
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Cerebral arterial air embolism after bag-valve-mask ventilation
Evren Senturk; Merve Umran Yilmaz*; Gulay Kir; Nahit Cakar
Koc University Hospital, Koç University School of Medicine, Turkey.
*Corresponding Author : Merve Umran Yilmaz
Koc University Hospital, Koç University School of Medicine, Turkey.
Email: merveumranyilmaz@gmail.com
Received : Nov 16, 2022
Accepted : Dec 12, 2022
Published : Dec 19, 2022
Archived : www.jcimcr.org
Copyright : © Yilmaz MU (2022).
Abstract
Cerebral Arterial Gas Embolism (CAGE) is a serious condition, which tends to occur as an iatrogenic complication of numerous invasive medical and surgical procedures performed in an esthesia and intensive care. Although air embolism due to right-to-left shunt is a well- known concept, positive pressure ventilation related arterial embolism is a frequently overlooked mechanism.
This case report represents two patients with cerebral arterial air embolism after bag- valve-mask ventilation. Both patients had tracheostomies because of their preexisting lung diseases. Bag-valve-mask ventilation was made through tracheostomy tubes after a brief desaturation period. Following positive pressure ventilation, both patients became unresponsive. Computed tomography images demonstrated air bubbles within multiple arterial regions which could explain patients’ rapid clinical decline with loss of consciousness and hemodynamic collapse. ECHO was performed in both cases but failed to demonstrate any intracardiac right-to-left shunt. Patients’ neurological condition did not improve and one of them died due to refractory sepsis related multiple organ failure.
We assume positive pressure related barotrauma can lead to not only venous air emboli but also arterial air embolism especially in patients with predisposing lung injuries. This case report aims to bring awareness to this rare complication of positive- pressure-ventilation. Sudden on set of neurological deficits in this patient population should initiate a workup for exploring the possibility of CAGE.
Keywords: Arterial air embolism; Cerebral air embolism; Tracheostomy; Bag-valve ventilation; Positive pressure related barotrauma; ARDS; COVID-19.
Citation: Sentur E, Yilmaz MU, Kir G, Cakar N. Cerebral arterial air embolism after bag-valve-mask ventilation. J Clin Images Med Case Rep. 2022; 3(12): 2204.
Introduction
Cerebral Arterial Gas Embolism (CAGE) is a serious condition, which occurs as a complication of numerous invasive medical and surgical procedures performed in anesthesia or intensive care [1]. CAGE usually presents with stroke-like manifestations, sudden onset neurologic deficits and altered mental status.
Here, we report two nonoperative patients with cerebral arterial air embolism who had CAGE after bag-valve ventilation from tracheostomies due to hypoxia.
Patient 1
An eighty-year-old tracheostomized male patient with a history of coronary arterial bypass grafting due to ischemic heart disease, paroxysmal atrial fibrillation, dilated cardiomyopathy, and severe Chronic Obstructive Pulmonary Disease (COPD) was hospitalized due to refractory decubitusulcers. The patient was being treated with antibiotics due to bacterial infection of his ulcers. On his 26th day of hospitalization, when he was awake and breathing room air, he started vomiting. He subsequently lost consciousness following a sudden decrease in oxygen satura tion level to 85%. He was unresponsive to painful stimuli and his pupillary reflexes were absent. Immediately, tracheal aspiration was performed without any removal of gastric contents. Bag Valve (BV) ventilation was initiated through his tracheostomy tube. Oxygen saturation returned to normal range but his unconscious state did not improve. Cranial and thoracic Computed Tomography (CT) scans were obtained, revealing the presence of air bubbles within the cerebral vasculature of the right frontal subarachnoid space. Additionally, thoracic CT showed interstitial edema and centrilobular emphysema. An Echocardiography (ECHO) was obtained which revealed neither any intracardiac pathologies nor right-to-left shunt. Ejection fraction was 43%, similar to his previous ECHOs. His pulmonary artery systolic pressure (PASP) was elevated to 70 mmHg, which was measured as 43 mmHg previously. He did not have any central lines inplace throughout his time in the hospital. An abdominal CT angiography was ordered due to the air images in the liver observed in his thoracic CT. His abdominal CT angiography revealed air in the hepaticportal venous system and the proximal jejunal wall, which was consistent with acute mesenteric ischemia. While he was in the CT imaging room, his blood pressure and saturation dropped to 80/50 mmHg and 90%, respectively. He transferred to our Intensive Care Unit (ICU). When the patient was admitted to the ICU, his Glasgow Coma Scale (GCS) was 4 (Eye: 2 Verbal: 1 Motor: 1), his pupils were non-reactive and he was unresponsive. His APACHE II score was 25. He was put on mechanical ventilation in pressure support mode with Post End Expiratory Pressure (PEEP) of 6 cm H2O and pressure support above PEEP of 14 cm H2O at Fraction of Inspired Oxygen (FiO2) of 40%. An Internal Jugular Vein (IJV) catheter was placed in the ICU. Blood, urine and Endotracheal Aspirate (ETA) culture samples were collected. His antibiotic regimen remained the same. Neurosurgery and general surgery were consulted. Both suggested surgical interventions, which were refused by the patient’s family. In the ICU, the patient remained stable, did not require vasopressor support, but his mental status did not improve. His cranial magnetic resonance imaging was obtained on the 5th day after the incidence, revealed sub acute ischemia in the arterial supply regions. After six days in the ICU, the patient was transferred back to the general ward. After twenty more days in the hospital due to his treatment of decubitus ulcers, he was discharged from the hospital without any improvements in his mental state.


