
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?
Lena Marinova1* Radoslav Georgiev 2 Nikolay Evgeniev 3
1Complex
2UMHAT
3Complex
*Corresponding Author : Lena Marinova
Microbial Biotechnology Department, National Research Centre, Cairo, Egypt
Email: rad_marinova@abv.bg
Received : Dec 15, 2020
Accepted : Dec 30, 2020
Published : Dec 31, 2020
Archived : www.jcimcr.org
Copyright : © Marinova (2022).
Abstract
Chordoma
Keywords: Chordoma, MRI, pathomorphology, immunohistochemical analysis, early diagnosis, surgery, radiotherapy, complex treatment.
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Introduction
Seizures during pregnancy affect less than 1% of all gestations. However, it can adversely affect both maternal and fetal outcome in acute and chronic form [1]. New onset seizures in pregnancy are usually a complication of eclampsia; but women can develop new onset epileptic seizures in pregnancy. Also, structural and metabolic causes can trigger new onset of seizures in pregnancy [2]. The structural causes include intracranial haemorrhage, cerebrovascular venous thrombosis, ischemic stroke and tuberculoma. Hyperemesis gravidarum, metabolic diseases such as acute intermittent porphyria and infections are the various metabolic causes of seizures in pregnancy [3].
Tuberculoma as a reason for seizures in pregnancy is particularly rare; since only 5-10% of cases of Tuberculosis (TB) involve intracranial elements as meningitis or tuberculoma and it has to be differentiated from toxaemia and neoplastic lesions [4]. Intracerebral tuberculomas usually present as ring enhancing lesions in Magnetic Resonance Imaging (MRI). It develops by haematogenous spread of bacilli into the brain [5]. Differential diagnosis should be clearly in mind as determining the etiology is crucial for managing these patients. Evaluation and management should be done in a step-wise manner and should be a multidisciplinary approach including neurology [1]. We are reporting a case of pregnant women with new onset of seizures, thought to be due to lacunar infarct, but turned out to be a tuberculoma.
Case presentation
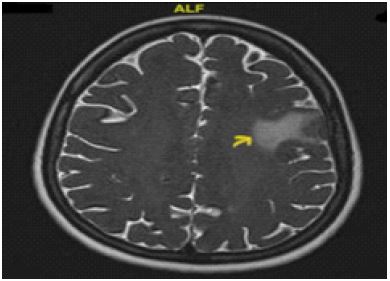
A 32 years Primigravida from Tamilnadu, India presented to JIPMER, India, at 37 weeks of gestation, with prelabour rupture of membranes. Her antenatal period was uneventful till 3 weeks earlier, when she developed 2 episodes of tonic clonic convulsions with loss of consciousness. She was not a known case of epilepsy or any evidence of hypertensive disorders of pregnancy. Her blood pressure was normal at the time of convulsion. As a part of evaluation of new onset seizures in pregnancy, plain MRI was taken. MRI brain showed a 2.5 x 1.8 cm lacunar infarct in left parietal lobe as in Figure 1. She was given intravenous Lorazepam and Phosphenytoin as initial management. Young stroke was suspected and workup was done for the same. Echocardiography heart, fundus examination, carotid artery doppler, MRI venogram brain and Electroencephalogram (EEG) were normal. She was started on Clobazam, Clopidogral and Atorvastatin.
She underwent induction of labour for prelabour rupture of membranes and delivered a healthy female baby of 2.4 kg vaginally without any complications.
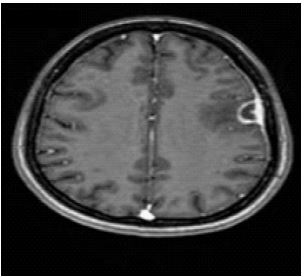
Detailed evaluation was done postnatally. A Computed Tomogram (CT) brain showed a ring enhancing lesion in frontal lobe. A repeat MRI brain also showed few ring enhancing lesions on left frontal lobe at different levels with perilesional oedema (Figure 2) and also MRI spectroscopy showed lipid/lactate peak (Figure 3), suggestive of tuberculoma. On probing, she gave history of cough with fever lasting for 1 week 3 months before the onset of seizures. Chest radiograph showed right side mild pleural effusion with basal consolidation. But sputum AFB, Mantoux and pleural fluid study were negative for any pulmonary involvement. She was started on anti-tubercular drugs and was planned for 9 months treatment. Her baby was given Isoniazid prophylaxis. She was followed up after 6months. There was no further episode of seizures, but she missed the follow up MRI brain for assessing the lesion response to treatment.

Discussion and conclusion
Tuberculosis (TB) is an airborne disease caused by Mycobacterium tuberculosis, which predominantly affects the poverty-striken populations groups from low and middle-income countries. TB is the leading cause of death from a single infectious agent and is among the top 10 causes of death. Another concern is of Multidrug-Resistant TB (MDR TB), which remains as a public health crisis and health security threat. TB is primarily a pulmonary disease, even though it can present as extra pulmonary TB simultaneously or individually [6]. In pregnancy, the T-helper 1 (Th1) proinflammatory response is suppressed, which increases susceptibility to new infections and reactivation of TB [7].
The most common cause of new onset seizures in pregnancy is eclampsia. Eclampsia is seizure of pregnant women with signs and symptoms of pre-eclampsia and without evidence of other cerebral conditions. But eclampsia can present even without the signs and symptoms of pre-eclampsia.
When eclampsia is not controlled or in the presence of atypical features, imaging of the brain should be considered to rule out other causes [8,9].
