 mmol/L 44-88 umol/L 2.15-2.55 mmol/L 0.80 – 1.50 mmol/L |
| Magnesium Serum osmolality |
1.48 mmol/L 435 mOsm/kg |
0.70- 1.00 mmol/L 275 to 295 mOsm/kg |
| CRP | 123 mg/L | 0.0-5.0 mg/L |
| D dimer | 34.800 ug/L | 0.0-500 ug/L |
| Troponin | 158 ng/L | 0-14 ng/L |
| LDH | 334 IU/L | 135-214 IU/L |
Her electrocardiogram ECG showed normal sinus rhythm with a rate of 102/min and deep T wave inversion in the infero-lateral leads. The repeated ECG showed the same findings and repeated troponin was trending down.
The chest x-ray and computerized tomography CT head were unremarkable.
Our provisional diagnoses were severe hypernatremia with severe dehydration, acute kidney injury, sepsis (urosepsis and suspected aspiration pneumonitis), a suspected pulmonary embolism (bed bounded, hypoxemia, and a high D dimer), and a decrease level of consciousness was most probably secondary to the previous diagnoses.
Septic screens (blood, urine and respiratory cultures) were sent to the laboratory.
She received the first litre of IV 0.9% sodium chloride over 6 hours and piperacillin/tazobactam IV adjusted dose according to estimated glomerular filtration rate eGFR. She was prescribed a therapeutic dose of dalteparin subcutaneously to cover the possibility of pulmonary embolism.
A plan for a CT pulmonary angiography was considered after improving the GFR with IV fluids therapy during the next few days.
Her calculated free water deficit (with target sodium 145 mmol/l) was 7.4 litres.
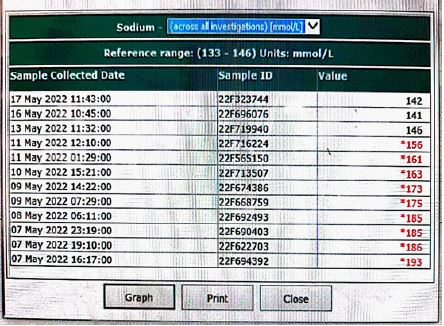
She received IV 0.45% sodium chloride slow infusion then 0.9 % sodium chloride alternate with Dextrose 5% and the rate of infusion was adjusted according to close monitoring of the serum sodium level. Daily levels of serum sodium were shown in a graphic curve and schedule (Figure 2) and (Figure 3).
The patient’s clinical condition gradually improved. Her tachycardia resolved, her oxygen requirement declined, and her renal function improved.
The CT pulmonary angiography could be performed on the 4th day after admission and did not show any pulmonary embolism.
Her serum sodium level was trending down daily within the acceptable target rate of decent (not more than 10 mmol/L over 24 hours), and her level of consciousness gradually improved.

She became more alert with coherent speech, and she could recognise her son and the care giver but was confused. On the 7th day after admission, her GCS became 14/15 and was nearly back to her baseline cognition (according to her son).
She was reviewed by both physiotherapist and the dietician and both family members and caregiver were taught about ensuring daily fluid intake to maintain hydration and type of fluid.
She could manage to walk again with support as her baseline before the illness.
On the 12th day after admission, she was discharged home with an arrangement for a home visit to review and repeat her renal function test at home.
Discussion
In a large population-based study in the USA (1.9 million patients during the period 2000 to 2018), 3% of all hospitalized patients have serum sodiumof more than 145 mmol/L. the incidence of in-hospital mortality was 12% in the hypernatremic patients and 2% in the normonatremic patients. Patients with serum sodium of more than 155 mmol/L have in-hospital mortality of 34.4% [4].
Hypernatremia is more common in elderly patients and pediatrics [5,6].
Elderly patients have decreased thirst sensation and their renal ability to dilute and concentrate urine is less than younger patients which makes them more susceptible to hypernatremia [5].
Hospital-acquired hypernatremia is more common than community-acquired hypernatremia.
In a study in the Netherlands during the period 1992 to 2012, hypernatremia in ICU patients was mainly hospital-acquired hypernatremia, and incidence increased during the period of the study from 13% to 24%. The mortality rate in patients with hypernatremia correlates with the severity of hypernatremia reaching up to 56% in patients with serum sodium more than 160 mmol/L [7].
Hospitalized patients with traumatic brain injury have the highest incidence of hypernatraemia (16%-40% of traumatic head injury patients) [8].
Hypernatremia from free water loss is more common than hypernatremia associated with excessive sodium intake [9]. Manifestations of severe hypernatremia include stupor, seizures, intracranial hemorrhage, coma, and death [10].
Blood gas analyzer has a high correlation with laboratory analyzer measurement of sodium level, but in hypernatremiamainly in acidosis and pulmonary disease discrepancy with laboratory analyzer increases [11]. In our case presentation, there was no acidosis or pulmonary disease, but the level of sodium was above the reportable value of sodium by the blood gas analyzer (it was above 190 mmol/L).