Patient 2
A fifty-eight-year-old male patient without any known disease history was admitted to the hospital due to shortness of breath. A week prior to his admittance, the patient was diagnosed with COVID-19. On the 4th day in the COVID ward, he was transferred to the ICU due to severe hypoxemia. He was fully awake and cooperative. His APACHE II score was 13. Noninvasive mechanical ventilation support was initiated. His therapy included an antiviral agent, prednisolone and anti coagulation. His condition deteriorated and he was placed on invasive mechanical ventilation. Antibiotic therapy was started for ventilator associated pneumonia. He required high fraction of inspired oxygen and ventilatory support because of his lung fibrosis. He developed mediastinal subcutaneous emphysema which did not require any drainage. He was finally tracheostomized on his 28th day in the ICU. After 60 days in the ICU, he was transferred to the ward on an home ventilator. At the time of transfer the patient was tracheostomized, fully awake, and oriented. On the 7th day in the ward, his saturation abruptly dropped to 74% and he became hypotensive. Tracheal aspiration was unrevealing and he was ventilated by BVM with 100% oxygen. His pupils were not reactive to light and anisocoria was noted. His GCS was 3. He was immediately transferred to the ICU and vasopressor support was initiated. When the patient became hemodynamically stable, CT images of the brain and chest were obtained. Cranial CT revealed air bubbles within the cerebral vasculature of the right frontal subarachnoid space and also in between cervical muscle planes. Thoracic CT demonstrated pneumomediastinum, interstitial emphysema, and signs consistent with acute respiratory distress syndrome all worsened compared to his previous thoracic CT scans, and new onset bilateral Pneu-moThorax (PTX). His old IJV catheter -which was placed a week before was occluded so a new central venous catheter was placed after his CT scans. Bilateral thoracostomy tubes were inserted for the treatment of his PTX. His ECHO, which was done one day prior to the incident did not show any structural abnormalities in the heart, or intracardiac shunts. Only distinguishable point was pulmonary arterial hypertension (PASP: 42 mmHg). During his ICU stay, his status did not improved, his vasopressor requirement escalated. On his 8th day in the ICU, he died due to refractory septic shock and respiratory distress.
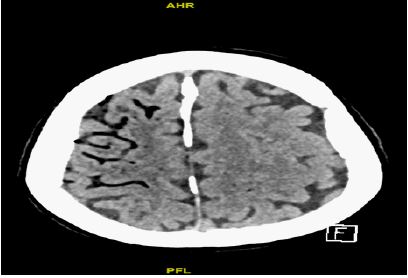

Table 1:
| Patient 1 | Patient 2 | |
|---|---|---|
| Predisposing lung condition | Severe COPD | Covid-19 pneumonia |
| Tracheostomized | Yes | Yes |
| PASP | 70 mmhg | 42 mmhg |
| Intracardiac right- to-left shunt existence | No | No |
| Glasgow coma scale (before /after) | 15/4 | 15/3 |
Discussion
Arterial gas embolism is a rare, life-threatening condition that needs early detection and rapid intervention. Infarciton in the effected arterial supply regions together with presence of air bubbles within the arteries should also raise awareness about arterial air embolism. The consequences of arterial gas embolism can be devastating. Patients can rapidly deteriorate from stable hemodynamics to total cardiovascular collapse.