We presented a case of new onset seizures in pregnancy due to tuberculoma. Our patient was initially diagnosed to have left parietal lobe lacunar infarct based on the MRI brain. But ischemic stroke presenting only with seizures is rare. Even then she was evaluated for young stroke and could not reveal any positive finding. A repeat Computed Tomogram (CT) was done after delivery for further investigation, which showed ring enhancing lesion in left frontal lobe and diagnosis of tuberculoma was made. Intracranial tuberculoma can behave like space occupying lesions and can present with headache, seizures, neurological deficits and even behaivoural problems due to raised intracranial pressure. Seizures are one of the commonest symptoms present in around 85% of cases along with headache and papilloedema [7].
Intracranial tuberculoma can present as new onset seizures in pregnancy. But in majority of cases, the initial diagnosis made was other causes for seizures in pregnancy similar to our case due to the absence of any evidence of pulmonary involvement. Diagnosis may be delayed due to nonspecific clinical manifestations that progress slowly and due to low sensitivity of Acid-Fast Bacilli (AFB) smear on extrapulmonary specimens. A woman from India showed similar presentation as new onset of seizures in pregnancy, which was thought to be brain tumour from neuro imaging. But it turned out to be tuberculoma in histopathological examination following surgical decompression by excision after delivery [10].
Sendhil Coumary Arumugam et al reported a case of term pregnant women with new onset seizures in early labour. She was started on Pritchard regimen with the diagnosis of eclampsia. Since blood pressure and urine protein remained normal, atypical eclampsia diagnosis was made. But fund us examination showed bilateral papilloedema. Postnatal evaluation led to the diagnosis of giant tuber culoma without any pulmonary involvement and she was started on anti-tubercular drugs [11].
Tuberculoma can also be present as a part of disseminated TB. Abnormal neurologic involvement in patients made the diagnosis of intracranial lesion, for which further evaluation reached the final diagnosis of pulmonary TB with central nervous system involvement. A 19 years old Somali refugee presented in the second trimester of pregnancy with four weeks history of gradual right-sided sensomotoric hemisyndrome including facial palsy, ptosis and double vision. She also had hilar lymphadenopathy with brain imaging revealing a solitary brainstem lesion. The diagnosis of disseminated tuberculosis with tuberculoma was made. Anti-tubercular treatment started and patient had neurological improvement and a favourable pregnancy outcome [7].
A standard course of anti-tubercular treatment involves 2HRZE and 4HR (H-isoniazid, R-rifampicin, Z-pyrazinamide and E-ethambutol). Continuation phase can be continued for 9-12 months for central nervous system involvement. Tuberculom as grow slowly and become encapsulated. Perilesional secondary granulomatous vasculitis associated with occlusion of the vessel lumen can be induced by immunological reaction, which can further hinder the penetration of drugs in to the lesion and delays the complete recovery. So, longer duration of treatment may be required in some cases which can affect the prognosis of tuberculoma [11,12].
Declarations
Conflicts of interest: The authors have no conflicts of interest relevant to this article.
Declaration of interests: None.
Funding/Support: Nil.
Acknowledgements: Nil.
References
- Hart LA, Sibai BM. Seizures in pregnancy: Epilepsy, eclampsia, and stroke. Semin in Perinatol. 2013; 37: 207-224.
- Ma JG, Yadav S, Kaplan PW, Johnson E. New-onset epilepsy in women with first time seizures during pregnancy. Seizure. 2020; 80: 42-45
- Beach RL, Kaplan PW. Seizures in pregnancy: Diagnosis and management. Int Rev Neurobiol. 2008; 83: 259-271.
- Malhotra A, Malhotra M. Giant cerebral tuberculoma in pregnancy: Review of literature discussion. Int Surg J. 2016; 3: 386-389.
- Namani S, Dreshaj S, Berisha AZ. Tuberculous meningoencephalitis associated with brain tuberculomas during pregnancy: A case report. J Med Case Reports: 2017; 11.
- World Health Organization (WHO). 2015. Tuberculosis. http://www.who.int/mediacentre/factsheets/fs104/en/.
- Muin DA, Wagner K, Burian R, GhaemMaghami N, Lapaire O, et al. Brainstem Tuberculoma in Pregnancy. Case Rep Obstet Gynecol. 2015; 2015: 179483. https://doi.org/10.1155/2015/179483
- Kshirsagar PC, Acharya NS, Acharya S, Tembhare A. Seizures in Pregnancy- A Rare Case of Neurocysticercosis Mimicking Eclampsia. Journal of Evolution of medical and Dental Sciences. 2020; 9: 1012-1014.
- Sibai BM, Fairlie FM. Eclampsia. In: Gleicher N. Principles and practice of medical therapy in pregnancy. 2nd ed. New York: Appleton & Lange. 1992: 880-888.
- Sujithra Devi R, Priya S, Kumari M, Ramkumar G, Jinkala S, et al. Diagnostic Challenges in Cerebral Tuberculoma Presenting with Seizures in Pregnancy. Obstetric Medicine. 2022. https://doi.org/10.1177/1753495X221078695.
- Arumugam SC, Murugesan S, Pradeep S, John L, Kolluru V, et al. Intracranial Tuberculoma Presenting as Atypical Eclampsia: A Case Report. J Clin Diagn Res. 2016; 10: QD01-2.
- World health organization. Treatment of tuberculosis: Guidelines, 4th edition. 2010. https://apps.who.int/iris/handle/10665/44165