In calculating the water deficit for chronic hypernatremia, target sodium used was 145 mmol/L which was the target level we used in calculating the water deficient in our patient.
The rate of correction of serum sodium in hypernatremic patients is a challenging issue.
In patients with severe symptoms i.e. neurological symptoms, serum sodium should be lowered by 2 mmol/hour in the first 2-3 hours, then followed by a correction rate of 0.5 mmol/L/hour [10]. The target is to lower serum sodium by10 mmol/L/day in these patients if possible [13].
We tried to achieve this target during our correction of the patient’s hypernatraemia with close monitoring of serum sodium level as per guidelines and changing the rate of fluid accordingly.
In a study in the USA involving both community-acquired and hospital-acquired severe hypernatraemia patients, there was no evidence that rapid correction (more than 0.5 mmol/L/hour) was associated with higher mortality rate, seizures, altered level of consciousness, or cerebral oedema) [13].
Association between hypernatraemia and sepsis in the elderly was noted in a study in the USA (more than 77% of 153 patients) [14]. Sepsis was one of our suspected diagnoses and an empirical antibiotic was initiated after taking a septic screen.
Thromboembolic risk is also increased with hypernatraemia and hyperosmolarity [15].
Our patient was hypoxaemic on admission, and her chest x-ray was normal with a very high dimer, immobility, and a high Wells’ score for pulmonary embolism. A therapeutic dose of low molecular weight heparin was started, and CT pulmonary angiography (after improvement of the renal function) excluded a pulmonary embolism.
Conclusion
Severe hypernatremia is an independent predictor for mortality of hospitalized patients and a higher level of serum sodium correlates with a higher mortality rates. Hypernatremia in hospitalized patients is associated with sepsis and thromboembolic disease.
Fluid therapy for hospitalized patients with severe hypernatremia is still a challenging issue and close monitoring of serum sodium is essential to achieve a good outcome.
References
- Liamis G, Filippatos TD, Elisaf MS. Evaluation and treatment of hypernatremia: A practical guide for physicians. Postgrad Med. 2016; 128: 299-306.
- Lombardi G, Ferraro PM, Calvaruso L, Naticchia A, D’Alonzo S, Gambaro G, et al. Sodium Fluctuations and Mortality in a General Hospitalized Population. Kidney Blood Press Res. 2019; 44: 604-614.
- Cabassi A, Tedeschi S. Severity of community acquired hypernatremia is an independent predictor of mortality: A matter of water balance and rate of correction. Intern Emerg Med. 2017; 12: 909-911.
- Arzhan S, Roumelioti ME, Litvinovich I, Bologa CG, Myers OB, et al. Hypernatremia in Hospitalized Patients: A Large Population-Based Study. Kidney. 360. 2022; 3: 1144-1157.
- Mahowald JM, Himmelstein DU. Hypernatremia in the elderly: Relation to infection and mortality. J Am Geriatr Soc. 1981; 29: 177-180.
- Martínez RM, Viñas T, Manrique G, López Herce J. Hyperchloremia and hypernatremia in critically ill children. Med Intensiva (Engl Ed). 2021; 45: e59-e61.
- Oude Lansink-Hartgring A, Hessels L, Weigel J, de Smet AMGA, Gommers D, et al. Long-term changes in dysnatremia incidence in the ICU: A shift from hyponatremia to hypernatremia. Ann Intensive Care. 2016; 6: 22.
- Kolmodin L, Sekhon MS, Henderson WR, Turgeon AF, Griesdale DE, et al. Hypernatremia in patients with severe traumatic brain injury: A systematic review. Ann Intensive Care. 2013; 3: 35.
- Cassorla FG, Gill JR Jr, Gold PW, et al. Nosocomial hypernatremia. N Engl J Med. 1985; 313: 329.
- Sterns RH. Disorders of plasma sodium-causes, consequences, and correction. N Engl J Med. 2015; 372: 55-65.
- Zamanabadi MN, Zamanabadi TN, Alizadeh R. Measuring serum sodium levels using blood gas analyzer and auto analyzer in heart and lung disease patients: A cross-sectional study. Ann Med Surg (Lond). 2022; 78: 103713.
- Al-Absi A, Gosmanova EO, Wall BM. A clinical approach to the treatment of chronic hypernatremia. Am J Kidney Dis. 2012; 60: 1032-1038.
- Chauhan K, Pattharanitima P, Patel N, Duffy A, Saha A, Chaudhary K, et al. Rate of Correction of Hypernatremia and Health Outcomes in Critically Ill Patients. Clin J Am Soc Nephrol. 2019; 14: 656-663.
- De Freitas G, Gudur A, Vela Ortiz M, Jodelka J, Livert D, et al. Krishnamurthy M. Where there is sodium there may be sepsis. J Community Hosp Intern Med Perspect. 2019; 9: 296-299.
- Grant PJ, Tate GM, Hughes JR, Davies JA, Prentice CR, et al. Does hypernatraemia promote thrombosis? Thromb Res. 1985; 40: 393-399.