Cerebral arterial air embolism is a relatively common problem in scuba divers. There are numerous case reports aimed to address this problem in the field of hyperbaric medicine. Scuba regulators deliver breathing gas to the diver at ambient pressure and, if divers don’t exhale sufficiently during ascent, gas inspired at depth will expand. This expansion over-distends the lungs leading to Pulmonary Barotrauma (PBT).
Iatrogenic arterial air embolism may result from the entry of gas during vascular cannulation procedures or PBT during mechanical ventilation in children and less commonly in adults. Simultaneous damage to respiratory and vascular tissues may lead to CAGE as a result of the gas passing from ruptured alveoli into the pulmonary veins and distributed into the systemic circulation [2]. PBT is likely to occur in patients with predisposing pulmonary disease [3]. Although, barotrauma related to positive pressure ventilation is a frequently seen phenomenon, its relation to arterial air embolism is uncommon [4-6].
Paradoxical Air Embolism (PAE) which is defined as venous gas embolism entering the arterial circulation via a right-to-left intracardiac shunt, such as an atrial septal defect or patent foramen ovale [2]. When intracardiac shunting cannot be demonstrated through cardiac imaging studies, the suggested underlying mechanism for PAE is transpulmonary passage. It is speculated that the transpulmonary air transport pathways (i.e. anatomic shunts) become functionally open in situations where pulmonary artery pressure becomes significantly elevated [8]. Presence of pulmonary arteriovenous malformations or inducible large diameter intrapulmonary arteriovenous an astomoses in otherwise healthy individuals is another explanation for PAE. These inducible large diameter intrapulmonary arteriovenous anastomoses are thought to be closed at rest but can open during hyperdynamic conditions. Arterial hypoxemia is found to reduce the filtering ability of the pulmonary microvasculature [9].
There are several case reports of CAGE observed after CPR. It is speculated that chest compressions cause the rupture of pulmonary vessels in conjunction with parenchymal destruction of the lung, enabling air to enter the pulmonary veins and reach the systemic circulation [10].
Both of our patients had predisposing lung conditions. After a period of desaturation, they were ventilated BVM through their tracheostomy tubes. We speculate that excessive use of BVM may have led to excessive positive airway pressure that lead to barotrauma since their lung parenchyma were already damaged. This barotrauma possibly resulted in air embolism as they did not have any demonstrable intracardiac shunt mechanisms.
Conclusion
We would like to emphasize the importance of arterial gas embolism in ICU patients considering many of them are mechanically ventilated due to their predisposing lung diseases. Cerebral arterial gas embolism should be considered when sudden onset of neurological symptoms and loss of consciousness occur in this patient population. Additionally, patients with lung diseases should be treated with caution when additional positive pressure ventilation is needed.
Acknowledgements: We would like to thank Dr. Avi Nahum for his guidance on this case report.
References
- Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000; 342: 476-482.
- Banham ND, Lippmann J. Fatal air embolism in a breath-hold diver. Diving Hyperb Med. 2019; 49: 304-305.
- Rivalland G, Mitchell SJ, van Schalkwyk JM. Pulmonary barotrauma and cerebral arterial gas embolism dur-ing hyperbaric oxygen therapy. Aviat Space Environ Med. 2010; 81: 888-890.
- Weaver LK, Morris A. Venous and arterial gas embolism associated with positive pressure ventilation. Chest. 1998; 113: 1132-1134.
- Gursoy S, Duger C, Kaygusuz K, Ozdemir Kol I, et al. Cerebral arterial air embolism associated with mechani-cal ventilation and deep tracheal aspiration. Case Rep Pulmonol. 2012; 2012: 416360.
- Mishra R, Reddy P, Khaja M. Fatal Cerebral Air Embolism: A Case Series and Literature Review. Case Rep Crit Care. 2016; 2016: 3425321.
- Moon RE. Bubbles in the brain: what to do for arterial gas embolism?. Crit Care Med. 2005; 33: 909-910.
- Bedell EA, Berge KH, Losasso TJ. Paradoxic air embolism during venous air embolism: Transesophageal echocardiographic evidence of transpulmonary air passage. Anesthesiology. 1994; 80: 947-950.
- Lovering AT, Elliott JE, Beasley KM, Laurie SS. Pulmonary pathways and mechanisms regulating transpul-monary shunting into the general circulation: an update. Injury. 2010; 41: S16-S23.
- Hashimoto Y, Yamaki T, Sakakibara T, Matsui J and Matsui M, et al. Cerebral air embolism caused by car-diopulmonary resuscitation after cardiopulmonary arrest on arrival. J Trauma. 2000; 48: 975-977.